
Abstract
A hernia is defined as an abnormal protrusion of a viscus, or part of a viscus, through the wall of its containing cavity. A hernia can therefore occur at many anatomical locations. Abdominal wall hernias are a common problem and prevalence of this condition has been estimated as approximately 2% for all ages. This review will concentrate on abdominal wall hernias, their presentation, diagnosis and management.
The GP curriculum and hernia
GP curriculum statement 15.2 Digestive Problems does not specifically mention hernias but expects GPs to manage primary contact with patients who have digestive problems. This includes the management of symptoms of abdominal pain as well as acute abdominal conditions.
Within the knowledge base, it requires GPs to have an understanding of common and important conditions that may present with abdominal pains, to recognize the acute abdomen and to be aware of secondary care management, including surgical options.
Nomenclature and classification
Abdominal hernias represent a functional failure of the abdominal wall and may occur through areas of normal weakness, for example due to the passage of the spermatic cord or femoral vessels, or an area of abnormal weakness caused by a congenital or acquired abnormality, for example umbilical or incisional hernia. Hernias may therefore be described according to the anatomical site at which they occur (Fig. 1). The most frequently occurring hernia is an inguinal hernia (75%) followed by umbilical (15%) and then femoral (8.5%) hernia.
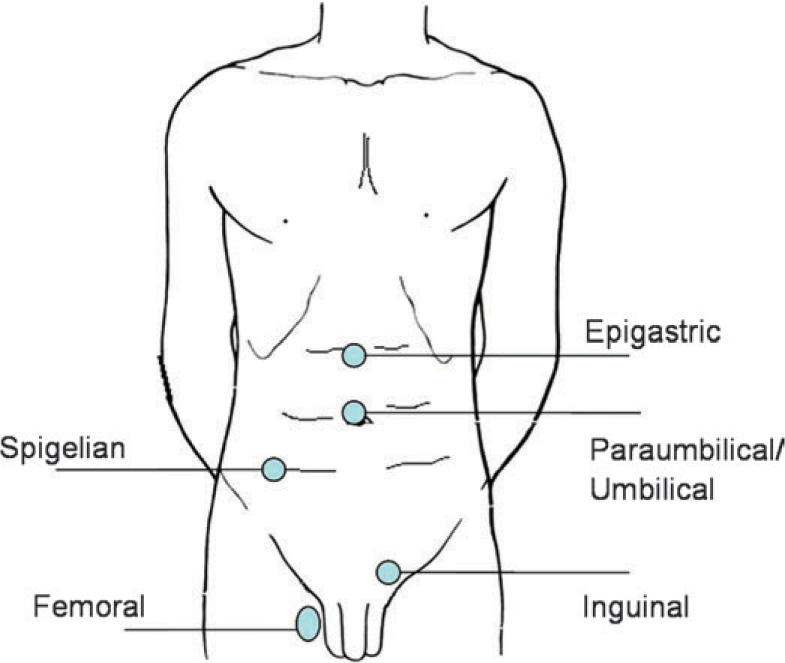
Common abdominal wall hernia sites.
Further to description by anatomical site, hernias may also be described as reducible, incarcerated or strangulated. In a reducible hernia, the contents of the hernia may return spontaneously to the abdominal cavity or can be pushed back by gentle pressure. When a hernia is incarcerated, it is irreducible. An irreducible hernia may present with bowel obstruction and if the blood supply is threatened then it is described as strangulated (Box 1). This requires emergent surgical intervention in order to prevent necrosis of the hernia contents.
Symptoms and signs of hernia strangulation and obstruction
Painful tender hernia Overlying skin may be red Systemic upset (tachycardia and temperature)
Colicky abdominal pain Vomiting (especially if small bowel involved) Abdominal distension Tinkling bowel sounds Irreducible hernia
Note: An incarcerated hernia should not be forcibly reduced as there is a risk of injury to the bowel. In the presence of obstruction, forcible reduction of the hernia may reduce it enmass. This is when the hernia appears reduced but the constricting peritoneal ring remains and has been pushed back inside the abdomen, so that the obstruction is not relieved.
Inguinal hernia
Paediatric inguinal hernia
Inguinal hernias may be congenital and may occur in up to 5% of full-term babies. They occur predominantly in boys (80–90%) and more commonly on the right-hand side although may be bilateral. The hernia may only be apparent when the child is crying or straining and is often noticed by the parents but not obvious on examination in the surgery. The scrotum should always be examined to avoid missing an undescended or retractile testis, although this condition itself often coexists with an inguinal hernia.
There is a high risk of incarceration of infant inguinal hernia, and so refer all suspected cases for elective surgical repair. If the hernia is incarcerated and/or the child is unwell, emergency referral is necessary.
Adult inguinal hernia
This is the most common abdominal hernia with approximately 70 000 inguinal hernia repairs performed annually in England with a cost to the NHS of 56 million pounds a year. Inguinal hernias are 10 times more common in males and up to 30% of people who have a unilateral inguinal hernia will go on to develop a contralateral hernia.
Inguinal hernias can be divided into indirect and direct hernias, with indirect hernias being more common. A direct inguinal hernia protrudes directly through the posterior wall of the inguinal canal. Indirect hernias arise through the deep inguinal ring, which is a natural defect in the abdominal wall that allows the passage of the spermatic cord into the inguinal canal. A large indirect inguinal hernia may enter the scrotum and is then described as an inguinal—scrotal hernia. The internal or deep inguinal ring lies at the midpoint of a line from the pubic tubercle to the anterior superior iliac spine, 1.25 cm above the inguinal ligament. Pressure over this area once the hernia is reduced may keep it reduced. This is the principal behind wearing a truss, a device used to keep the hernia reduced while waiting for surgery or as a more permanent conservative measure for patients who do not want or are unfit for surgery. Trusses may be prescribed on NHS prescription.
Inguinal hernias often present with a lump in the groin which may cause discomfort, especially on physical activity, however, up to a third of patients with a hernia will have no pain. Although inguinal hernias are at risk of incarceration, the risk of strangulation is low (3 in 1000) with only 5% of hernia repairs carried out as an emergency. Examine the patient in the standing and lying positions and consider the differential diagnosis of other groin lumps (Table 1).
Differential diagnosis of groin lumps

Note: An additional differential of an inguinal—scrotal hernia is a hydrocoele, but a hydrocoele should transilluminate.
Treatment of inguinal hernia usually involves surgical repair. It has been suggested that patients with small asymptomatic hernias can be managed by watchful waiting as risk of serious complication from the hernia is low, but it is not clear how many of these patients will go on to develop symptoms and require surgery at a later stage when they have a larger and more technically challenging hernia or when they are older and less fit for surgery. All medically fit patients with inguinal hernia should therefore be referred for consideration of surgery.
Many different methods of hernia repair have been described but the most commonly performed operation in the UK is an open mesh repair (Lichtenstein repair) due to its relative ease of reproducibility and lower recurrence rates than sutured repair. Open mesh repair can be performed as day case surgery and median duration of time off work has been estimated as 7 days (4.5 for office work and 14 days for manual work). Patients should be advised not to perform heavy lifting for approximately 6–8 weeks after the operations. Ismail et al. (2000) demonstrated that there is a wide variety of advice given to patients on driving after groin hernia repair. Evidence suggests that most patients are safe to drive at approximately 1 week, but there may be individual variation in healing and post-operative recovery times that make this a guide only. In general, advice is usually given that the patient must be safe to perform an emergency stop. Motorcycle riders may take longer before they are safe to drive as riding a bike is more physically demanding.
Complications of open mesh repair include pain, wound infection, seroma, haematoma, numbness and recurrence. Scrotal swelling and bruising are common, especially after repair of a large hernia. Moderate to severe chronic post-operative pain can occur in approximately 3% of patients and can have an adverse impact on quality of life. Referral to a pain specialist is indicated in these patients.
Other surgical options include laparoscopic repair, which is associated with less post-operative pain, fewer post-operative complications and a faster return to work. Laparoscopic repair is also associated, however, with increased costs, a longer operative time, increased risk of more major complications such as bowel injury and vessel injury and an increased recurrence rate. In addition, laparoscopic surgery cannot be performed under local anaesthetic. The two main types of laparoscopic repair are the totally extraperitoneal or the transabdominal preperitoneal repairs. Recent NICE guidelines have recommended that the risk and benefits of open and laparoscopic surgery are discussed with patients to allow them to choose between the two (Box 2).
Advantages and disadvantages of laparoscopic as compared to open inguinal hernia repair
Faster return to work by up to 4 days Reduced risk of numbness Reduced risk of wound haematoma/infection Reduced risk of chronic post-operative pain
Increased recurrence rates Increased cost Longer operating time Higher rate of serious complications (particularly visceral or vascular injury)
Umbilical and paraumbilical hernia
Paediatric umbilical hernia
Congenital umbilical hernia may result from the failure of the gut to return to the abdominal cavity at 10 weeks of gestation. This occurs in 1 in 5000 births and is usually associated with other congenital abnormalities. Most cases are detected in utero on antenatal scanning and are managed immediately after the birth, which is usually arranged in a hospital with a specialist paediatric surgical unit.
Infantile umbilical hernias occur in approximately one in five births, with a higher incidence in Afro-Caribbean and Asian infants. Commonly the parents present with a well child in which they have noticed a bulge at the umbilicus which becomes more noticeable every time that the child cries. Spontaneous resolution occurs in up to 90% of cases by 2 years of age. If the hernia is present beyond 5 years of age, it is likely to persist and the child should be referred for surgical management. Large defects are less likely to resolve spontaneously and should be referred for treatment earlier. Other indications for surgery include development of tenderness or pain over the hernia, which may represent the development of complications.
Paraumbilical and adult umbilical hernia
Paraumbilical hernias occur five times more frequently in females than males and are more commonly seen over the age of 35. Presenting features may involve intermittent pain and the patient may complain of a bulge at the umbilicus. Paraumbilical hernias are acquired hernias of the abdominal wall and arise at the edge of the umbilicus. Small hernias may only contain preperitoneal fat whereas larger hernias are likely to contain bowel and patients may suffer with intestinal colic as the hernia intermittently obstructs. They tend to progress over time and are at high risk of incarceration and strangulation, so referral for surgical repair is always indicated.
Adult umbilical hernias are more commonly seen in female multi-parous patients although are also seen in patients with chronically raised intra-abdominal pressure (e.g. in patients with ascites). They are often symptomatic and have increased risk of incarceration, and so require referral for surgical intervention if the patient is fit enough.
Femoral hernia
Femoral hernias are four times more common in women than men, accounting for up to 20% of female hernias. Despite this, inguinal hernias are still more common in women than femoral hernia.
The femoral canal lies medially to the femoral vein below the groin crease. A femoral hernia may be felt as a lump below and lateral to the pubic tubercle, as opposed to an inguinal hernia which is generally felt above and medial to the pubic tubercle. However, as small inguinal hernias may be felt lateral to the pubic tubercle, and rarely femoral hernias may be felt above the inguinal ligament (Fig. 2), diagnosis can be difficult. Hair et al. (2001) carried out a small study in Glasgow that demonstrated medical staff of all grades were poor at making a preoperative diagnosis of femoral hernia.

An inguinal hernia emerges above and medial to the pubic tubercle, a femoral hernia is felt below and lateral.
Due to the narrow neck of the femoral canal, the risk of strangulation is high and up to 40% of femoral hernia present as an emergency with signs of strangulation or obstruction. Therefore, a suspected femoral hernia should always be referred for surgical repair.
Epigastric hernia
Epigastric hernias are hernias in the upper midline of the abdomen. They are relatively common, with post-mortem studies suggesting a prevalence of up to 10%. They are four times more common in men than women and the majority are asymptomatic. When symptomatic, pain or discomfort is the usual feature. In adults, the decision to offer surgery is based on the severity of symptoms and there is a 5–10% recurrence rate.
Other hernia
Incisional hernia
Incisional hernia occurs as a result of breakdown of the muscle closure in an abdominal wound some time after surgery. There may be a history of wound sepsis, haematoma or breakdown. Incisional hernias present with a bulge at the site of the operation scar. This may be associated with some discomfort. The hernia is usually visible when the patient stands, and it can be made more obvious by asking the patient to cough or straight leg raise while lying flat. The margins of the muscular defect are palpable under the skin. Note whether the hernia is fully reducible or not.
Often reassurance suffices. If the hernia is obstructed, strangulated or causing discomfort, then refer for surgical assessment.
Spigelian hernia
A spigelian hernia is a rarer abdominal wall hernia. A hernial sac protrudes lateral to the rectus sheath midway between umbilicus and pubic bone. It presents with discomfort and sometimes also vomiting and signs of obstruction. Always refer for surgical repair, as an emergency if any signs of strangulation or obstruction.
Key points
Abdominal wall hernias are a common problem Most hernia, with the exception of paediatric umbilical hernia, will not resolve spontaneously and will therefore need referral for repair Strangulated or obstructed hernias are a surgical emergency