
Abstract
The pancreas is a retroperitoneal organ with both endocrine and exocrine functions. It was first described by a Greek physician Herophilus between 335 and 280 BC and was given its name by Ruphos only a few hundred years later. In 1642, Wirsung discovered the pancreatic duct and within three decades Graff investigated its secretory properties. Paul Langerhans described ‘islets of Langerhans’ in 1869 and the first description of pancreatitis as a disease was by Fitz in 1889. Halstead performed the first operation on the pancreas in 1898.
The GP curriculum and pancreatic disease
There are several sections of the GP curriculum of relevance to pancreatic disease.
GPs have a crucial role to play in promoting health and preventing disease. To put patients at the centre of their care, GPs need to possess appropriate skills to support people to self-care, taking them through a range of approaches in partnership, recognizing that the individual should make the choices, decisions and take the actions themselves.
It has relevance to the presentation of acute pancreatic disease. It specifically states that the effective management of an acutely ill person will include recognition and immediate management.
It has relevance to those patients with possible pancreatic malignancy. It emphasizes the importance of the role of the GP, which extends from primary prevention through early diagnosis of cancer to terminal care.
It emphasizes the GP's central role in the diagnosis and management of digestive problems in primary care. The knowledge base relevant to this subset of illnesses should include an awareness of symptoms of digestive disease including abdominal pain and jaundice. Common and important diseases include gallstone-related disease and gastrointestinal (GI) cancers (including pancreatic).
Both drug and alcohol problems are relevant to the primary and secondary prevention of both acute and chronic pancreatic disease as alcohol is one of the main aetiological factors. Statement 15.3 specifically states that the knowledge base of GPs should include the symptoms and signs of manifestation of alcohol problems including physical, psychological and social.
Pancreatic structure and function
A basic appreciation of pancreatic structure and function allows understanding of pancreatic disease processes, their presentation, associated complications, the rationale for logical investigation and subsequent management and common pitfalls. The pancreas lies retroperitoneally in the trans-pyloric plane. Anatomically, it is divided into a head and uncinate process, neck, body and tail. It has important relations (Fig. 1) to the coeliac plexus, confluence of the superior mesenteric and portal veins and common bile duct (CBD). Thus, a pancreatic neoplasm may cause intractable pain, portal vein obstruction or obstructive jaundice from CBD obstruction.

Anatomical relations of the pancreas gland.
Functionally, the pancreas gland has two divisions — endocrine and exocrine. The pancreas is lobulated and encapsulated with the lobules being made of secretory cells draining via their ductules into the CBD via the pancreatic duct, which forms the exocrine portion. Between the alveoli are islets of Langerhans, which have endocrine functions secreting directly into the portal circulation.
Exocrine pancreas
The exocrine pancreas secretes pancreatic juice in response to stimulation by the vagus nerve. Pancreatic juice has an acinar and ductal component.
The acinar cells secrete enzymes that digest duodenal content, and the alkaline composition of the ductal secretions increases the pH of duodenal contents. This loss of exocrine function and subsequent malabsorption is part of the explanation for weight loss and malnutrition (together with pain on eating and gastric outlet obstruction) in patients with chronic pancreatitis.
Endocrine pancreas
The endocrine portion of the gland secretes a range of hormones including insulin, glucagon, somatostatin and pancreatic polypeptide from the islets of Langerhans. These pass directly into the blood stream and loss of endocrine function leads to the inability to regulate glucose levels and thus diabetes mellitus.
Acute pancreatitis
Pancreatitis is an inflammatory condition of the pancreas, which may be acute or chronic and range from simple oedema to haemorrhage and necrosis. Acute pancreatitis is an acute inflammatory process affecting the pancreas with variable involvement of other regional or remote organ systems. The majority of first attacks in the UK are secondary to gallstones and approximately 85% of cases run a self-limiting course and rapidly resolve with a short period of analgesia and intravenous fluid resuscitation. The remaining 15% of cases have a severe systemic illness with high morbidity and mortality.
Epidemiology
The annual incidence of acute pancreatitis in the UK is reported as 318 cases per million with a male to female ratio of approximately 1.5: 1. Over recent years, there has been a suggestion of an increasing incidence of pancreatitis in the UK, the cause of which is not fully known, but in Finland a similar increase is correlated to increasing alcohol consumption. The first presentation is commonly in the fourth and fifth decades of life but younger patients are frequently seen. Mortality is classically quoted as 10% of cases but recent data suggest that this figure is lower and the 85% of cases who have mild disease contribute only 5% of this mortality rate, as opposed to a reported mortality rate of 30% associated with acute severe pancreatitis.
Aetiology
Acute pancreatitis is caused by many different aetiological factors (Box 1). It is estimated that in the UK 50–70% of cases are directly related to gallstones and alcohol accounts for 25% of cases. Recent studies have suggested that cases of alcohol-induced pancreatitis are increasing. Aetiology is an important factor as removal of the causative agent is likely to avoid further episodes of pancreatitis.
Causes of acute pancreatitis
Gallstones Alcohol
Trauma — endoscopic retrograde cholangiopancreaticogram (ERCP), biliary monometry Tumour — pancreatic duct obstruction, ampulla of Vater neoplasia Drugs — Azathioprine, diuretics, oestrogens, thiazides, steroids Metabolic — hypercalcaemia, hyperlipidaemia Infection — mumps, Coxsackie B, human immunodeficiency virus Vascular — vasculitis, cardiopulmonary bypass Hereditary — abnormal trypsinogen stability
Clinical presentation
There are no pathognomonic symptoms or signs of acute pancreatitis and presentation may range from mild discomfort in the epigastrium to continuous overwhelming abdominal pain. Thus, acute pancreatitis may be one of a number of differential diagnoses (Box 2). Pain is often acute with a maximum intensity within minutes. It is often poorly localized, worse lying down and radiates to the back in approximately 50% of patients. Pancreatitis is almost always associated with nausea, vomiting or wretching. Occasionally, patients may appear confused from metabolic disturbance or hypoxaemia. Patients may have a prior history of symptoms consistent with gallstone disease or be known to have gallstones. In alcohol-induced pancreatitis, patients may declare recent excessive alcohol intake or give a long history of high alcohol use.
Differential diagnosis of acute pancreatitis
Acute cholecystitis/cholangitis Perforated viscus Peptic ulcer disease Abdominal aortic aneurysm High intestinal obstruction Mesenteric infarction Myocardial infarction
Clinically, the patient may appear well but is likely to exhibit signs of respiratory and cardiovascular dysfunction, being systemic inflammatory response syndrome positive with tachycardia, tachypnoea and fever. Patients with marked or swinging pyrexia are more likely to have cholangitis. They may be hypotensive indicating profound shock.
Examination of the abdomen is likely to reveal abdominal pain, which can range from mild discomfort in the epigastrium to peritonitis. Most commonly, there is guarding in the upper abdomen and marked tenderness. The abdomen may be distended with decreased or silent bowel sounds.
Patients occasionally appear icteric with obstructive jaundice caused by gallstones or more commonly pancreatic head oedema leading to obstruction of the CBD. Rarely, there may be evidence of retroperitoneal haemorrhage into the fascial planes presenting as flank (Grey Turner's sign) or peri-umbilical echymoses (Cullen's sign).
Initial primary care management strategy
Patients encountered in the primary care setting by the GP who have acute epigastric pain and who are clinically unwell should be assessed and referred as a surgical emergency. Appropriate care of acute pancreatitis requires timely diagnosis and supportive management to reduce the risk of complications and associated morbidity and mortality.
Patients should be made nil by mouth, and intravenous fluids commenced if available and signs of circulatory dysfunction are present. Analgesia is appropriate and is unlikely to mask vital diagnostic signs in the acute abdomen. Anti-emetic medication may help relieve nausea and make the patient feel more comfortable.
Confirmation of diagnosis in secondary care
Diagnosis traditionally depends on the detection of a serum amylase concentration three times the upper limit of normal. Hyperamylasaemia occurs in other conditions (Box 3) and these must be remembered when faced with a patient who has suspected pancreatitis. Conversely, a normal amylase does not rule out the diagnosis as concentrations may have normalized in patients with a prolonged history.
Causes of hyperamylasaemia
Acute pancreatitis Pancreatic pseudocyst Mesenteric infarction Abdominal aortic aneurysm Perforated viscus (gall bladder) Acute cholecystitis Diabetic ketoacidosis Mumps
Secondary care management
Many management guidelines for acute pancreatitis have been published. These generally include initial resuscitation with a low threshold for intensive care input, severity stratification, establishing aetiology and subsequent pancreatic imaging.
Patients require aggressive supportive therapy. Early warning score (EWS) monitoring, intravenous fluids, analgesia and oxygen are the mainstay of treatment instigated on admission to the acute surgical unit.
Patients are often catheterized for careful observation of urine output. Blood glucose levels are closely monitored and insulin therapy may be required for tight glycaemic control. Patients are often fed early and if oral intake is not tolerated a nasogastric or nasojejunal feed can be started. Antibiotics are not routinely employed as the evidence for their use is equivocal. Antibiotics are generally restricted to patients with proven necrosis or a secondary infective source.
Acute pancreatitis can be classified as mild or severe. This has an important bearing on how to expectantly manage the patient due to the dramatic differences in outcome. In general, disease in patients with mild pancreatitis runs a self-limiting course and resolves rapidly, whereas patients with severe pancreatitis often develop multiorgan failure and require a period of management on the intensive care unit.
Numerous simple scoring systems exist, which allow easy risk stratification (Box 4). These systems are multifactorial and require collection of numerous variables to predict severity. It is recognized that they achieve approximately 80% accuracy in predicting prognosis. Recently, a biochemical scoring system based upon C-reactive protein has been shown to have a similar predictive performance but is limited by the lag to reach peak plasma concentration from the onset of disease.
Scoring systems for acute pancreatitis

All patients diagnosed with acute pancreatitis undergo an abdominal ultrasound scan (USS) to detect the presence of gallstones or CBD dilatation. Patients with prognostically severe pancreatitis also undergo a contrast enhanced computed tomography (CT) scan looking for pancreatic necrosis.
Interval cholecystectomy should then be scheduled within 6 weeks of discharge if the patient is fit enough for surgery. Patients unfit for surgery may be managed expectantly with an elective ERCP and sphincterotomy with biliary stent insertion if necessary. If there is evidence of CBD obstruction and cholangitis associated with severe disease, then an urgent ERCP should be considered in a specialist centre. If the attack is thought to be secondary to alcohol, a thorough history should be taken to illicit this and appropriate counseling offered to aid abstinence.
Complications
Delayed complications (Box 5) may present to the GP and should be considered in patients recently discharged from hospital after an attack of pancreatitis. Cardinal symptoms include persistent pain, failure to gain weight, reduced appetite and vomiting. Haemorrhagic complications will present with the above plus varying degrees of shock. Patients with recurrent attacks may have a pancreatic duct stricture.
Complications of acute pancreatitis
Pancreatic necrosis Pancreatic pseudocyst Pancreatic duct fistula Gastric outlet obstruction Abscess formation Haemorrhage Thrombosis Gastrointestinal haemorrhage
Primary care management post-hospital discharge
The role of the GP after hospital discharge is vital. The stimulus deemed responsible for causing the attack of acute pancreatitis needs to be removed to prevent further attacks. For example, GPs should be aware that patients with gallstone-induced pancreatitis need to be scheduled for a subsequent cholecystectomy. If a patient is lost to follow-up, GPs are advised to re-refer patients urgently unless an alternative management plan has been put in place. Another example is patients with pancreatitis as a result of alcohol overuse. These patients need significant primary care advice and support with alcohol abstinence. Summary of acute pancreatitis.
Gallstones (50–75%) and alcohol (25%) are the most common causes of acute pancreatitis in the UK population If acute pancreatitis is suspected, urgent admission is warranted to an acute surgical unit The mortality rate of acute pancreatitis is approximately 10% Ongoing management in primary care after hospital discharge includes making sure the causative agent is removed/avoided
Chronic pancreatitis
Chronic pancreatitis is a chronic inflammatory process affecting the pancreas with irreversible progressive destruction of pancreatic tissue and subsequently irreversible fibrosis.
Epidemiology
Alcohol is the prime aetiological factor and the incidence of chronic pancreatitis in industrialized countries is rising secondary to an increase in alcohol consumption. The incidence of chronic pancreatitis is thought to be in the region of 13 per 100 000 in the Western world and there was a 4-fold increase in chronic pancreatitis from the 1960s to the 1980s. Owing to a greater alcohol consumption in men, the male to female ratio is 4 : 1 but we are seeing a disproportionate increase in the number of cases in the female population. Mean age of onset is 40 years.
Aetiology
Alcohol is thought to play a role in the development of 60–70% of new cases of chronic pancreatitis. There are numerous other causes (Box 6) including tobacco, but it is difficult to be dogmatic about the exact contribution due to smoking's association with alcohol use.
Causes of chronic pancreatitis
Alcohol —most frequent cause Tropical pancreatitis Obstructive pancreatitis Hereditary chronic pancreatitis Biliary tract disease Idiopathic chronic pancreatitis
Hereditary chronic pancreatitis is important as avoidance of other factors such as tobacco and alcohol must be taken to reduce the risk of developing chronic pancreatitis. There is also an association with pancreatic cancer and patients should be considered for pancreatic cancer surveillance. This is not a clear-cut decision as patients undergoing surveillance are likely to find it difficult to attain life insurance or a mortgage, the association is relatively weak and investigations will not reliably detect the early development of malignancies. Thus, a patient must be counselled as to the implications, risks and benefits.
Pathophysiology
The mechanisms for development of chronic pancreatitis are not fully understood. Chronic pancreatitis is characterized by sclerosis and destruction of the exocrine parenchyma and associated ductal dilatation secondary to protein plugs and calcification.
Clinical presentation
Patients generally complain of poor health with a primary symptom of pain. Pain is of varying intensity and ranges from episodic occurrence to constant severe pain. Most patients describe a constant dull gnawing background pain with severe episodic attacks. The pain is often felt in the epigastrium radiating to the back or shoulder tip and may be alleviated by leaning forward or adopting the ‘jackknife position’. Patients may use a hot water bottle to aid pain relief that in turn may lead to the development of erythema ab igne. The pain often leads to a decrease in the patient's quality of life, loss of sleep, time off work and an eventual dependency on high-dose opioids. Severity appears to correlate with quality of life and hospital admissions.
Nausea and vomiting is common and may be a factor in weight loss and malnutrition, which is caused by gradual loss of pancreatic exocrine and endocrine function. Pancreatic insufficiency presents with diabetes (endocrine) and steatorrhoea (exocrine) often years after the initial diagnosis.
Investigations and diagnosis
In primary care, if chronic pancreatitis is suspected, refer for a specialist opinion to confirm diagnosis. Diagnosis of chronic pancreatitis is generally based on history and imaging of the pancreas.
Plain abdominal radiography may give the appearance of opacities related to the pancreas suggesting calcification. Ultrasound is used to assess local complications including bile or pancreatic duct dilatation and the presence of a pseudocyst but does not produce adequate images of the pancreas to aid diagnosis. Contrast enhanced CT (Fig. 2) is the prime investigation of choice and demonstrates the gland revealing the morphological appearance and any areas of damage. CT may also demonstrate an enlarged pancreatic duct and associated cysts.

CT showing pancreatic calcification representing chronic pancreatitis.
ERCP has been shown to be the most effective method of diagnosing early chronic pancreatitis when combined with CT, but it is not routinely used due to the risk of acute pancreatitis, cholangitis and visceral perforation. Magnetic resonance cholangiopancreatography (MRCP) has largely replaced ERCP due to the reduced risks and excellent quality of the images with recent equipment.
Other investigations that may be carried out include
Biochemistry — amylase levels are usually within normal limits or very slightly raised. Liver function tests are routinely normal but may demonstrate obstructive jaundice if there is associated biliary obstruction. A fasting blood glucose level should be performed if chronic pancreatitis is expected. Tests of pancreatic function — pancreatic function tests such as faecal elastase are not used in all centres, as there is an argument that they merely confirm the presence of pancreatic exocrine insufficiency. They do not differentiate between chronic pancreatitis and pancreatic cancer.
Management strategy
Chronic pancreatitis is a difficult condition to manage in primary and secondary care. Many patients are successfully treated conservatively without difficulty for long periods of time but management is often complicated by pain that may be severe, unrelenting and unresponsive to treatment. Alcohol use/withdrawal, smoking cessation and malnutrition secondary to anorexia and pancreatic insufficiency also hinder management.
Treatment of pain
The treatment of pain should utilize the analgesic ladder. Pain control may initially be achieved by simple analgesics such as paracetamol but these are often poor at controlling pain from a visceral source. Many patients require opioid analgesia commencing with codeine and/or tramadol and progressing to slow-release morphine preparations as pain increases or is less well controlled. Pethidine should be avoided due to the potential for dependency and addiction. Non-traditional analgesics such as amitriptyline and selective serotonin uptake inhibitors are used in conjunction with non-opioid and opioid analgesics to good effect.
In patients who have intractable pain despite appropriate and maximal oral analgesic therapy, approaches such as coeliac plexus blockade and splanchnicectomy have been used but have yet to show effective long-term control of pain. Surgery may also be utilized in the management of pain.
Alcohol avoidance and smoking cessation
The role of the GP is crucial in helping the patient avoid alcohol and stop smoking. Patients require considerable support from their GP and the rapport between doctor and patient is pivotal to abstinence.
Nutrition
Patients with chronic pancreatitis are often malnourished secondary to a combination of anorexia, nausea and pancreatic insufficiency. Adequate analgesia and antiemetics may reduce anorexia and nausea.
Pancreatic replacement therapy is often required to treat steatorrhoea and the associated malabsorption secondary to pancreatic insufficiency. Treatment is generally commenced when the patient is losing weight and/or has diarrhoea with a faecal fat excretion in excess of 15 g/day or abnormally low faecal elastase. Along with this, a fat reducing diet may be appropriate to help pain relief but must be part of a well-balanced diet with sufficient calorie intake.
Glycaemic control
Patients who lose pancreatic endocrine function subsequently develop diabetes mellitus. Glycaemic control may be difficult due to variable food intake and lack of endogenous glucagon. Patients have an increased susceptibility to insulin and have an increased risk of hypoglycaemia.
Surgical options
Surgical treatment in chronic pancreatitis is reserved for pain, gastric outlet obstruction with intractable vomiting or obstruction of the CBD that cannot be managed endoscopically. Surgical procedures are also performed to treat secondary complications (Table 1) such as pancreatic pseudocysts, upper gastrointestinal (GI) bleeding due to the involvement of the duodenum or upper abdominal vessels.
Complications of chronic pancreatitis

Procedures for pain include pancreatic duct drainage or formal pancreatic resection. Drainage procedures such as a lateral pancreaticojejenostomy are thought to allow drainage of a blocked pancreatic duct thus reducing pressure and subsequently reducing pain. In practice, surgical drainage procedures are ineffective as duct dilatation is often secondary to fibrosis pulling the duct open and not due to pressure subsequent to obstruction that would be relieved by drainage.
Pancreatic resections may be local or extensive. Due to chronic pancreatitis affecting the whole gland, an extensive procedure is often necessary. Total pancreatectomy is associated with significant morbidity but recent results with associated islet cell autotransplantation are promising and reduce or can even abolish insulin requirements. Summary of chronic pancreatitis
The incidence of chronic pancreatitis is increasing The number one causative agent is alcohol Patients are often initially managed with simple analgesics and abstinence A significant proportion of patients progress to severe pain and pancreatic insufficiency Analgesic requirements may be high and opioid dependency is common, especially with pethidine Nutrition is problematic. Patients inevitably require replacement of pancreatic enzymes and may need insulin. Patients are often extremely sensitive to insulin and are at risk of hypoglycaemia Surgery is reserved for advanced cases after adequate counselling in specialist centres.
Pancreatic carcinoma
In the UK, 7600 patients are diagnosed with pancreatic cancer per year and pancreatic cancer is the fifth most common cause of cancer-related deaths. Ductal adenocarcinoma is by far the most common pancreatic neoplasia accounting for 95% of malignant pancreatic lesions and 85% of all pancreatic lesions. In patients with small (less than 2-cm diameter), localized tumours and no lymph node metastases, surgical resection can yield survival rates of 18–24%; however, less than 10% of tumours are amenable to surgical resection at presentation. Survival rates without operative resection are dismal and compounded by a poor response to chemotherapy. Five-year survival rates are in the region of 2–3% but less than 1% at 5 years in patients with advanced disease, with most patients dying within a year.
Epidemiology
Pancreatic cancers are a significant cause of mortality, being responsible for approximately 200 000 deaths per year worldwide. The incidence is particularly high in the Western world with 40 000 deaths in Europe and 30 000 in the USA per year. It is estimated that the incidence in the UK is 12 per 100 000 population per year. It affects men and women equally and peak incidence is in the seventh decade of life. Pancreatic cancer is extremely rare under the age of 30 years.
Aetiology and risk factors
There are several documented risk factors associated with pancreatic cancer (Box 7). Smoking is classified as a proven carcinogen with respect to carcinoma of the pancreas. It is thought to relate to the steady rise in the incidence of pancreatic cancer over recent decades. Alcohol alone does not increase the risk of pancreatic carcinoma unless it leads to chronic pancreatitis.
Risk factors associated with development of pancreatic carcinoma
Smoking Diabetes Chronic pancreatitis Diet Adenoma of the ampulla Familial adenomatous polyposis Gardner's syndrome
Clinical presentation
Presentation of pancreatic carcinoma is often vague in the early stages of the disease and as such many patients often present with advanced disease (Box 8). Early in the disease, patients often report non-specific symptoms including anorexia, malaise, nausea and fatigue. Common later presentations include epigastric pain often radiating to the back, painless obstructive jaundice and significant weight loss due to cancer-related anorexia, subclinical malabsorption and gastric outlet obstruction. Rarer clinical presentations include diabetes mellitus, Trousseau's sign (migratory superficial thrombophlebitis), steatorrhoea and alterations in endocrine function associated with neuroendocrine tumours (NETs).
Presenting symptoms and signs of pancreatic carcinoma
Weight loss (91% of cases) Jaundice (71%) Pain (83%) Malaise (34%) Ascites (30%) Pancreatitis (5%) Anorexia Fatigue Nausea and vomiting
Referral to secondary care
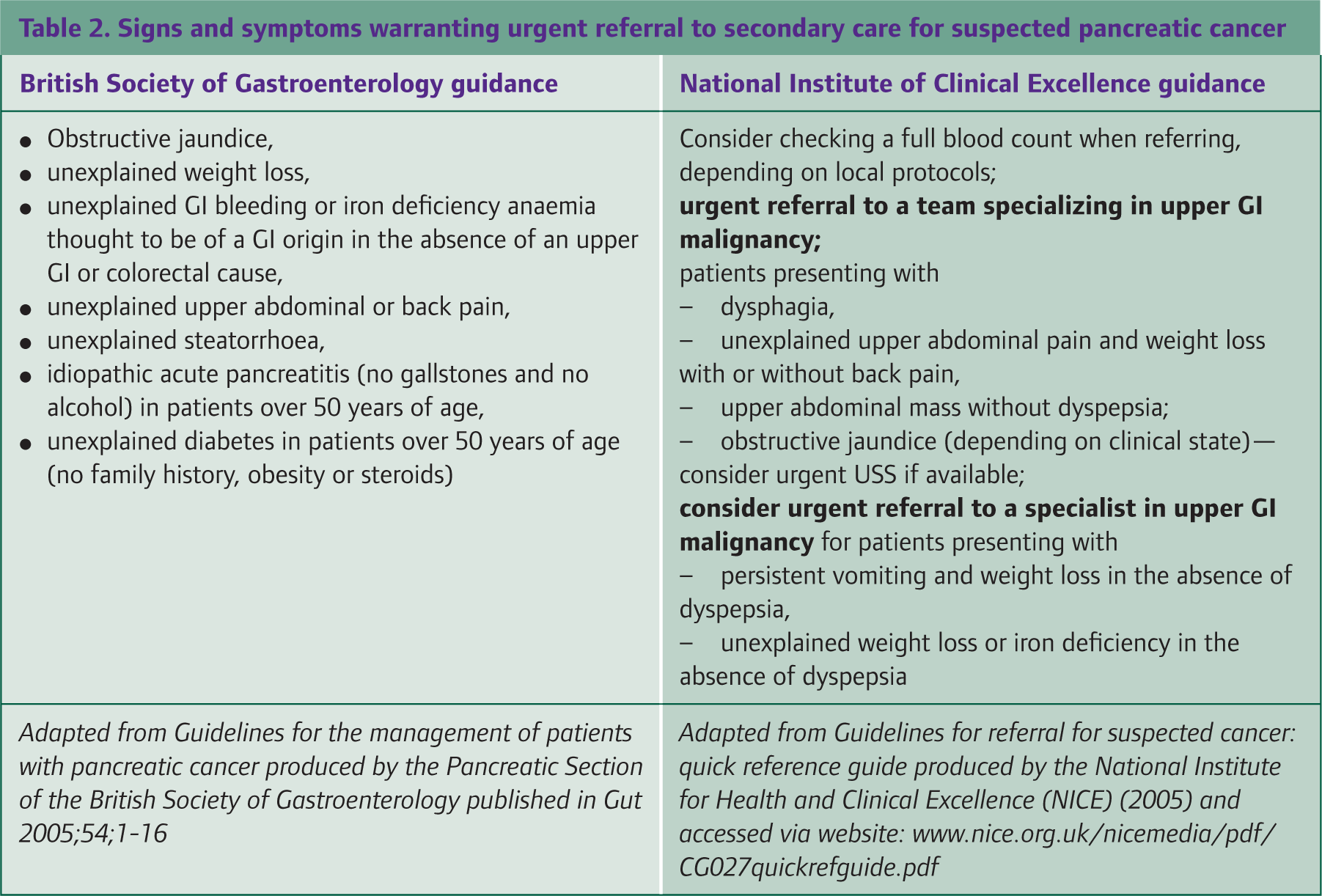
Both the British Society of Gastroenterology and National Institute of Clinical Excellence have published documents with guidelines stating which patient groups merit GP referral to a local cancer unit (Table 2).
Signs and symptoms warranting urgent referral to secondary care for suspected pancreatic cancer
Diagnosis and staging in secondary care
Due to the initial vague presentation, a high index of suspicion is required. Commonly biochemical tests lie within normal ranges. Blood tests including liver function tests may be deranged (with a raised bilirubin and alkaline phosphatase) indicating an extrahepatic obstructive cause for jaundice.
A raised carbohydrate antigen 19-9 (CA 19-9) is highly specific for pancreatic cancer in the absence of biliary tract disease, intrinsic liver disease or benign pancreatic disease. About 75–85% of patients with pancreatic cancer have elevated CA 19-9 levels.
Patients often have an upper abdominal USS, which may be normal as overlying bowel gas often largely obscures the pancreas. USS may, however, show dilation of the bile ducts and exclude gallstones in obstructive jaundice.
A contrast enhanced CT is the gold standard investigation and allows visualization and characterization of the tumour (Fig. 3). It also gives valuable information on spread and resectability of the disease. MRCP may be utilized if the diagnosis of obstructive jaundice is in doubt as this allows visualization of the bile duct and related structures.

CT showing a malignant mass in the head of the pancreas.
The majority of patients with peri-ampullary tumours will undergo an ERCP. About 90–95% of patients with pancreatic tumours have abnormalities visible at ERCP but these are not specific for pancreatic adenocarcinoma. ERCP does not allow direct biopsy of the lesion but brushings from the bile duct may be taken for cytology. The placement of a stent for therapeutic biliary drainage can be performed but does carry a significant risk of complications (5–10%).
Pre-operative staging laparoscopy is advocated in the vast majority of centres. This allows direct or ultrasound visualization of the spread of the primary tumour, direct biopsy of the primary lesion and visualization of liver or peritoneal metastases that may preclude curative resection.
Histology
There are many subtypes of pancreatic tumour with varying histological appearances (Table 3). They may be exocrine (epithelial) or endocrine in origin. Exocrine tumours are further categorized as solid or cystic. Eighty-five percent of all pancreatic lesions are ductal adenocarcinomas of the exocrine pancreas. Of the remaining tumours of the exocrine pancreas, 2% are benign and less than 5% (which may be benign or malignant) are cystic in nature.
Classification of pancreatic neoplasms

Rarely, patients may develop endocrine tumours of the pancreas derived from the islet cells that may be functional or non-functional. These include insulinomas and gastrinomas, which are part of the gastrointestinal neuroendocrine tumour (GP-NET) group and may occur anywhere within the GI tract but most commonly in the pancreas (Table 4).
Classification, location, malignant potential and clinical features of GI NETs

Treatment
The treatment of pancreatic cancer is coordinated by regional hepato—pancreato—biliary (HPB) specialist multidisciplinary teams. Therapy in pancreatic cancers can be divided into curative or palliative treatments depending upon the stage of the disease. As with all tumours, a multidisciplinary approach to treatment of pancreatic cancer is essential.
Surgical resection offers the only possibility of cure. Unfortunately, only 10% of cases are suitable for resection at the time of presentation. Resection depends upon tumour location, with peri-ampullary tumours being most amenable to resection (resection rate is approximately 10–15%). Resection requires a pancreaticoduodenectomy (Whipples procedure) (Figs. 4 and 5).

Diagram showing resected area (grey shaded area) in a pancreaticoduodenectomy from Mayo clinic.
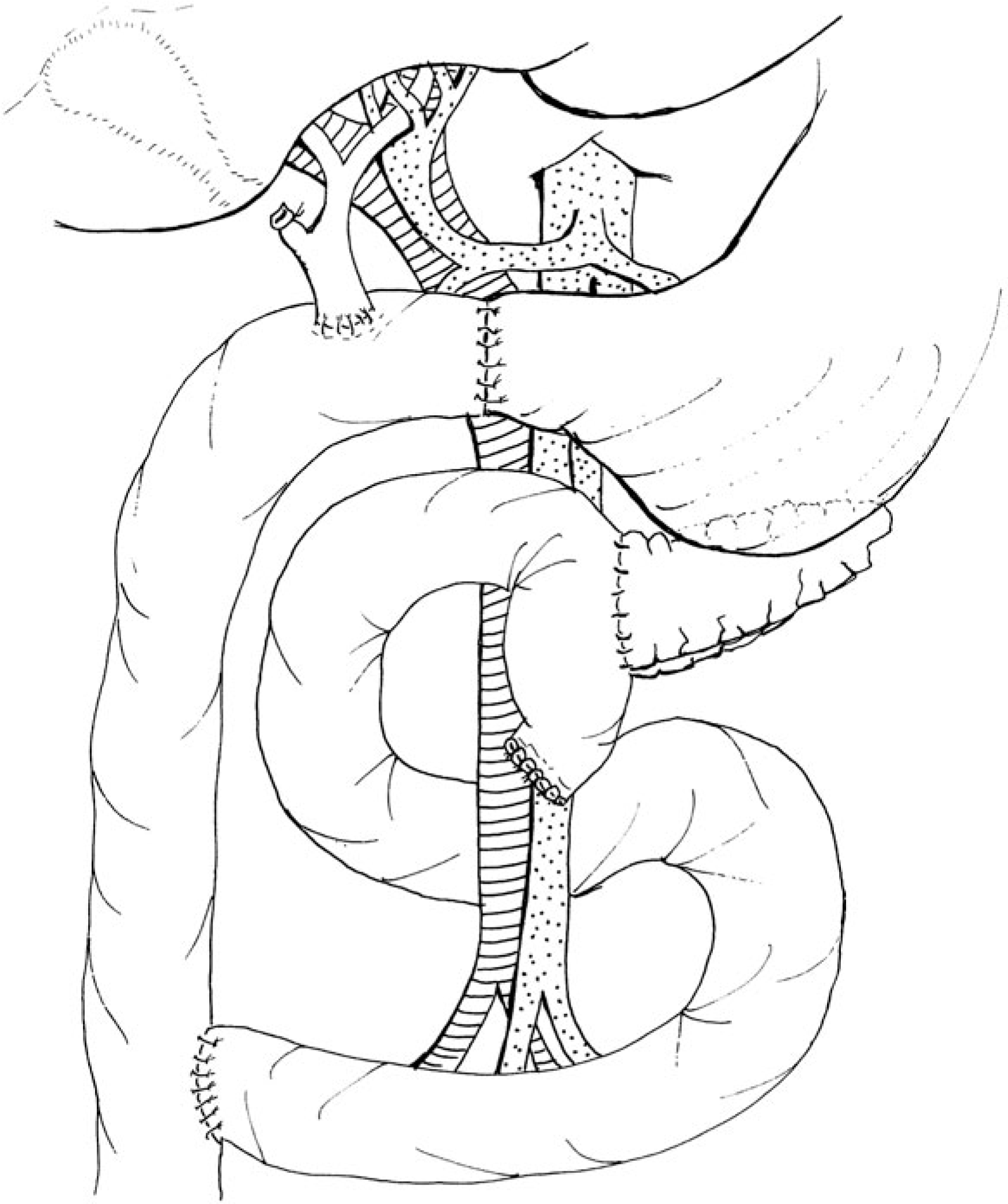
Subsequent reconstruction post-pancreacticoduodenectomy
Distal tumours (body and tail) often present late and less than 7% are resectable. Resection will involve a distal pancreatectomy and generally also a splenectomy to achieve tumour and lymph node clearance. There is evidence that suggests that resection plus adjuvant chemotherapy with gemcitabine may prolong survival.
Palliative care
Patients not undergoing resection for pancreatic cancer should have therapy focused on palliating their symptoms. The majority of patients require symptomatic treatment of pain and/or jaundice.
Pain relief is crucial. Pancreatic carcinoma may initially be painless but pain can quickly progress to become severe and unrelenting. Opioid analgesia should be commenced early and titrated to response using slow-release preparations with the addition of quick-acting preparations for breakthrough. Involve the palliative care team early. Tricyclic antidepressants, coeliac plexus nerve blocks and occasionally radiotherapy (this has no role in altering prognosis) can also be used for pain relief.
Approximately 70% of patients with pancreatic cancer are jaundiced at presentation and the majority of patients with carcinoma head of pancreas will develop it at a later stage. The mainstay of relieving jaundice is by using stents, which are preferably placed endoscopically at ERCP. Rarely, this is not possible and a percutaneous stent may be placed transhepatically under radiological guidance.
In patients who are found to be inoperable at laparotomy, a biliary and duodenal bypass procedure may be undertaken in patients likely to survive more than 6 months. This involves a hepaticojejunostomy, cholecystectomy and gastrojejenostomy for bile and gastric diversion into the jejunum bypassing the CBD and duodenum. This can dramatically improve quality of life by relieving disabling symptoms, particularly pruritis, anorexia and nausea.
Nutrition must also be considered due to anorexia secondary to carcinomatosis. Occasionally, patients require a procedure for gastric outlet obstruction.
For patients with unresectable disease, chemotherapeutic treatments were historically based upon fluorouracil. More recently, this has been replaced with gemcitabine. Gemcitabine has been shown to confer a survival advantage over treatment with fluorouracil (1-year survival rate 18% as opposed to 2%). It is easily administered in the outpatient setting and reasonably well tolerated. However, still only 18% of patients survive a year and only 23.8% of patients perceive any symptomatic improvement. Trials are ongoing combining gemcitibine with other chemotherapies and novel agents.
Considerations in primary care
The majority of HPB units have experienced nurse specialists who are an important link between primary and secondary care.
Patients with pancreatic cancer without prior obstructive jaundice, or with previously treated obstructive jaundice, may subsequently develop a recurrence of their problems secondary to tumour progression or stent blockage. These patients require referral back to the specialist centre for consideration of a bile duct drainage procedure.
Patients with pancreatic cancer are often malnourished. Nutritional supplements may be required and the nutrition team in secondary care usually sees these patients. Appetite stimulants do not tend to be effective but pancreatic enzyme supplements may increase quality of life and symptom scores. There is some early evidence that lipid supplements, particularly fish oil, may reduce weight loss and cachexia.
Depression is a common problem in pancreatic cancer. It can be difficult to differentiate symptoms of depression from symptoms of malignancy such as fatigue and anorexia. Have a low threshold to screen for and treat depression.
Analgesic requirements may be high in patients with pancreatic carcinoma and routine analgesics may be ineffective. In cases where pain is intractable, advice from secondary and palliative care may be appropriate. If the patient agrees, involve the specialist palliative care team early.
Summary of pancreatic cancer
Pancreatic cancer is the fifth most common cause of cancer-related deaths in the UK Overall, 5-year survival is in the region of 1% Patients often present with advanced disease due to early symptoms being vague. A low index of suspicion is required to facilitate prompt referral. Surgery is the only curative treatment but only 10% of patients are deemed resectable at presentation. Surgical resection can yield actuarial survival rates of 18–24% at 5 years Gemcitabine chemotherapy has increased survival rates in unresectable tumours to 18% at 1 year but prognosis remains dismal
Key points
Gallstones (50–75%) and alcohol (25%) are the most common causes of acute pancreatitis in the UK population. Ongoing management in primary care after hospital discharge includes making sure that the causative agent is removed/avoided. The incidence of chronic pancreatitis is increasing and the number one causative agent is alcohol. A significant proportion of patients with chronic pancreatitis progress to severe pain where analgesic requirements may be high and opioid dependency is common, especially with pethidine. Nutrition of patients with chronic pancreatitis is problematic. Patients inevitably require replacement of pancreatic enzymes and may need insulin, which they may be extremely sensitive to. Pancreatic cancer is the fifth most common cause of cancer-related deaths in the UK, with overall 5-year survival in the region of 1% Patients often present with advanced disease due to early symptoms being vague. A low index of suspicion is required to facilitate prompt referral.