
Abstract
Since the first benzodiazepines were marketed in the late 1950s, their use has steadily increased, culminating in one benzodiazepine, diazepam, being one of the most widely prescribed drugs of all time. Often these drugs were prescribed long term for complaints such as anxiety, depression and ordinary life stresses. Since their potential for dependence and addiction have become readily apparent, the question of the correct use of benzodiazepines as anxiolytics and hypnotics by GPs has been hotly debated in the UK. Many doctors still feel more comfortable prescribing benzodiazepines than methadone to problem users. Strategies for discontinuation start with GPs, who are still the main prescribers.
‘Absolute sobriety is not a natural or primary human state’
(Davenport-Hines)
This article outlines
A brief overview of the legal status and pharmacology of benzodiazepines Tolerance and benzodiazepine dependence Management of the benzodiazepine-dependent patient in practice
The GP curriculum and benzodiazepine dependence
Curriculum statement 15.3 dedicates an entire section to drugs and alcohol problems. It highlights that
All GPs have a responsibility for providing general medical care to drug-using adults GPs should be aware of the morbidity (physical, psychological and social) caused by drugs and alcohol An understanding of the difference between dependent and problematic drug and experimental drug and alcohol use Drug use is amenable to treatment, using a combination of psychological, social and medical interventions Our own attitudes and feelings are important determinants of how we manage people who self-harm and misuse drugs or alcohol
Legal status
All benzodiazepines are prescription-only under the Medicines Act 1968. Under the Misuse of Drugs Regulations 1985, benzodiazepines are Class C controlled drugs (Schedule 4) (except temazepam, flunitrazepam and midazolam which are Schedule 3). This means it is illegal to supply the drugs or be in possession of them without a doctor's prescription. Benzodiazepines are classified as Class C under the Misuse of Drugs Act, 1971. All benzodiazepines carry the same penalties (see Box 1).
Misuse of Drugs Act 1971
2 years and/or unlimited fine
5 years and/or unlimited fine
Travelling abroad
There are strict import and export rules concerning benzodiazepines. People carrying with them prescribed controlled drugs in Schedules 2, 3 and 4 (Part 1), and travelling abroad for more than 3 months, require a personal import or export licence for the UK (see website: www.drugs.gov.uk/drugs-laws/licensing/personal). This is not needed for patients travelling abroad for less than 1 month.
Different rules may apply in other countries. Advise travellers to check that entry is allowed with benzodiazepines for medical use with the embassy or consulate of the country or countries to be visited. Controlled drugs should be carried in their original packaging together with a letter from the prescribing doctor confirming the carrier's name, destination, drug details and amounts.
How do benzodiazepines work?
Benzodiazepines act by enhancing the effect of inhibitory gamma-aminobutyric acid resulting in central nervous system depression and psychomotor retardation. Their range of actions includes anxiolytic, sedative/hypnotic, anticonvulsant, amnesic and muscle relaxant. In clinical practice, they are used for the treatment of anxiety and panic disorders, agitated psychoses, insomnia, seizures/some forms of epilepsy, muscle spasticity, alcohol and stimulant withdrawal and as premedication/sedation for surgical procedures.
Tolerance and dependence
Tolerance to benzodiazepines develops to both the therapeutic and non-therapeutic effects at variable rates and to different degrees. Tolerance to the hypnotic effects of benzodiazepines tends to develop rapidly within a few days or weeks of regular use. Hence, after only 2 weeks of regular use, benzodiazepines may become ineffective as sleeping pills. Some poor sleepers may report continued efficacy of benzodiazepines as hypnotics, but this is because they prevent rebound insomnia (a withdrawal effect).
Tolerance to the anxiolytic effect of benzodiazepines seems to develop more slowly, but there is little evidence to indicate that benzodiazepines retain their efficacy for more than 4–6 months of regular use. It is estimated that half of those continually taking benzodiazepines for more than a year do so as a result of dependence rather than because the drug is still medically effective. Again, it is likely that the drugs are preventing withdrawal symptoms rather than reducing anxiety.
Tolerance to the anticonvulsant effects of benzodiazepines also occurs within a few weeks. However, little tolerance develops to the amnesic and cognitive impairment effects caused by benzodiazepines. This is of clinical importance.
Dosage escalation often maintains the cycle of tolerance and dependence (Fig. 1). It is estimated that benzodiazepine use for more than 3 months (and possibly for just a few weeks) is associated with dependence. Box 2 summarizes good prescribing policy to prevent benzodiazepine dependence in primary care.

Factors leading to drug dependence.
Practical tips in benzodiazepine prescribing
Do not prescribe benzodiazepines to someone with a history of drug misuse and dependence Prescribe the lowest possible dose of benzodiazepine and only prescribe for 2 weeks or less Do not add new benzodiazepines onto a repeat prescription unless there is a clear medical reason for this, for example in palliative care Consider alternative strategies instead of prescribing benzodiazepines, e.g. relaxation techniques Advise patients of the risk of dependence when taking benzodiazepines and about impaired reaction times especially when driving or using other machinery Evaluate your practice's current prescribing of benzodiazepines and consider setting up a benzodiazepine reduction programme
When is someone drug dependent?
Substance dependence can be diagnosed with physiological dependence, evidence of tolerance or withdrawal or without physiological dependence. The current Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria are given in Box 3. The key signs of benzodiazepine dependence are withdrawal symptoms on dosage reduction or discontinuation. In practice, this dependence is often inferred in a continuing chronic benzodiazepine user, for example, the reliance on regular prescriptions, dosage escalation and unsuccessful attempts to cut down or stop.
DSM-IV criteria for dependency
Three or more features must be present for at least a year:
Tolerance: a need for markedly increased amounts of the substance to achieve intoxication or desired effect or markedly diminished effect with continued use of the same amount of the substance Withdrawal: the characteristic withdrawal syndrome for the substance or the same (or a closely related) substance is taken to relieve or avoid withdrawal symptoms The substance is often taken in larger amounts or over a longer period than was intended There is a persistent desire or unsuccessful efforts to cut down or control substance abuse A great deal of time is spent in activities necessary to obtain the substance, use the substance or recovering from its effects Important social, occupational or recreational activities are given up or reduced because of substance use The substance use is continued despite the knowledge of having a persistent or recurrent physical or psychological problem that is likely to have been caused or exacerbated by the substance
Are benzodiazepines that bad?
People on long-term benzodiazepines should be advised to stop because inevitable tolerance to these drugs progressively reduces their effectiveness for the treatment of insomnia or anxiety. As little tolerance develops to the amnesic or cognitive effects caused by benzodiazepines, deficits in learning, memory, attention span and visuospatial ability are well documented, particularly in the elderly. Other risks include daytime somnolence, accidents (for example, road traffic accidents), falls and consequences of those falls such as hip fracture.
Rarely, paradoxical disinhibition with benzodiazepines also occurs where there is increased excitement, irritability, aggression, hostility and impulsivity. Dependence may develop, and continuing treatment then serves only to prevent withdrawal symptoms. Benzodiazepines also interact synergistically with other central nervous depressants, including alcohol and opioids. Fatal overdose with benzodiazepines alone is rare, but when it does occur, the combination of benzodiazepines and alcohol, with or without opioids, is often the cause of death.
Stopping long-term benzodiazepines in elderly people has been found to improve their working memory and reaction times, increase levels of alertness, and improve concentration. However, improvements may be slow and may never be complete.
Withdrawal syndrome
The main problem in general practice with benzodiazepine use is undoubtedly the associated with withdrawal syndrome, i.e. when an existing benzodiazepine dose is decreased or withdrawal is attempted. These symptoms can be so poorly tolerated that they preclude the long-term user from ever stopping their benzodiazepine medication (see Table 1).
Common benzodiazepine withdrawal symptoms

Withdrawal effects may develop from 1 day to 3 weeks after suddenly stopping benzodiazepines, with the time lag corresponding to the half-life of the particular benzodiazepine. Withdrawal severity correlates with prolonged or high-dose use and short-acting, potent benzodiazepines. Some symptoms may continue for weeks or months after stopping benzodiazepines. Often these expected self-limiting withdrawal symptoms may resemble the original complaint (e.g. relapse of prior insomnia or anxiety), and both patient and the doctor may be tempted to continue benzodiazepine medication as a result.
Patient types
In the surgery, there are two groups of patients who are likely to become benzodiazepine dependent:
the inadvertent long-term user who does not abuse their prescription—i.e. therapeutic dose dependence and those that abuse or use benzodiazepines illicitly, often associated with a polysubstance abuse pattern
This distinction is important since management differs.
Driving and benzodiazepines
People who take benzodiazepines at doses recommended by the British National Formulary and have no evidence of impairment do not need to inform the Driver and Vehicle Licensing Agency, although clinically dependence may exist. The non-prescribed use of benzodiazepines or the use of supratherapeutic dosage, whether in a substance withdrawal/maintenance programme or otherwise, constitutes misuse/dependency for licensing purposes (see Table 2).
Benzodiazepine misuse and/or dependency and fitness to drive

Consideration of benzodiazepine withdrawal
Before embarking on discontinuing benzodiazepines, assess whether this is a suitable time for the person to stop taking the drug. The chances of success are improved when a person's physical and psychological health and personal circumstances are stable. In some circumstances, it may be more appropriate to wait until other problems are resolved or improved before starting drug withdrawal.
Enquire about symptoms of depression and anxiety. Discontinuing benzodiazepines can worsen symptoms of clinical depression and anxiety and it may be worthwhile treating these underlying conditions first.
Consider whether the withdrawal of the benzodiazepine can be appropriately managed in primary care. Seek specialist's advice or refer to a specialist centre for people with
a history of alcohol or other drug use or dependence a concurrent, severe medical or psychiatric disorder or personality disorder or a history of drug withdrawal seizures
The inadvertently benzodiazepine-dependent patient
Many long-term users of benzodiazepines become inadvertently dependent. This group does not abuse their prescription and patients are dependent at therapeutic doses. Box 4 outlines some suggestions on how to tackle this problem in the surgery.
Management of benzodiazepine dependence in a non-abusing patient
Make the diagnosis of dependence if the patient fits the criteria Begin with advisory letters and patient information Offer a consultation with a GP or practice nurse. Provide education on why long-term benzodiazepines are harmful. Explain the difficulties that may arise with continued prescribing. Benzodiazepines should not be withdrawn abruptly because there is a risk of seizures, confusion or paranoid psychosis Graded discontinuation:
Consider changing to diazepam Reducing regimens vary and should be individually adjusted to the patient's needs; a reduction of one-eighth to one-tenth of the daily dose every 1–2 weeks is suggested. If withdrawal symptoms develop at the reduced dose, then consider going back to a higher dose for a while. The rate of withdrawal is determined by the patient's capacity to tolerate symptoms. Warn the patient of expected self-limiting withdrawal symptoms, as these may be misconstrued as relapse of prior insomnia or anxiety Follow-up regularly Consider adjuvant therapy in all patients, e.g. cognitive behavioural therapy and relaxation
In Denmark, new regulations have restricted prescriptions of hypnotics to only 1 month at a time and only after a consultation; renewal of prescriptions by telephone is not allowed. Studies showing prescribing cost data have shown that simple practice audit of benzodiazepine prescribing can achieve a significant reduction in the volume of drugs dispensed. The help of a community pharmacist is invaluable. Advice from the GP together with a self-help booklet, or a letter from the GP suggesting a reduction in the use of benzodiazepines, and ways to tackle drug reduction can also have a significant impact.
How do I switch from a benzodiazepine to diazepam?
Switching to diazepam prior to withdrawal is recommended, particularly if people have difficulty withdrawing or if they are dependent on short-acting, potent benzodiazepines such as alprazolam or lorazepam. In other cases, it is reasonable to try benzodiazepine withdrawal without switching to diazepam. A Cochrane Review in 2006 concluded that withdrawal from short half-life benzodiazepines was associated with a higher dropout rate, but withdrawal symptoms were no more severe than with withdrawal from longer acting benzodiazepines.
A dose conversion table is given in Table 3. This equivalence is based on clinical experience of withdrawal schedules, not on equivalent efficacies. In the same way, a complete dose substitution may not always be required, depending on the individual response. Dose withdrawal may be started when conversion to diazepam is complete.
Dose conversion table for equivalent doses of benzodiazepines to diazepam 5 mg
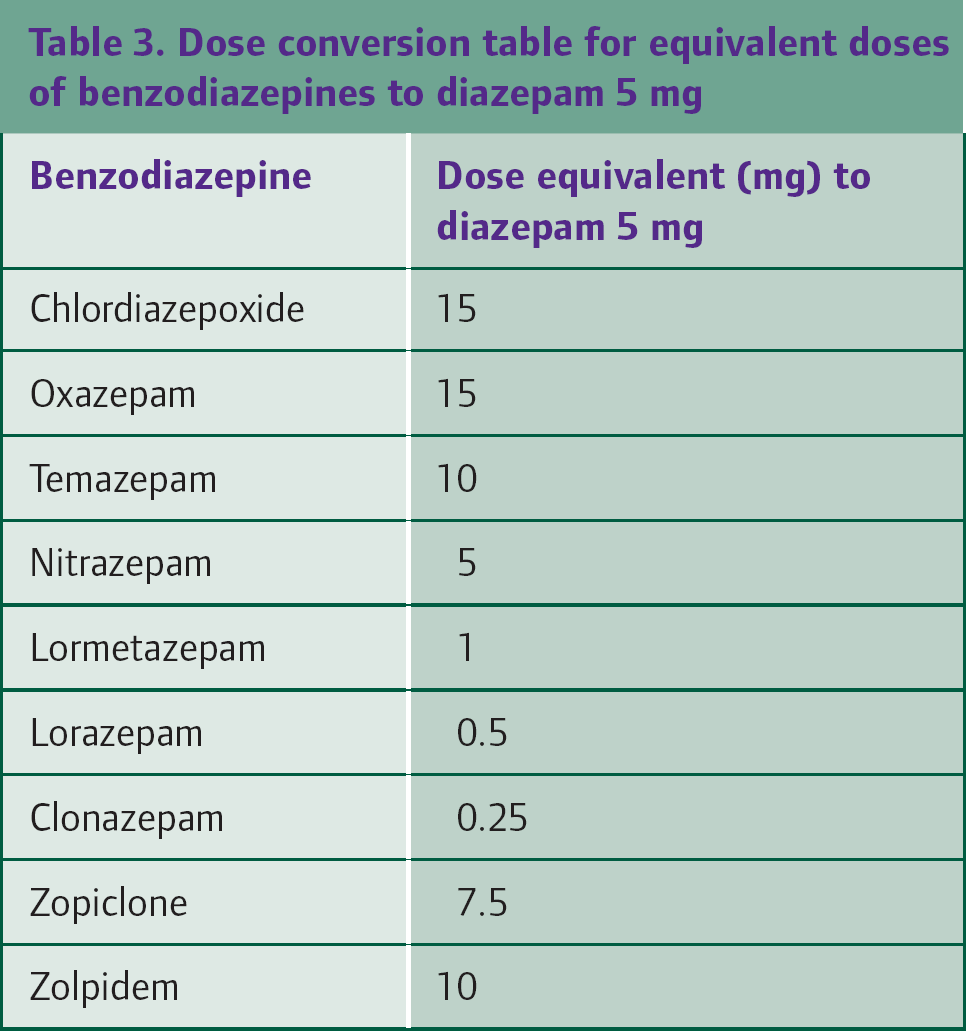
If switching to diazepam in people with hepatic dysfunction seek specialist advice as diazepam may accumulate to a toxic level in these individuals. An alternative benzodiazepine without active metabolites (such as oxazepam) may be preferred.
Controlled withdrawal of benzodiazepine dose
Rate of benzodiazepine withdrawal is a contentious and poorly researched issue, but several small studies have shown that people who gradually withdraw benzodiazepines have a higher cessation rate and less symptoms of withdrawal, than those who stop abruptly.
The early stages of withdrawal are easier to tolerate than later stages. Stopping the last few milligrams is particularly difficult and often requires a slower reduction in dosage. Remind the person that reducing benzodiazepine dosage, even if this falls short of complete drug withdrawal, can still be beneficial.
The optimal duration of controlled withdrawal is not clear and may vary from patient to patient. In most patients, a brisk schedule is possible (8–12 weeks) but this should be tried with the flexibility of slowing down if symptoms are not well tolerated. In patients who have tried but failed to withdraw previously, a 6 month schedule may be necessary. In most cases, it is possible to stop completely when a very low dose (e.g. diazepam 1 mg daily) is reached.
Drug treatment of benzodiazepine dependence
There is no ‘gold standard’ treatment for benzodiazepine dependence. Antidepressants or mood stabilizers, such as carbamazepine, valproate, mirtazapine and trazodone, may be helpful under specialist supervision. This probably reflects the finding of co-morbid depression. In particular, carbamazepine (200–800 mg/day) may reduce withdrawal severity in patients receiving the equivalent of diazepam 20 mg/day; however, further studies are needed.
The ‘z-drugs’ (zopiclone and zolpidem) should not be used as there have been increasing reports of abuse and addiction. At present there are mixed views on flumazenil (initially thought of as a pure benzodiazepine antagonist). Some suggest that it may alleviate withdrawal symptoms, others have clearly shown that this is not to be the case. Currently, flumazenil is not recommended in the primary care setting.
Management of expected withdrawal symptoms
Warn the patient of expected self-limiting withdrawal symptoms, as these may be misconstrued as relapse of prior insomnia or anxiety. Box 5 outlines advice to give to patients undergoing withdrawal.
What should I advise people undergoing withdrawal?
Inform the person that nearly all the acute symptoms of withdrawal are those of anxiety Explain that some of the withdrawal symptoms may be similar to the original complaint and do not indicate a return of that complaint It is not possible to estimate the severity and duration of withdrawal symptoms, as these will depend on a number of factors, such as severity of dependence and speed of withdrawal For most who withdraw from treatment slowly, symptoms are mild and can usually be effectively managed Reassure patients that they will be in control of the drug withdrawal and that they can proceed at a rate that suits them Reassure patients that they can try again if they do not succeed at their first attempt Advise patients to avoid taking extra tablets in times of stress or compensating by increasing intake of alcohol
Symptomatic treatment of withdrawal symptoms during gradual tapering of the benzodiazepine dose is recommended. The three symptoms that predominate are anxiety, depressive symptoms and insomnia. Table 4 summarizes the symptomatic treatment of common withdrawal symptoms. However, often withdrawal symptoms are difficult to treat. For example, muscle spasms may not respond to muscle relaxants. Take care in treating symptoms of withdrawal not to substitute one drug dependency for another.
Management of expected withdrawal symptoms

Psychological interventions
Patients with benzodiazepine dependency are often worried by possible withdrawal symptoms, and may feel ill-equipped to deal with them. Psychological interventions range from simple support through counselling to expert cognitive behavioural therapy. A key worker accessed through the local drug and alcohol services may be very helpful.
Self-help support measures can be helpful for both patients and their families and carers. Battle Against Tranquillizers (website: www.bataid.org) provides a telephone help line, support groups, advocacy and drop in centres. Benzodiazepines Co-operation Not Confrontation (website: www.bcnc.org.uk) provides information about inadvertent benzodiazepine dependence. The Tranquilliser Recovery and Awareness Place (website: www.non-benzodiazepines.org.uk) provides further information and also an online forum for patients and carers.
Evidence from two meta-analyses indicates that gradual benzodiazepine withdrawal combined with psychological interventions is more effective than usual care or gradual withdrawal alone. However, these findings should be interpreted with caution as the studies were generally small and heterogeneous.
How do I manage someone who does not want to stop taking benzodiazepines?
Many patients who have taken benzodiazepines for years are reluctant to stop. Listen to their concerns and try to address the issues that they raise. Discuss the benefits of stopping and explain tolerance, the adverse effects of benzodiazepines and the risk of continuing the drugs. Even if patients refuse to consider benzodiazepine withdrawal, encourage dose reduction as even small reductions in dosage are beneficial.
Abusing or illicit benzodiazepine users
Abuse or illicit use of benzodiazepines is often associated with polysubstance abuse. Medical prescriptions constitute the primary source of supply for people who abuse benzodiazepines and abusers may obtain their supplies directly from GPs or buy diverted prescribed supplies from dealers. Individuals may try to get prescriptions for benzodiazepines from practices both for their own usage and to sell the prescriptions. They may try to do this by deceit, for example by taking on multiple false identities and shopping around GP surgeries as a temporary resident, often with a story of forgotten or lost medication. This is a big problem for GPs and alerts about such patients are frequently cascaded to practices.
When confronted with such patients in the surgery, the responsibility for whether a prescription is issued lies with the prescribing GP. However, many GPs feel very uncomfortable in this situation. Refusing to prescribe might result in confrontation, but prescribing is opposed to the usual principles of benefits outweighing risks, and sets a difficult precedent for that practice and other GPs.
In most cases it is best not to prescribe. Many people continue to buy from dealers on top of any prescription given as they consume high doses and often mix benzodiazepines with other drugs to create the so-called ‘cocktail effect’. Maintenance prescribing of benzodiazepines has not been shown to have any definite medical value and is rarely justified.
If the individual wants to withdraw from benzodiazepines, a different approach is required (Box 6). Use this opportunity to assess dependence on other substances, such as alcohol, and refer to the specialist drug and alcohol services for advice and support. Inpatient detoxification may be required.
A comprehensive approach
Few conditions exemplify more clearly than benzodiazepine abuse the need for a generalist holistic approach to a problem. GPs may often come into contact with users at a relatively early stage in their drug-taking career. Often individuals with drug dependence lead chaotic lives and have multiple problems—depression, infection, poor diet, poor hygiene, childhood abuse, crime and/or unemployment. Try to use this opportunity to discuss physical health problems, possible offending behaviour and mental health well-being. Be aware of the extent and implications of stigma and social exclusion.
Management of dependence in abusing or illicit benzodiazepine users
Assess whether patients are motivated to change at least some aspect of their drug abuse Avoid prescribing benzodiazepines if at all possible—determine exactly what is needed and consider alternatives If you do decide to continue prescribing, then continue with safeguards in place, e.g. daily or weekly dispensing Adhere to local protocols If a prescription has been lost or the drugs have been used up before the next prescription is due, they should not be repeated Confront the patient with whatever evidence of drug abuse you have Consider a urinary drug screen to detect if other drugs of abuse are being used A dose above 30 mg diazepam daily is rarely needed and this dose is sufficient to prevent withdrawal seizures whatever dose has been taken previously A key worker provided through the local drug and alcohol service is invaluable to address psychosocial issues, e.g. housing problems
Hidden harm
It is important to recognize the vulnerability of children whose parents are drug users; children are at increased risk of accidents, physical and emotional abuse, poverty, inadequate parental supervision, separation, frequent changes of residence and risks associated with toxic substances; often the child may adopt the role of carer in such circumstances. That said, parental drug use in isolation does not automatically correlate with poor parenting and many drug users do manage to provide good parental care, especially if they receive appropriate treatment. Focus on the quality of parenting overall rather than exclusively on drug use.
Key points
Distinguish long-term benzodiazepine use that might be justified because of symptomatic treatment of the underlying disorder from long-term use reflecting chronic dependence—use DSM-IV criteria Use the opportunity to discuss their overall physical and mental well-being—be aware of concurrent depression Benzodiazepines should not be withdrawn abruptly; negotiate a step-wise, flexible reduction programme Non-drug strategies range from simple audit, patient education, advice to tapering off, to cognitive behavioural therapy Adjunct medication is not firmly established; only weak evidence supports the use of other medications such as carbamazepine Regular follow-up and review of symptoms and benzodiazepine dose
Additional information
The RCGP runs a Certificate in the Management of Drug Misuse. Part 1 is aimed at the generalist GP and Part 2 at the practitioner with a special interest. More details are available at website: www.rcgp.org.uk