
Abstract
Endocarditis is the inflammation of the endocardium (the inner lining) of the myocardium and the heart valves. Endocarditis is a rare condition and is most commonly infective, resulting in significant mortality and morbidity from both intracardiac and systemic effects. Endocarditis occasionally presents as an acute and fulminating disease, but more often, it presents insidiously. The term ‘infective endocarditis’ (IE) is now preferred to the previously used ‘bacterial endocarditis’ as not all the infecting organisms are bacterial.
The GP curriculum and endocarditis
outlines the general practitioners' role in recognition, management and prevention of cardiovascular problems. It states specifically
Cardiovascular problems are an important cause of morbidity and mortality Management of the risk factors for cardiovascular problems is an essential part of health promotion activity Accurate diagnosis of symptoms that may be potentially due to cardiovascular problems is a key competence of general practice
Recognize and evaluate acutely ill patients Take responsibility for a decision to admit an acutely ill person and not be unduly influenced by others, such as secondary care doctors who have not assessed the patient
With regards to the recent change in policy on antibiotic prophylaxis of endocarditis,
Epidemiology
The annual incidence of infective endocarditis (IE) in the UK is low—less than 10 per 100 000 people per year. IE increases with age and is more common in men with a male to female ratio of 2 : 1.
There has been little change in the prevalence of IE over the last 40 years. Until the late 1970s, damage to valves from rheumatic heart disease, congenitally abnormal valves and other congenital heart abnormalities (e.g. ventricular septal defects causing an intracardiac shunt) were the major risk factors for developing IE.
Since the reduction in rheumatic heart disease in the developed world in the latter part of the 20th century, other risk factors have emerged—the development and increase in the use of prosthetic valves, an ageing population leading to an increased incidence of sclerotic heart disease, intravenous drug use and invasive medical procedures causing bacteraemia. NICE have recently provided guidance on which congenital and/or structural heart defects should be considered risk factors for IE (see Box 1). However, it is important to note that IE can also occur on structurally normal valves without any other risk factors.
NICE guidelines for antibiotic prophylaxis in IE
Health care professionals should regard people with the following cardiac conditions to be at increased risk of developing IE:
Acquired valve heart disease with stenosis or regurgitation Valve replacement Structural congenital heart disease, including surgically corrected or palliated structural conditions, but excluding isolated atrial septal defect, fully repaired ventricular septal defect or fully repaired ventricular septal defect and closure devices that are considered to be endothelialized Hypertrophic cardiomyopathy Previous IE
Pathophysiology
In IE, colonization of the organism on the endocardium and subsequent systemic infection is a complicated process. It can be caused by numerous different pathogens during the presence of circulating bacteraemia (see Box 2).
Causative organisms in IE
These are the most common organisms causing IE, with Streptococcus viridians being most frequent. These organisms are part of the normal bacterial flora of the mouth, larynx and pharynx. Hence, gingival infection, invasive dental procedures and bronchoscopy can lead to IE.
As part of skin flora, staphylococcal IE tends to originate from cellulitic infections or abscesses. It is more commonly seen in intravenous drug users and in patients with central venous catheters. Staphylococcus aureus and Staphylococcus epidermis are the two common pathogens. Acute IE is more likely to be due to a Staphylococcal source.
As part of the bacterial flora of the bowel and perineal region, pelvic surgery or instrumentation can lead to IE.
Organisms such as the HACEK group (Haemophilus species, Actinobacillus/Actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens and Kingella), Legionella, Coxiella, Brucella and certain fungi are other pathogens more common in intravenous drug abusers, alcoholics and the immunosuppressed. These account for less than 5–10% of cases of IE. These organisms need specific requirement to be cultured and are therefore considered fastidious. They are sometimes the cause of ‘culture-negative’ endocarditis.
The predisposing lesions are thought to be microulcerations on the endocardial surface exposing the underlying tissue to blood. This promotes tiny clot formation upon which organisms can attach. Once the infecting organism has been established on the endocardial surface, platelet aggregation and fibrin deposition occur which facilitate the pathogen to multiply and ‘stick’ to the lesion. The resulting mass is known as a ‘vegetation’ (Fig. 1).

Vegetations visible on the aortic valve in two places. From the University of Alabama at Birmingham, Department of Pathology, PEIR Digital Library (http://peir.net).
Organisms initially colonize the edges of the valve. Vegetations are more common on left-sided regurgitant valves, although in intravenous drug users the right-sided valves are predominantly affected. Shunt lesions such as ventricular septal defects tend to develop vegetations on the low-pressure side of the shunt. The virulent pathogens can spread and invade the valve cusps rapidly causing valvular destruction and regurgitation.
The extra-cardiac features (Box 3) of IE are caused by two different phenomena:
Embolic—septic emboli (fragments breaking off from the vegetation) can involve any circulation (e.g. brain and lungs) and are seen in 20–45% of patients. These septic emboli not only cause localized ischaemic effects such as stroke or pulmonary embolism but can also cause a distant infection, although this is uncommon as the causative organisms are minimally invasive.
Immunological—the levels of agglutinating and complement-fixing bactericidal antibodies and cryoglobulins are increased in IE. These circulating immune complexes can be deposited in peripheral vessels causing a range of phenomena.
Presentation
The clinical features of IE are summarized in Box 3
Subacute IE
The presentation of IE is insidious and the clinician must always be alert to the possibility of IE as a possible diagnosis. The features of IE include
Low-grade pyrexia Weight loss Night sweats Fatigue Myalgia and/or New heart murmur
Alternatively, the presentation may be of a complication of the illness, for example renal failure or symptoms of cardiac failure.
Acute IE
The presentation of acute IE is of a florid and rapidly progressive illness. Features include
High-grade pyrexia Systemic inflammatory response to sepsis, in the form of fever, tachycardia and hypotension and/or Severe heart failure due to rapid valve destruction or chordae tympani rupture
Clinical features of IE
Murmur—signs of a previous underlying heart disease may be present. The presence of a new murmur or a change in the existing characteristics of a murmur should alert the clinician to the possibility of IE. Congestive cardiac failure (CCF)—symptoms and signs of cardiac failure, for example orthopnoea and peripheral oedema Palpitations/tachycardia—interference with the conduction system can cause arrhythmias Heart block—often occurring in the presence of aortic root abscess, which causes a physical disruption to the atrioventricular node Pericarditis
Brain—stroke, mycotic aneurysms (infected cerebral aneurysms that can occur after the IE has been treated) Limbs—acute limb ischaemia Coronary—myocardial infarction Renal—haematuria, renal failure Spleen—hyposplenism Lung—pulmonary infarction
Skin
Osler's nodes—lesions resulting from immune complex deposition causing hard tender subcutaneous swellings in the hands and feet, particulary the finger pulps. (Fig. 2) Janeway lesions—non-tender, macular erythematous blanching lesions found on the thenar and hypothenar eminence Splinter haemorrhages—seen as red, linear lesions in the nail bed (Fig. 3) Petechiae—these can occur secondary to vasculitis at a variety of sites including the conjunctivae, oral mucosa and soft palate. When occurring on the retina, they are termed Roth's spots.

Osler's nodes.

Splinter haemorrhages.
Renal
Glomerulonephritis—due to vasculitis Acute renal failure
Joints
Subacute IE can cause a sterile oligoarthritis.
Spleen
Splenomegaly occurs most commonly in patients with long-standing subacute disease.
Others
Neurological Clubbing—rare now as it is a late sign
Prosthetic valve IE
The clinical features of prosthetic valve endocarditis are similar to those of a native valve endocarditis. Emboli are common and CCF tends to be more severe as valve ring vegetations can cause severe stenosis as well as regurgitation. Prosthetic valve endocarditis is classified as ‘early’, which is due to infection of the prosthetic valve during or immediately after the surgical procedure and usually presents within 2 months of the surgery, or ‘late’ when IE is due to systemic bacteraemia.
IE in intravenous drug users
Intravenous drug users with IE often present with florid right-sided endocarditis. The origin of bacteraemia is usually skin abscesses at the site of intravenous drug self-injection. Pathogens include staphylococcus but also fungi and other fastidious organisms. These patients can be difficult to manage as they have poor venous access and a high-risk lifestyle leading to poor concordance with treatment during the illness and reduced likelihood of risk avoidance after recovery.
Secondary care investigations in suspected IE
Haematology—normocytic normochromic anaemia and a raised erythrocyte sedimentation rate (ESR). A thrombocytopenia can be present.
Biochemistry—raised C-reactive protein (CRP). Renal failure is commonly present to varying degrees and liver function tests can be mildly disturbed.
Urine—frequently displays microscopic haematuria on dipstick examination and proteinuria can also be present
Blood cultures—are the most important test in making the diagnosis of IE. A minimum of three sets of blood cultures taken from different venepuncture sites an hour apart are needed to demonstrate continuous bacteremia. Special medium or prolonged incubation may be needed for certain organisms, for example Brucella.
Serological tests—are needed for detecting Coxiella, Chlamydia and Brucella
Immunology—there is a polyclonal elevation in serum immunoglobulins and a decrease in circulating complement due to immune complex formation
Transthoracic echocardiography is non-invasive and detects vegetations greater than 2 mm diameter in 60% of native valve IE, but is not as accurate with prosthetic valves
Transoesophageal echocardiography is invasive but detects 90% of all vegetations. It is particularly useful for right-sided and prosthetic valve lesions, which can be small and difficult to visualize with transthoracic echocardiography.
Echocardiography is useful for predicting complications such as embolization. Risk factors include
Vegetations over 10 mm in diameter Multiple vegetations Pedunculated vegetations Prolapsing vegetations
Investigations
In primary care, if endocarditis is suspected, a same day referral to cardiology or the on-call medical team is warranted. Do not delay to perform investigations. Possible investigations to consider in a secondary care environment are summarized in Box 4.
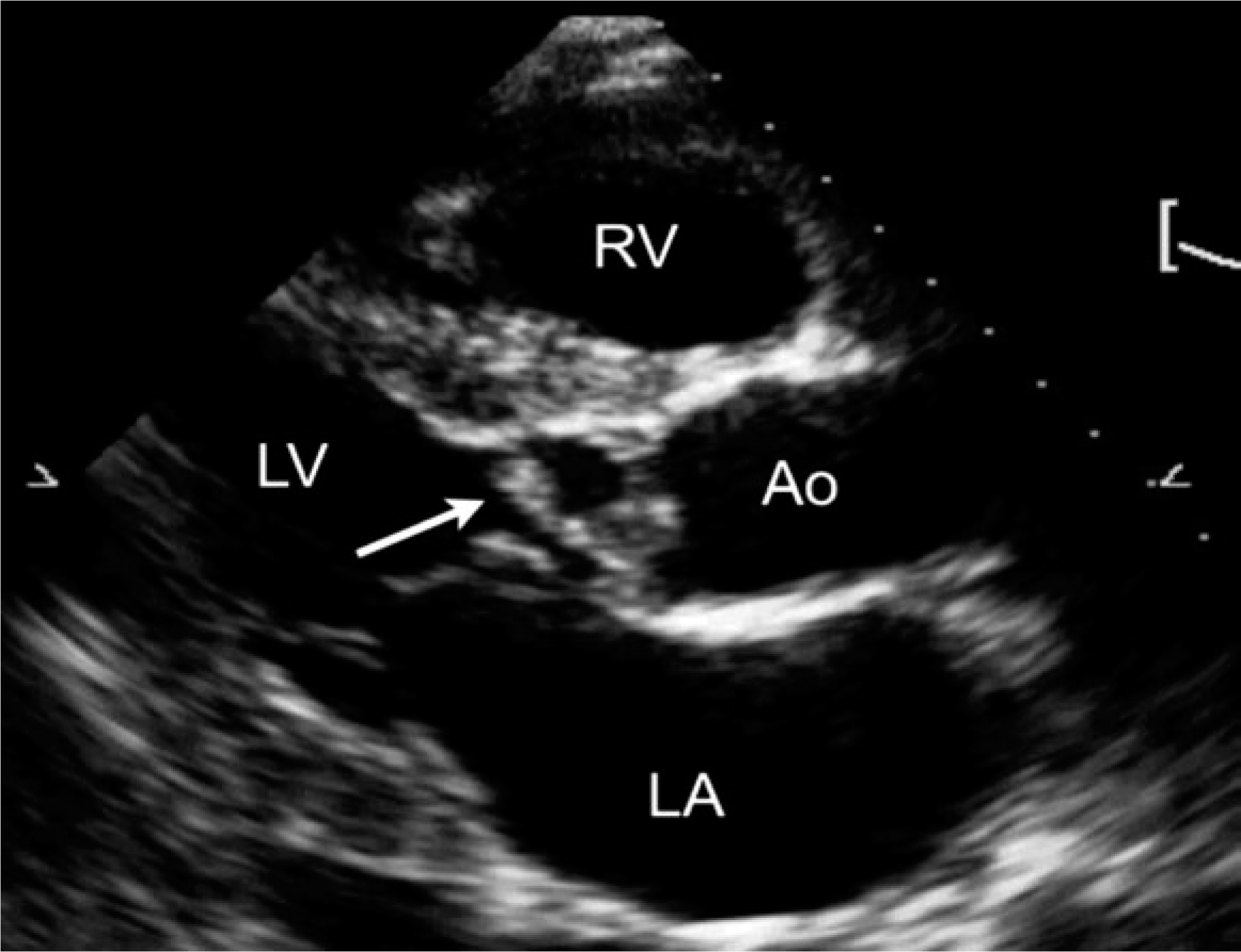
Transthoracic echocardiogram—parasternal long axis view showing a vegetation (arrow) on the aortic valve. LA, left atrium; LV, left ventricle; RV, right ventricle; Ao, aorta. From: Jassal et al. Cardiovascular ultrasound (2007) 5: 20. Jassal et al. (2007); licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution and reproduction in any medium, provided the original work is properly cited.
Diagnosis
As the presentation can often be vague, practitioners should always be alert to the possibility of IE in those patients presenting with combinations of pyrexia of uncertain origin, bacteraemia and predisposing cardiac lesions. The ‘Duke's Criteria’ have been developed to aid diagnosis (see Box 5).
Treatment
Treatment of IE is always secondary care led.
Medical
Antibiotic therapy is an important aspect of treatment in IE. Antibiotic choice should be tailored to the individual patient depending on the identified organism and local resistance profiles (see Table 1). Microbiologist's advice should be sought in all cases.
Suggested antibiotic regimes for IE
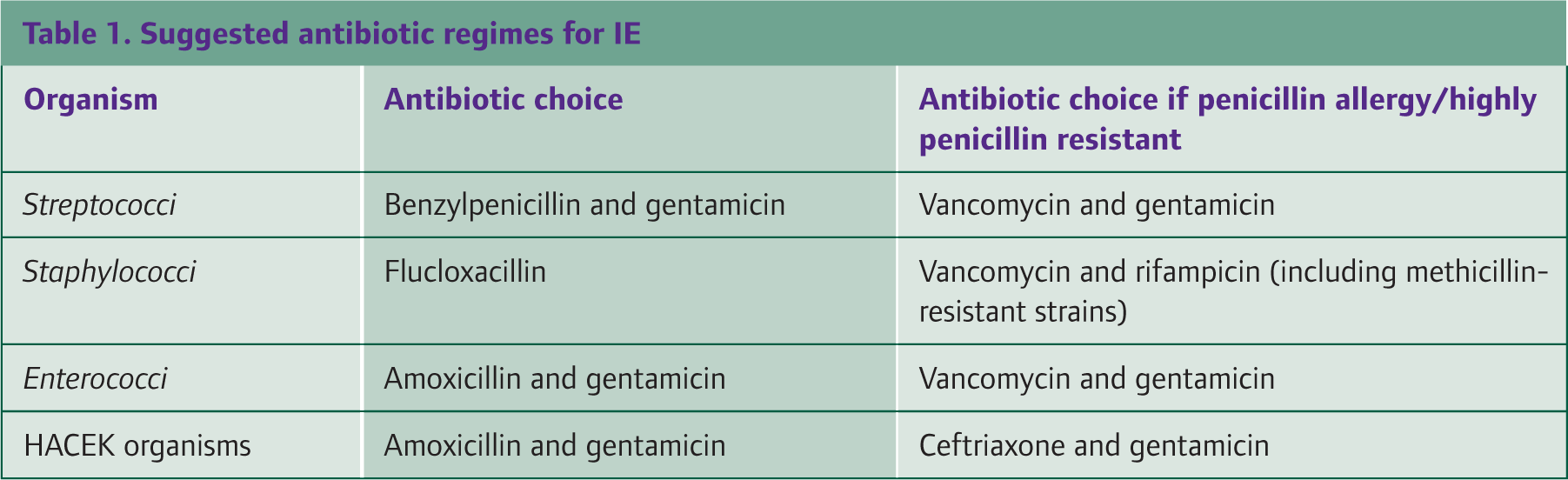
The duration of antibiotic treatment will vary with the type of infection—acute or subacute presentation, the presence of other complications and the nature of the infecting organism. Most cases will require a minimum of 6 weeks of antibiotics. In some cases, oral treatment can be considered after 2 weeks of intravenous treatment.
After the initial blood cultures have been taken, it is necessary to start ‘blind’ antimicrobial treatment while awaiting the results. The British National Formulary suggests initial treatment with flucloxacillin or benzylpenicillin and gentamicin, but this can be altered depending on the presentation, which will often give a clue as to the underlying organism. For example, a florid presentation of IE in a person who uses intravenous drugs may indicate a staphylococcal source. The antibiotic regime is then adjusted as needed once culture and sensitivity results are available. Advice should always be sought at all stages from the local microbiology department.
Duke's criteria for the diagnosis of IE
Major criteria
Positive blood culture
Typical IE organism in two positive blood cultures Persistently positive blood culture
Evidence of endocardial involvement on echocardiography
Vegetation visualized with no alternative explanation Abscess Partial dehiscence of prosthetic valve New valvular degeneration
Minor criteria
Predisposing cardiac condition Intravenous drug use Pyrexia greater than 38°C Vascular lesions, for example Janeway lesions Immunological lesions, for example glomerulonephritis Positive blood cultures but not meeting major criteria Positive serology Echocardiogram suggestive of IE but not meeting major criteria
Culture-negative IE can pose a significant management problem to clinicians. Administration of antibiotics prior to taking blood cultures can cause a negative result, or it may be the fastidious nature of the organism that makes culture difficult (e.g. Legionella or fungi). In these cases, serological testing is particularly useful. The benefits of stopping antibiotic treatment in these patients and taking subsequent repeat blood cultures to try to identify the infecting organism must be weighed against the risk of deterioration in clinical condition as a result of a break in treatment.
Surgical
Surgery for IE can be a life-saving procedure but needs to be correctly timed to avoid further complications. The timing will be dependent on the haemodynamic stability of the patient, whether the infection is successfully treated or becomes persistent, and the presence of complications that necessitate surgery. Discussions with cardiothoracic surgeons regarding surgery should take place early in the appropriate setting. The following are situations, in which surgery might be considered:
Moderate-severe progressive heart failure causing haemodynamic compromise Unstable prosthesis Persistent uncontrolled infection Large vegetations that are hypermobile Infection of prosthetic material Embolization Perivalvular extension of the infection
Monitoring during treatment
Clinical features
Persistent pyrexia and systemic symptoms or resurgence of fever may suggest that the antibiotic treatment is inadequate, there is a concomitant infection (e.g. line sepsis) or it may indicate a drug reaction
Laboratory tests
Inflammatory markers—CRP and ESR—should be carried out on a twice-weekly basis to judge response to treatment. Renal function should also be monitored regularly as renal insufficiency is very common in IE and can occur at any stage in the illness. A rising haemoglobin and a falling white cell count (to within the normal range) suggests successful treatment.
Microbiology
Antibiotic levels when using vancomycin or gentamicin are appropriate to ensure the treatment is falling within the therapeutic window. Back titration can be performed on antibiotic levels to ensure sufficient bactericidal activity is present.
ECG
Daily ECGs should be carried out, looking specifically for the presence of arrhythmias or conduction deficits.
Echocardiography
Regular (weekly) echocardiography can identify progressive valve destruction or abscess development that may not be clinically apparent.
Non-infective causes of endocarditis
Non-infective causes of endocarditis are much rarer than infective causes. Libman—Sacks endocarditis is a non-IE associated with systemic lupus erythematosus (SLE). Circulating immune complexes formed in SLE can become attached to cardiac valvular tissue and attract platelets and fibrin causing a sterile vegetation. These do not often cause significant regurgitation. It is found in up to 40% of SLE patients at autopsy.
Marantic endocarditis is a non-IE that occurs in chronic wasting illnesses, such as the latter stages of malignancy. The vegetations tend to be small and the reason for their development is unclear. Complications include bacterial colonization of these vegetations and the development of a subsequent IE. These sterile vegetations also have a propensity to embolize but alone cause few intracardiac effects.
Prevention of IE
Until 2008, it was standard practice to consider any cardiac lesion a risk factor for IE and to offer all such patients antibiotic prophylaxis prior to interventional procedures, including non-invasive dental procedures such as scaling. In March 2008, NICE released new guidance for prophylaxis against IE. This guidance provides clinicians with clear advice on which cardiac lesions put patients ‘at risk’ from IE (see Box 1) and gives evidence-based advice regarding antibiotic prophylaxis (see Box 6).
The important message from this new guidance is that antibiotic prophylaxis solely to prevent IE should not be given to at-risk patients undergoing interventional procedures. The basis to this guidance is that
There is no consistent association between having an interventional procedure (dental or non-dental) and developing IE Simple daily activities such as regular toothbrushing almost certainly present a greater risk of IE than a single dental procedure due to repetitive exposure to bacteremia The clinical effectiveness of antibiotic prophylaxis is not proven Antibiotic prophylaxis for dental procedures may lead to a greater number of deaths through fatal anaphylaxis than a strategy of no prophylaxis, which is neither clinically nor cost-effective
NICE guidelines for antibiotic prophylaxis for endocarditis
Health care professionals should offer people at risk of endocarditis clear and consistent information about prevention, including
The benefits and risks of antibiotic prophylaxis and an explanation of why antibiotic prophylaxis is no longer routinely recommended The importance of maintaining good oral health Symptoms that may indicate IE and when to seek expert advice The risks of undergoing invasive procedures, including non-medical procedures such as body piercing or tattooing
Antibiotic prophylaxis against IE is not recommended for people undergoing dental procedures or for people undergoing non-dental procedures at the following sites:
Upper and lower gastro-intestinal tract Genito-urinary tract, this includes urological, gynaecological and obstetric procedures and childbirth Upper and lower respiratory tract, this includes ear, nose and throat procedures and bronchoscopy
Any episodes in patients at risk of IE should be investigated and treated promptly to reduce the risk of endocarditis developing.
If a person at risk of IE is receiving antimicrobial therapy because they are undergoing a gastro-intestinal or genito-urinary procedure at a site where there is a suspected infection, the person should receive an antibiotic that covers organisms that cause IE.
Relevance to general practice
Despite the fact that IE is almost exclusively investigated, diagnosed and managed in a secondary care setting, the initial presentation of the patient with IE (particularly subacute IE) is often to the GP. As the diagnosis is uncommon and the presentation vague with no clearly defined or pathognomonic features, IE may not initially spring to mind when considering a differential diagnosis. However, delayed diagnosis and management can result in a poorer outcome for the patient. It is therefore important for general practitioners to have a degree of up to date knowledge on the features of IE and the risks factors that predispose individuals to developing IE to aid timely referral for secondary care investigation.
Along with patients who have certain structural abnormalities of the heart, patients who have had a previous episode of IE are considered at higher risk of developing IE. GPs should help these patients to minimize their risk of developing IE by promoting self-care (see Box 6).
Additionally, due to the revised antibiotic prophylaxis guidelines, there is a large cohort of patients with structural cardiac abnormalities who are facing a change in their established management in terms of IE prophylaxis. GPs have an important role to play in introducing them to the revised guidelines on antibiotic prophylaxis and explaining the reasons for that change.
Key points
Endocarditis is a rare but serious condition, with a high mortality. It often has an insidious presentation, so clinicians need to maintain a high level of suspicion of IE, particularly in patients with underlying risk factors. Risk factors for IE include structural heart disease, previous IE, valve prosthesis, hypertrophic cardiomyopathy, intravenous drug use and other causes of significant bacteremia (including iatrogenic) The suspicion of IE should prompt immediate referral for investigation and management Antibiotic administration solely to prevent IE should no longer be given for interventional dental and non-dental procedures but if the patient is receiving antibiotics for suspected infection at sites of gastro-intestinal/genito-urinary procedures, the antibiotics should cover IE organisms Individuals at increased risk of IE need to be able to have a thorough discussion with their clinician about what they can do to reduce their risk of IE, seeking early advice for signs and symptoms of infection and why the advice on antibiotic prophylaxis has changed