
Abstract
Peripheral neuropathy is defined as dysfunction of the structure and function of peripheral motor, sensory and autonomic nerves. Although many individual causes of peripheral neuropathy are rare, it is estimated that up to 8% of the population have some degree of peripheral neuropathy or a total of 4.7 million people in the UK alone. There are many different types of peripheral neuropathy but the most common cause is diabetes and up to 60% of diabetic patients have a peripheral neuropathy of some sort. Peripheral neuropathy not only causes problems with everyday functioning but also in many cases causes severe, disabling neuropathic pain. This article aims to provide a simple overview of peripheral neuropathy and its management in primary care.
The GP curriculum and peripheral neuropathy
Neuropathy features as a symptom in the knowledge base of curriculum statement 15.7: Neurological problems. The knowledge base also lists as common and important conditions:
Mononeuropathies—trigeminal neuralgia, Bell's palsy, carpal tunnel syndrome and nerve entrapments, for example ulnar, sciatic and femoral nerves and Polyneuropathies—metabolic causes (diabetes alcohol, vitamin B12 and folate, porphyria, uraemia), infectious causes (e.g. Guillain-Barré, postviral, HIV), drug-induced neuropathy
GPs are required to manage primary contact with patients who have a neurological problem; coordinate care with other primary care health professionals, such as occupational therapists, physiotherapists and district nurses to enable chronic disease management and rehabilitation and describe the indications for referral to a neurologist for chronic conditions requiring ongoing specialist management and conditions that are irreversible without early treatment (e.g. ulnar nerve entrapment).
In addition, GPs should demonstrate empathy and compassion towards patients with incurable disabling neurological conditions. This includes recognition that neurological conditions often affect patients during their working lives and consequently have a large impact on the family's social and economic well-being.
Mononeuropathy
A mononeuropathy results from damage to an individual peripheral or cranial nerve. The most common causes of mononeuropathy are trauma, compression or diabetes. Table 1 lists some common peripheral mononeuropathies that you might see in the surgery.
Common peripheral mononeuropathies

If more than one peripheral nerve is affected in different parts of the body, the term ‘mononeuritis multiplex’ is used. Mononeuritis multiplex tends to be caused by systemic disease such as diabetes, sarcoid, cancers, polyarteritis nodosum or amyloid, although in one in three cases, no cause is ever identified.
Carpal tunnel syndrome
Carpal tunnel syndrome results from compression of the median nerve as it passes under the flexor retinaculum (Fig. 1). It may be associated with pregnancy, hypothyroidism, obesity or carpal arthritis but often occurs with no obvious cause.

Carpal tunnel syndrome.
Patients present with pain in the radial three-and-a-half digits of the hand, sometimes with associated numbness or pins and needles, weakness and thenar wasting. Symptoms tend to be worse at night and are improved by shaking the wrist.
On examination, Phalen's test—hyperflexion of wrist for 1 minute (Fig. 2)—triggers symptoms. Tinel's test—tapping over the carpal tunnel—causes paraesthesiae. Neither of these tests is particularly reliable, so request nerve conduction studies if clinical diagnosis is in doubt.
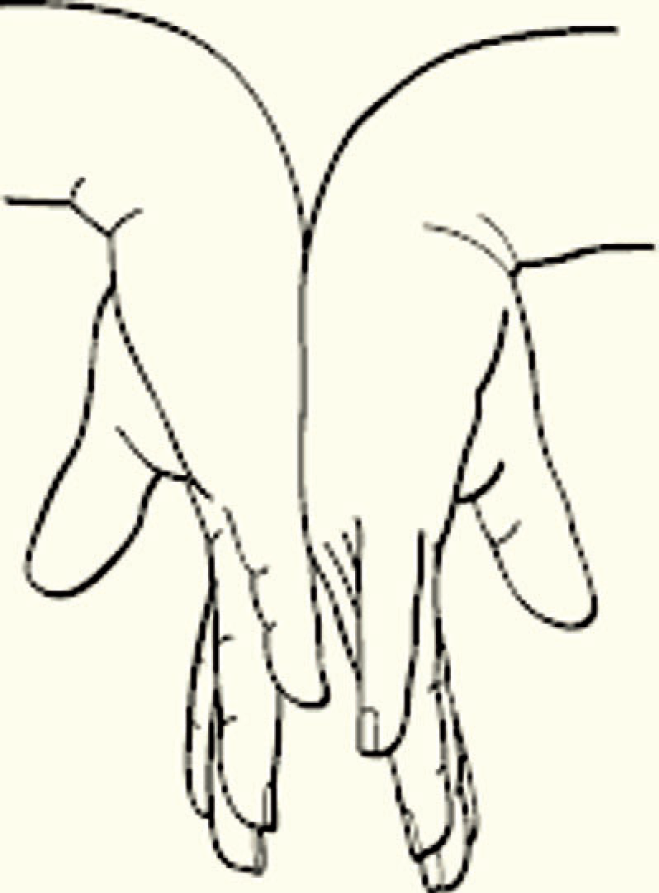
Phalen's test for carpal tunnel syndrome.
In general practice, night splints may help as may a carpal tunnel steroid injection. These can be purchased from surgical suppliers or obtained via physiotherapy or occupational therapy departments. Do not attempt carpal tunnel injection unless you have been properly trained to carry out the procedure as injections performed incorrectly can result in median nerve damage. Injections and splints are less likely to be effective if the patient is over the age of 50 or symptoms have been present for more than 10 months.
If GP treatment fails, you do not feel confident to inject the carpal tunnel, or if there is constant paraesthesiae and/or triggering of fingers, refer to orthopaedics or rheumatology depending on local protocols. Surgical treatment involves division of the flexor retinaculum.
Ulnar neuritis
Narrowing of the ulnar grove (from osteoarthritis, rheumatoid arthritis or after a fracture) causes pressure on the ulnar nerve leading to ulnar neuropathy. Clumsiness with the hand is often the first symptom, then weakness. There may be wasting of hand muscles innervated by the ulnar nerve and reduced sensation in the little finger and medial half of the ring finger. Rule out metabolic and autoimmune causes of a mononeuritis and refer for consideration of nerve conduction studies or directly to orthopaedics for surgical decompression if entrapment is likely.
Bell's palsy
Bell's palsy was named after Scottish anatomist and surgeon Sir Charles Bell (1774-1842). A Bell's palsy is a unilateral facial nerve palsy, affecting the left side of the face with the same frequency as the right and without other signs (Fig. 3). It is the most common acute mononeuropathy with a lifetime incidence of 1 in 65 and tends to affect young adults with a peak age of incidence in the range 10–40 years. The cause is unknown although a viral aetiology has been widely proposed.

Bell's palsy affecting the left side of the face. Dr P. Marazzi/Science Photo Library.
Symptoms are usually of sudden onset with partial or complete paralysis of one side of the face appearing over a time period of less than 24 hours but may be preceded by pain around the ear. Apart from facial weakness, other possible symptoms include reduced noise tolerance, facial numbness and disturbed taste on the anterior part of the tongue.
Around 70% of patients who suffer a Bell's palsy recover completely; 13% have insignificant sequelae; but the remainder have permanent deficit. Most (in excess of 85%) improve spontaneously within 3 weeks of the onset of symptoms. All patients should be advised to protect the affected eye by taping the lid shut and wearing a protective eye pad at night. Glasses should be worn in the day and consider supplying artificial tears if the eye is drying.
Drug management is controversial. Both prednisolone and aciclovir have been used for the treatment of acute Bell's palsy but Cochrane reviews have not shown any conclusive benefit for either. However, one study (Sullivan et al., 2007) has shown benefit from steroid treatment with prednisolone 25 mg twice daily for 10 days but only if started within 72 hours of the onset of symptoms.
Refer for ear, nose and throat, ophthalmology or neurology review as appropriate if
recovery is not starting after 3 weeks (to ear, nose and throat or neurology) complete or long-standing palsy for tarsorrhaphy (to ophthalmology) unacceptable cosmetic result (to plastic surgery)
Ramsay Hunt syndrome
Ramsay Hunt syndrome, named after American neurologist James Ramsey Hunt (1872-1937) is also known as Herpes zoster oticus. Patients present with severe pain in one ear followed by facial palsy. Zoster vesicles appear around the ear, in the external ear canal, on the soft palate and in the tonsillar fossa. It is often accompanied by deafness and/or vertigo which are slow to resolve and may result in permanent deficit. Pain usually abates after 48 hours, but post-herpetic neuralgia can be a problem. If the patient presents within 24 hours of the rash appearing, treatment with antivirals (e.g. aciclovir 800 mg five times daily for a week) may be effective in reducing duration of symptoms. The effect of antivirals on the development of post-herpetic neuralgia is controversial with a recent Cochrane Review (Li et al., 2009) suggesting no benefit.
Trigeminal neuralgia
Patients with trigeminal neuralgia complain of paroxysms of intense stabbing, burning or ‘electric shock’ type pain lasting seconds to minutes in the trigeminal (V) nerve distribution (Fig. 4). In 96% of cases, the pain is unilateral and pain is more likely to be in the distribution of the mandibular and maxillary divisions of the trigeminal nerve rather than the ophthalmic division.
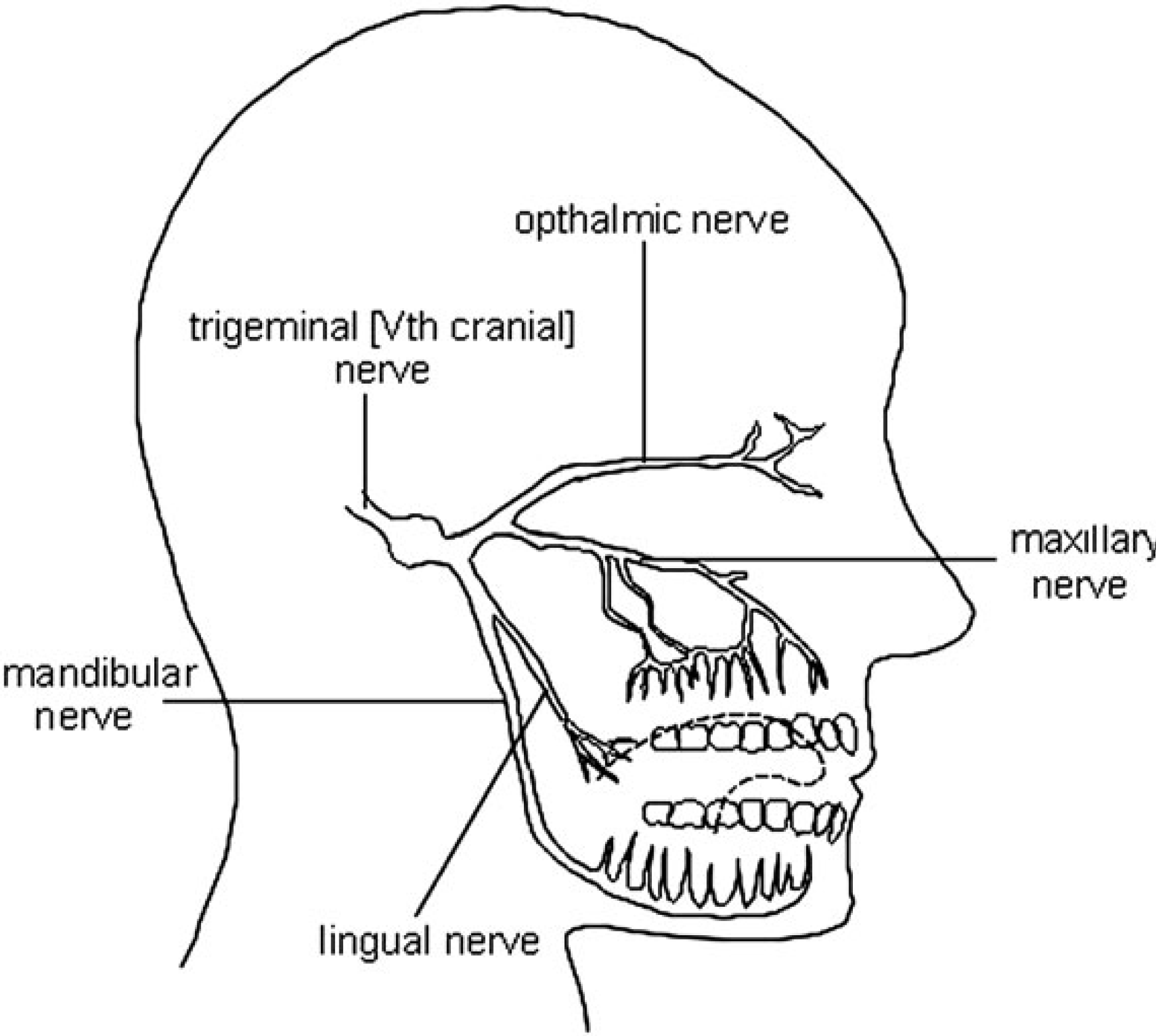
Distribution of the trigeminal nerve.
Frequency of attacks range from hundreds of attacks per day to remissions lasting years. Between attacks, there are no symptoms. Pain may be provoked by movement of the face (e.g. talking, eating or laughing) or touching the skin (such as when shaving or washing).
Trigeminal neuralgia can occur at any age but is more common in women and those over the age of 50. Its cause is unknown, but trigeminal neuralgia may be associated with multiple sclerosis, in women only it may be associated with hypertension.
If simple analgesia with paracetamol or a non-steroidal antiinflammatory drug (NSAID) is ineffective, try treatment with neuropathic painkillers. When pain is controlled, review regularly and on each occasion consider reducing the dose or stopping medication as spontaneous remission may occur. Refer for neurologist review if
the patient is under 50 years of age there is any neurological deficit between attacks or treatment with neuropathic painkillers in primary care fails—specialist options include drug treatment with lamotrigine, duloxetine, baclofen or phenytoin and/or surgical intervention
Morton's metatarsalgia
Morton's metatarsalgia is pain due to entrapment of the interdigital nerve between the third and fourth metatarsal heads in the foot and neuroma formation. Patients present with sudden attacks of pain or paraesthesia during walking. If suspected, refer to orthopaedics. Treatment is usually with steroid injection and modification of footwear. If this fails, some need surgical excision of the neuroma.
Autonomic neuropathy
Autonomic neuropathy is neuropathy affecting the autonomic nerves. Patients present with the symptoms summarized in Box 1.
Symptoms of autonomic neuropathy
Postural hypotension (dizziness or syncope on standing, after exercise or a large meal). Check blood pressure lying and standing—a postural drop of 30/15 mmHg or more is abnormal. Impotence Inability to sweat Vomiting and dysphagia Diarrhoea or constipation—exclude other causes for change in bowel habit Urinary retention or incontinence and/or Horner's syndrome: Sympathetic nerve disruption to the iris causes a small (meiotic) pupil with lack of pupil dilation in the dark, partial lid ptosis, anhydrosis of the forehead and enophthalmos (Fig. 5).

Horner's syndrome of the left eye. Science Photo Library.
Primary autonomic failure
Primary autonomic failure is autonomic neuropathy of unknown cause. It occurs alone or as part of multisystem atrophy and typically affects middle-aged or elderly men. Onset is insidious and diagnosis may be delayed. Despite a slow and often subtle onset, this is a serious condition and sufferers rarely survive more than 10 years after diagnosis. Treatment is supportive.
Ageing
A quarter of patients over the age of 74 have postural hypotension. This is often associated with disordered thermoregulation, making elderly people prone to hypothermia and also overheating in hot weather. Exclude other disorders such as diabetes and multisystem atrophy before putting symptoms of autonomic neuropathy down to ageing alone.
Other causes
Autonomic neuropathy may occur as part of more general polyneuropathy, such as diabetes mellitus, Guillain—Barré syndrome or alcoholic or nutritional neuropathy. Rarer causes include craniopharyngioma, vascular lesions, spinal cord lesions, tabes dorsalis, Chagas' disease, HIV and familial dysautonomia.
Management of autonomic neuropathy
Where possible treat any underlying cause identified. In all cases, discourage prolonged bed rest and review medication to exclude possible drug causes. Common culprits are antihypertensives, diuretics and drugs affecting the central nervous system (e.g. L-dopa, tricyclic antidepressants, phenothiazines and benzodiazepines).
Advise patients to stand slowly, raise the head of the bed at night, eat little and often and reduce carbohydrate and alcohol intake. Increasing dietary salt intake may help. Diabetic diarrhoea can be treated with two or three doses of 250 mg tetracycline (unlicensed). Otherwise treat with codeine phosphate 30 mg three or four times daily as needed. For gastric paresis, an antiemetic that promotes gastric transit, such as domperidone 30 mg three times daily, may be effective.
Refer for general medical or neurological review if diagnosis is unclear or simple measures are ineffective. Specialist treatments are usually unlicensed and include fludrocortisone 100–400 mcg daily for postural dropping of blood pressure and antimuscarinics such as propantheline bromide for gustatory sweating, but side effects (e.g. uncomfortable oedema with fludrocortisone) are common.
Polyneuropathy
Polyneuropathy is a generalized disorder of peripheral nerves, including cranial and autonomic nerves. The distribution of polyneuropathy is bilateral, symmetrical and widespread in contrast to mononeuritis multiplex which typically affects only a few nerves, often in different areas of the body. There are two main types of polyneuropathy:
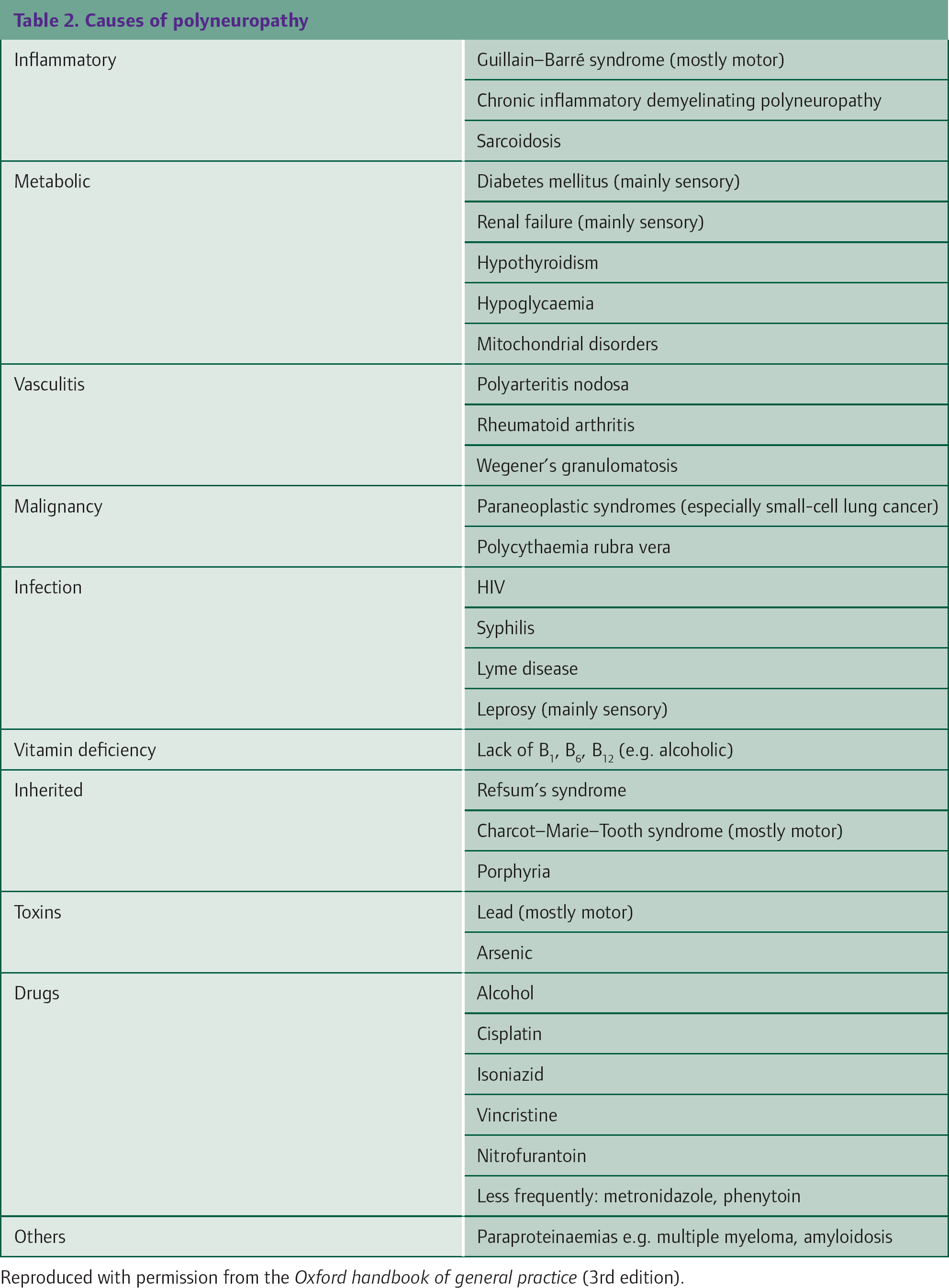
The common causes of polyneuropathy are listed in Table 2; however, in about 30% of cases, no cause can be isolated. Initial investigations in the surgery should be directed at excluding common causes. A reasonable initial screen, with appropriate counselling, might include
Full blood count Erythrocyte sedimentation rate and/or C-reactive protein Fasting blood glucose Renal function tests Liver function tests Thyroid function tests Plasma B12 level Autoimmune profile and Syphilis serology
Causes of polyneuropathy
In all cases, treat the cause if possible. Recovery time is highly variable if the cause can be resolved and can take months or even years. Involve physiotherapists and occupational therapy as needed. If there is sensory neuropathy, care of the feet is important to minimize trauma and consequent disability. Specialist podiatry may be required.
Refer for neurological review if a cause is not found. If there is rapid deterioration, admit as an acute medical emergency as ventilation may be needed.
Diabetic polyneuropathy
Symmetrical sensory progressive polyneuropathy affects 40–50% of patients with diabetes. It starts distally in a glove-and-stocking distribution and affects the feet more than the hands. It may be asymptomatic or cause numbness, tingling or neuropathic pain. Pain can be depressing and disabling, so it is important to be supportive. If simple analgesia with a paracetamol or an NSAID is ineffective, try neuropathic painkillers. When pain is controlled, review regularly and consider reducing dose or stopping medication.
Guillain—Barré polyneuritis
Although relatively rare, Guillain—Barré polyneuritis is important as its onset is often rapid and the consequences of missing the diagnosis can be severe. It is named after two French neurologists, Georges Guillain and Jean-Alexandre Barré and is thought to have an autoimmune basis. It tends to affect young, fit people and often develops within a few weeks of surgery, influenza vaccination or infection (upper respiratory tract, influenza, varicellazoster, herpes simplex, cytomegalovirus, glandular fever, campylobacter or mycoplasma infection). However, in 40% of cases, no precipitating event is identified.
Guillain—Barré polyneuritis presents with ascending motor neuropathy which may advance fast. The proximal muscles are more affected than distal muscles, and the trunk, respiratory muscles and muscles supplied by the cranial nerves are commonly affected.
If suspected, admit immediately to hospital as an acute medical emergency. Ventilation is frequently required. Although Guillain—Barré polyneuritis carries a 10% mortality, 85% of patients make a complete or near complete recovery with supportive care. However, 10% are still unable to walk alone a year after onset of symptoms.
Charcot—Marie—Tooth syndrome
Charcot—Marie—Tooth syndrome (named after two French neurologists, Jean-Martin Charcot and Pierre Marie, and English neurologist, Henry Tooth) is also known as peroneal muscular atrophy and is the most common hereditary motor and sensory neuropathy. Its inheritance is variable and may be autosomal dominant, autosomal recessive or X linked.
Charcot—Marie—Tooth syndrome presents at puberty or in early adult life and begins with foot drop and weak legs. The peroneal muscles are the first to atrophy. The disease spreads to the hands and then to the arms. Sensation and reflexes are also reduced. Intelligence is not affected and most individuals have a normal lifespan. Once diagnosis is confirmed, treatment is supportive.
Charcot osteoarthropathy
A Charcot's joint occurs in a neuropathic foot. The joint is damaged as a result of trauma secondary to loss of pain sensation. If suspected refer immediately to the multidisciplinary foot care team for immobilization and long-term management.
Neuropathic pain
Neuropathic pain occurs as a result of damage to neural tissue, for example as a result of diabetic neuropathy. Pain typically occurs in association with altered sensation, for example burning, stabbing or numbness. Pain may also be provoked by non-noxious stimuli (allodynia) such as gentle heat or cold.
Non-drug treatments
Patients with chronic neuropathic pain often require a multidisciplinary approach including physiotherapy and psychological support. Transcutaneous electrical nerve stimulation and/or acupuncture may help in some cases. If the patient has severe intractable pain, nerve blocks may help—refer for specialist advice.
Analgesics
NSAIDs are sometimes effective for neuropathic pain—either because there is mixed nociceptive pain or because they reduce inflammatory sensitization of nerves. There is considerable variation in individual patient tolerance and response.
Neuropathic pain often responds only partially to opioid analgesics. Of the opioids, oxycodone, tramadol and methadone are probably the most effective—consider when other measures fail.
Tricyclic antidepressants
Amitriptyline is the most commonly prescribed drug for neuropathic pain. Start at a dose of 25 mg at night (nocte)—10 mg nocte if elderly. Increase the dose by 10–25 mg nocte every 5–7 days to a maximum of 75 mg nocte as needed (higher doses under specialist supervision). Some patients do not derive benefit for 4–6 weeks. Alternatives include nortriptyline, dosulepin and lofepramine.
Although there is a strong evidence base for the use of amitriptyline for neuropathic pain, it is not a licensed indication. It is important to inform patients and carers of what you are doing and why. Explain that the patient information leaflet will not have information about the use of the drug in these circumstances and record in the patient's notes your reasons for prescribing outside the licensed indications for the drug.
Anticonvulsants
Gabapentin and pregabalin (Box 2) are both licensed for treatment of neuropathic pain and are now used in preference to other anticonvulsant medications for this purpose and as second-line medication when amitriptyline is ineffective.
Carbamazepine was traditionally the drug of choice for neuropathic pain but it is unlicensed and often poorly tolerated. Oxcarbazine is an alternative. Sodium valproate, lamotrigine and phenytoin are also occasionally used for neuropathic pain but are reserved for use under specialist supervision.
Dose regimes for gabapentin and pregabalin
Gabapentin
300 mg on day 1 300 mg twice daily on day 2 300 mg three times daily on day 3 then increase dose according to response in steps of 300 mg daily—in three divided doses—to a maximum of 1.8 g/day.
Pregabalin
initially 150 mg daily in two to three divided doses increased if necessary after 3–7 days to 300 mg daily in two to three divided doses increased further if necessary after 7 days to a maximum of 600 mg daily in two to three divided doses
Other drug treatments
Corticosteroids may help relieve pressure in compression neuropathy and, indirectly, pain. They are most commonly used in palliative care situations. Start with a high initial dose to achieve rapid results (dexamethasone 8 mg/day works in 1–3 days), then rapidly reduce the dose to the minimum that maintains benefit.
Capsaicin is a topical treatment licensed for neuropathic pain. Apply a small amount three to four times daily. It acts by counter-irritation but intense burning during initial treatment limits use. Advise patients to wash their hands after application and avoid application after a hot shower or bath as this causes an increase in the burning sensation.
Plasters impregnated with lidocaine 5% (Versatis™) are licensed for post-herpetic neuralgia. Apply daily for up to 12 hours, followed by a 12-hour plaster-free period. Up to three plasters may be used to cover large areas; plasters may be cut. Discontinue if there is no response after 4 weeks.
Referral
If you are unable to achieve adequate pain relief for a patient with neuropathic pain, consider referral to a specialist pain control clinic (or palliative care team if more appropriate).
Support for patients with peripheral neuropathy
Peripheral neuropathy is a blanket term and patients with the condition often find it difficult to find information and support of relevance to their particular problem. In some ways, it is easier if an underlying cause has been found, but in many cases, no underlying cause is identified resulting in uncertainty about prognosis and course of symptoms.
Often there may be no outward signs that the patient has a problem. This can lead to difficulties with peers and employers. Furthermore, peripheral neuropathy is often painful and neuropathic pain is particularly unpleasant and difficult for others to understand. That in itself is wearing and depressing.
In all cases, talk through these issues and provide support Use screening questions (Box 3) to identify possible depression. Consider liaising with the patient's employe (with patient permission) to explore whether adaptations to the working environment may help the patient to cope at work, and employ the whole multidisciplinary team as needed, for example physiotherapy to aid mobility and occupational therapy to arrange home adaptations. Explore whether the patient and any informal carers might be eligible for any benefits to provide additional financial support.
NICE screening questions for depression
During the last month, have you often been bothered by feeling down, depressed or hopeless? During the last month, have you often been bothered by having little interest or pleasure in doing things?
A positive response to either of these questions should prompt further assessment, for example with the Patient Health Questionnaire depression-screening tool.
Where the neuropathy results from a specific underlying cause, such as diabetes, support and useful information sheets may be available from the disease-specific support charities. For example, the Trigeminal Neuralgia Association (website: www.tna.org.uk) provides information and support for sufferers from that condition and Diabetes UK (website www.diabetes.org.uk) produces an excellent leaflet entitled ‘Diabetic neuropathy’. The Neuropathy Trust (website www.neurocentre.com) provides information, support and an interactive forum for those with rarer conditions or where a cause has not been identified.
Key points
Although many individual causes of peripheral neuropathy are rare, there are about 4.7 million people affected by peripheral neuropathy of some sort in the UK The most common cause is diabetes, but in many cases, no underlying cause for the patient's neuropathy is found Peripheral neuropathy may take the form of mononeuritis, mononeuritis multiplex, autonomic neuropathy or polyneuropathy Management involves identification and treatment of the underlying cause, where possible, and supportive care Neuropathic pain is a particularly unpleasant symptom which may be treated with neuropathic painkillers such as amitriptyline or anticonvulsants