
Abstract
Everybody regardless of age, ethnic background or socio-economic group has had at least one respiratory tract infection (RTI) in their lifetime and a quarter of the population will visit their GP with RTIs each year. Before antibiotics, secondary complications of usually self-limiting RTIs, such as pneumonia and quinsy, could be fatal. The discovery and development of penicillin by Fleming in the 1920's made antibiotics a lifesaver and they became increasingly prescribed for minor, usually self-limiting illness to prevent these complications. Over the years the cycle of medicalising self-limiting illness has continued. For example parents of children with otitis media are 30% more likely to attribute the improvement in the child to the antibiotics and not to their child's own immune system.
The GP curriculum and antibiotic prescribing
Antibiotic prescribing is covered directly in three GP curriculum statements:
In addition,
Recognising that patients are diverse, and that their behaviour and attitudes vary Respond flexibly to the needs and expectations of different individuals Negotiate a shared understanding of the problem and its management with the patient, so that he or she is empowered to look after his or her own health Manage the potential conflicts between personal health needs, evidence-based practice and public health responsibilities.
Despite education and public health initiatives 60% of total antibiotic prescriptions are for RTIs (NICE CG69, 2008). Patients may directly request scripts but overall evidence suggests that GPs overestimate the proportion of patients who expect antibiotics. We currently prescribe more antibiotics than any other northern European country. There is no evidence that we have any lower complication rates as a result.
NICE has developed a guideline for RTIs with a strategy to reduce unnecessary antibiotic prescribing (NICE CG69, 2008). The guidance addresses five common RTIs. These are: acute otitis media, acute pharyngitis or tonsillitis, the common cold, acute rhinosinusitis and acute cough/bronchitis. This article summarises the guidelines and offers some suggestions on how to apply them to everyday practice.
The evidence
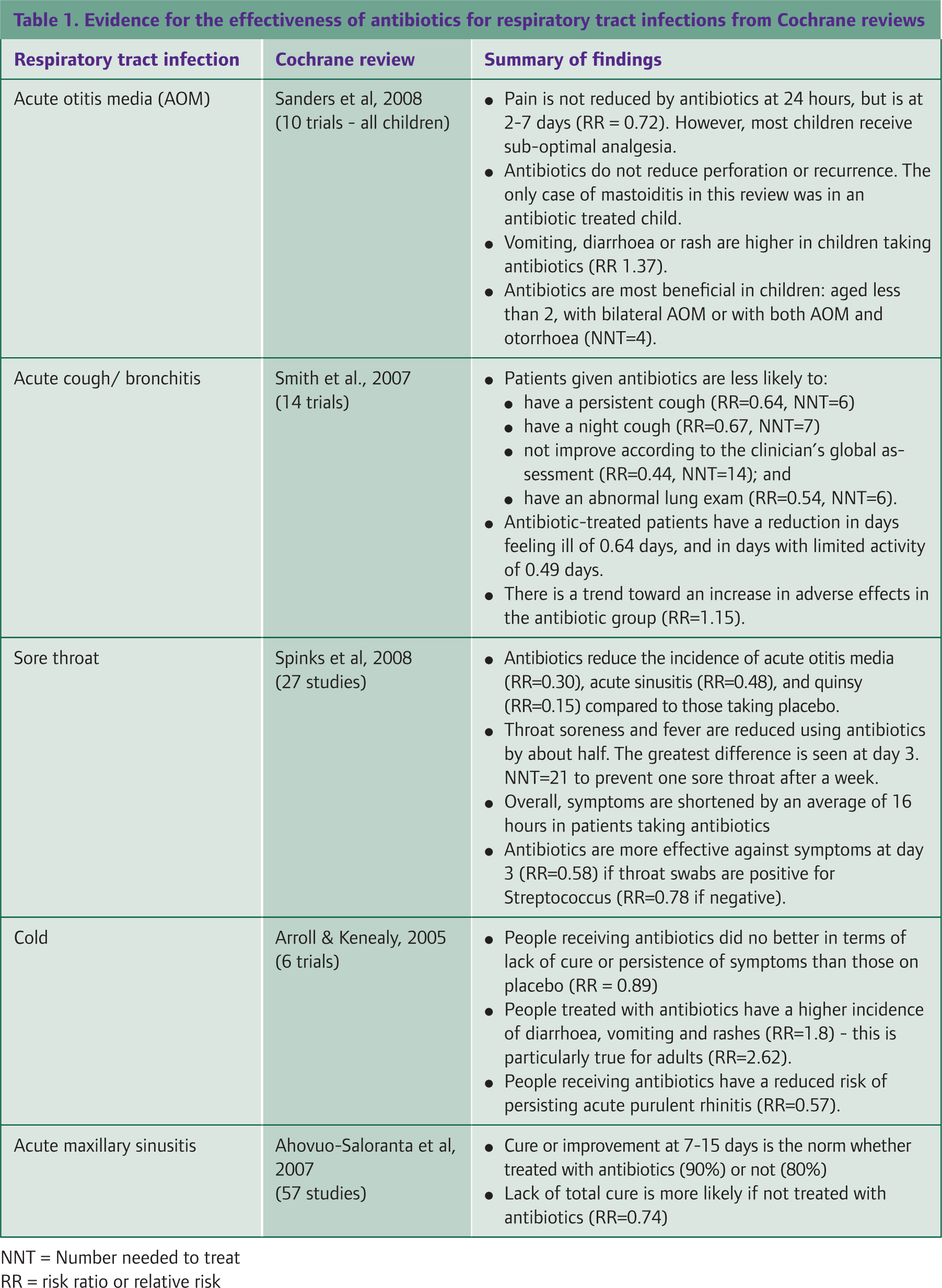
The NICE guidance outlines best practice, which starts with a thorough assessment. To be well informed, patients need to be aware of the aetiology of their condition, the natural history, the options available (either no antibiotics, antibiotics or a delayed prescription) and the risks and benefits of each treatment option. Table 1 outlines the evidence behind the NICE recommendations for treatment of these conditions, drawing on recently published systematic reviews.
Evidence for the effectiveness of antibiotics for respiratory tract infections from Cochrane reviews
All antibiotics have adverse effects. First, there is always a possibility of side effects. Common side effects of antibiotics include diarrhoea, vomiting and skin rashes. For example, a skin rash occurs in 3–10% of patients prescribed penicillin. More severe side effects are much rarer but fatal anaphylaxis attributed to penicillin allergy accounts for between 3–4 deaths per year in the UK.
Drug interactions with antibiotics are also common. For example, patients should be advised not to take their statin when prescribed a macrolide antibiotic such as erythromycin due to an increased risk of myositis, and co-prescription of trimethoprim with methotrexate enhances the cytotoxic effect of methotrexate and can lead to fatal pancytopoenia. The most common drug interaction with antibiotics seen in the GP surgery is between antibiotics and the combined oral contraceptive pill. Broad spectrum antibiotics such as amoxicillin interfere with absorption of the combined oral contraceptive by affecting gut flora thus making it ineffective. Women should be advised to use additional contraception (usually a barrier method) during the course of antibiotics and for 7 days afterwards, omitting the pill-free interval if the 7 days runs beyond the end of the packet.
There is also some evidence that indiscriminately prescribing antibiotics is not only expensive to the NHS, but can increase the primary care consultation rate for minor illnesses. Prescribing for a condition that is likely to get better anyway increases the patient's faith in antibiotics, thus encouraging future reattendance at the GP surgery with minor self-limiting illness. High levels of prescribing of antibiotics in the community, in turn increases community antibiotic resistance, making infections harder to treat.
However, antibiotics do also have beneficial effects. They give a modest benefit in symptom relief for patients with minor self-limiting illness (for example, 16 hours less symptoms for sore throat), and may confer slight protection against some complications such as quinsy, and pneumonia. Whether to prescribe antibiotics or not is a matter of weighing the risks of prescribing against the benefits for the individual patient. For most patients, the magnitude of the beneficial effect of antibiotics is outweighed by the adverse effects of prescribing. However, NICE identifies high risk groups where the benefits of prescribing antibiotics exceed the risks (NICE CG69, 2008). These groups should receive antibiotic treatment without delay (Box 1 and Table 2).
Respiratory tract infections: duration, acute infective complications and antibiotic treatments of choice

Treat with antibiotics if purulent discharge for more than 7 days
The Centor criteria (Centor et al, 1981) were developed to help clinicians determine the likelihood of a sore throat being secondary to a group A beta-haemolytic streptococcal infection (GABHS). GABHS sore throat should be treated with antibiotics as the evidence for beneficial effect on symptoms is greater, and the incidence of serious complications, such as generalised septicaemia, is higher in this group. Patients need to have all four symptoms/signs present:
tonsillar exudate tender anterior cervical lymphadenopathy history of fever, and absence of cough.
The presence of all four clinical features has a low positive predictive value of 40% for a throat swab to test positive for Group A Streptococcus, but the absence of all four variables has a negative predictive value of greater than 80%. Therefore, this scoring system is better for ruling out a streptococcal sore throat than proving it.
Delayed antibiotics
Delayed prescribing as a concept has been around since the 1990s. It is an important and effective safety-net strategy for patients who are used to receiving antibiotics for self-limiting illnesses, and does not result in an increased rate of complications. Delayed prescriptions reduce antibiotic usage by 63–80% compared to immediate prescription. For patients who are expecting to receive immediate antibiotics during a consultation, 70–90% who receive a delayed prescription for acute RTIs instead are satisfied and would choose to receive a delayed prescription again in the future.
Patients are more likely to be satisfied if counselled effectively that the risks associated with antibiotics outweigh the potential benefits using a shared decision making model. A delayed script can be given to the patient or left at an agreed location to be collected at a later date. Patients should be advised to use the delayed script if they experience significant worsening of symptoms, new symptoms that suggest complications or if the illness lasts longer than the expected course (NICE CG69, 2008). It is important to ensure that they know to re-consult if they have any concerns.
Managing symptoms
Simple conservative measures are all that are needed to manage uncomplicated respiratory tract infections. Paracetamol and/or ibuprofen can be used to manage headaches, aches, pains and fever. Suggest plenty of fluids and rest from normal activities.
Indications for immediate prescribing of antibiotics
Offer immediate antibiotics or further investigation/management for patients who:
are systemically very unwell have symptoms and signs suggestive of serious illness and/or complications are at high risk of serious complications because of pre-existing comorbidity. This includes:
patients with significant heart, lung, renal, liver or neuromuscular disease immunosuppressed patients patients with cystic fibrosis young children who were born prematurely are older than 65 years with acute cough and two or more of the following, or older than 80 years with acute cough and one or more of the following:
hospitalisation in previous year type 1 or type 2 diabetes history of congestive heart failure current use of oral glucocorticoids
Depending on clinical assessment of severity, consider offering immediate antibiotics for:
children younger than 2 years with bilateral acute otitis media children with otorrhoea who have acute otitis media patients with acute sore throat/acute pharyngitis/acute tonsillitis when three or more Centor criteria are present.
Although self-medication does have a role in reducing the burden on primary care, there is little evidence for many of the other symptom-control remedies sold in supermarkets and pharmacies. For example, Smith, Schroeder & Fahey (2008) in a Cochrane review concluded that there was no evidence supporting the use of over-the-counter cough medicines. GPs should not recommend purchase of over-the-counter medicines of unproven effectiveness, and when asked about them should ensure that patients are aware of the lack of evidence to support their use.
Case study 1
Karl is a 38-year-old primary school teacher. He has developed a sore throat and a cough over the last 24 hours. He thinks he has probably caught it from one of his pupils.
His grandfather recently had a valve replacement and spent a long time in hospital. His grandfather developed rheumatic fever from tonsillitis when he was a child and this has lead to heart problems. Karl went on the Internet last night to look at the link between rheumatic fever and sore throats. He is now very concerned that he is going to get heart, brain and joint problems if this remains untreated.
On examination he has a mildly red throat with scanty lymph nodes in the anterior cervical chain. His chest is clear. Karl scores one out of our on the Centor criteria.
You discuss with Karl the decreasing incidence of rheumatic fever in the past century and its rarity now, and also his feelings about his grandfather's illness. After some information on the risks and benefits of prescribing antibiotics for sore throat, Karl is happy to leave without antibiotics. You give him a leaflet about sore throat and self-management strategies and advise him to come back if he is not improving within a week or worried meanwhile.
Case study 2
Jessica is a 15-year-old young woman who is brought in by her mother after developing a non-productive cough 10 days ago. She has no other past medical problems and her last few consultations this year have been with viral illnesses.
Jessica is still managing to play netball after school but generally feels a bit tired and under the weather. There is nothing to find on examination.
Her mother leads the conversation. Jessica is 2 weeks away from sitting her first GCSE exam. Her mother demands antibiotics as she does not want Jessica running the risk of not getting A* in her exams. She feels that there must be a more serious cause than ‘just a virus’ because she has had it for over a week.
You feel quite intimidated by Jessica's mother but try to focus on Jessica as the patient. You reassure both Jessica and her mother that there are no features that might suggest anything other than a minor, self-limiting respiratory infection. You discuss the risks and benefits of antibiotics and normal duration of symptoms of an uncomplicated acute cough. You explain that even in those treated, on average antibiotics reduce durations of symptoms by less than a day.
Jessica appears quite happy with this explanation and comments that her mother is more stressed than she is about her exams.
You offer a delayed script so that if Jessica is not improving within the next week, she could have some antibiotics before her exams.
The H1N1 (swine flu) pandemic
We are currently in the treatment phase of an influenza pandemic. In terms of antibiotic prescribing, the suggestions within this review are applicable. However in addition you should consider the possibility of reducing length of illness and infectivity with prescription of an antiviral. For most, oseltamivir (Tamiflu®) is the drug of choice but this is contraindicated in pregnancy. For pregnant women consider prescription of inhaled zanamivir (Relenza®).
Patients meet the criteria for antiviral treatment if they have a temperature over 38°C and have symptoms of flu, such as cough, aches and pains, sore throat and/or loss of appetite. Most patients can obtain supplies of antiviral via the National Pandemic Flu Helpline or on-line at their website (www.direct.gov.uk/pandemicflu) without seeing a GP. Patients most severely affected by the virus and most at risk of complications include children under a year old, those with chronic illness or who are immunocompromised, and pregnant women. Particular care should be taken with these groups, so have a low threshold for medical review. The Health Protection Agency (website: www.hpa.org.uk) is providing regular updates to information about this pandemic and your surgery will be aware of local guidelines.
Dealing with the ‘inner consultation’
Discussions about minor illnesses can be very frustrating especially if you are busy and stressed. Keep in mind that patients believe antibiotics will help because of years of misuse and prescriptions, and it takes time to challenge these health beliefs. Try and establish why the patient is consulting now by identifying their ideas, concerns and expectations. This allows an open discussion about why the patient has consulted, what they know about antibiotics and what they want. These skills are challenging and can be practised during Consultation Observation Tools and Case Base Discussions, providing points for discussion with your trainer.
Consultation skills
Everyone has their own specific consultation style and what makes our job interesting is that we use different techniques for different sets of patients. The suggestions included here are by no means prescriptive but may provide food for thought. Case study 4 describes a worried mother who brings a child to the GP surgery expecting an antibiotic prescription. Think about how you would deal with this, and all the other case studies included in this article, in your consultation. Boxes 2 and 3 describe different ways of communicating the evidence base - one paternalistically and one in an empathic, patient-centred way.
Case study 3
Kathleen is a 56-year-old divorcee who works shifts at the local call centre. She attends from time to time with vague symptoms. Today she attends with blocked sinuses and lethargy. She is quiet by nature and not keen on seeing the doctor.
She has been feeling very low for the past 2 months and is increasingly disillusioned with her job. She is waking up early in the morning and is unable to get back to sleep. She cannot be bothered with anything and when she tries to do something she finds no joy in it and can get distracted quickly. She thinks that her sinuses are to blame and is keen for an antibiotic ‘tonic’ to make her better.
You immediately wonder if Kathleen is subconsciously seeking help for more serious underlying psychological problems as patients will often present with minor problems when their coping skills are at a low ebb. Physical examination is entirely normal so you do a PHQ-9 depression score. This shows that Kathleen has moderately severe depression.
You explain to Kathleen that she has no features to make you think that she has a serious sinus infection, that antibiotics are unlikely to help and might even give her unwanted side effects. You explain the link between depression and physical symptoms which gives Kathleen the opportunity to talk about her low mood.
Case study 4
Kerry is a mother of three children under 8. She consults you because Chloë, her youngest at age 18 months, has developed a cold. Chloë has been sneezing, has had a runny nose for the past 3 days and has been a bit clingy. She is however, eating well, has normal wet nappies and has no cough, drowsiness or skin rashes.
When Chloë's sister Natalie was this age she developed pneumonia and had a spell in hospital. Kerry found the process very stressful as, at the time, she had put her condition down to a cold. The only thing that worked with Natalie was a course of antibiotics and Kerry wants them for Chloë to prevent her from getting pneumonia.
Kerry is currently estranged from Chloë's father and the breakdown of the relationship is a source of a lot of angst. Often arguments involve a lot of negative criticisms about her ability to care for their children.
The paternalistic approach
Kerry: “It's Chloe she's really poorly - she's got a runny nose and is not herself. I'm really worried”
Doctor: “She's got a cold then?”
Kerry: “I'm not sure, it's just not like her”
Doctor: “Well has she any other symptoms? Cough, wheeze, breathing problems, anything else? Is she eating?”
Kerry: “Err, yeah she's eating alright”
Doctor: “Normal wet nappies?”
Kerry: “Err yes”
Doctor examines Chloe
Doctor: “Well it's just a cold – paracetamol, fluids and she'll be better in no time
Kerry: “Oh ok. Doesn't she need antibiotics?”
Doctor: “No she doesn't, anything else?”
Kerry: “No thanks”
The patient-centred approach
Kerry: “It's Chloe she's really poorly - she's got a runny nose and is not herself. I'm really worried
Doctor: “Has she any other symptoms? Cough, wheeze, breathing problems, anything else? Is she eating?”
Kerry: “Err, yeah she's eating alright”
Doctor: “Normal wet nappies?”
Kerry: “Err yes”
Doctor examines Chloë
Doctor: “Well I can't find anything but a simple cold. You should give her some paracetamol - regularly whilst she's miserable - and make sure that she's drinking plenty of fluids. She should get better over the next week to 10 days.
Kerry: “Oh ok ‥…so she doesn't she need antibiotics?”
Doctor: “Why do you want her to have antibiotics?
Kerry: “Um, they worked when Natalie was ill”
Doctor: “Natalie is your older daughter?”
Kerry: “Yeah, she had pneumonia. I was so scared. I don't want that again.”
Doctor: “Well I can understand why you're worried but everything that I have found today makes me think that Chloe is fighting off this cold very well on her own. Giving antibiotics doesn't mean that she'll get any better faster and she might even get side effects from them.”
Kerry: “But what if she gets worse?”
Doctor: “If you are worried that she is getting worse, you should either call the surgery and ask to speak to a doctor or ask to be seen again. …we always have emergency appointments for sick children. If the surgery is closed, you can either ring NHS direct or our emergency number which you can get from the front desk on your way out.” Kerry “So I can ring back tomorrow morning if she's worse? I guess that's OK then.”
Reflection
Using the paternalistic approach (Box 2), the doctor may have made the right diagnosis and treated Chloë according to the NICE guidelines, but has he elicited Kerry's agenda?
She still has no further skills to help manage Chloë in the next few days and may go home and still worry about pneumonia. This may cause her to seek help elsewhere, for example through an inappropriate attendance at the Accident and Emergency department, and contribute towards inappropriate health seeking behaviour in the future.
By being more alert to Kerry's perspective, and responding to the cues that Kerry has put into her conversation, the doctor using the patient-centred approach (Box 3) has not only made the right diagnosis and treated Chloë according to the NICE guidelines, but has also:
explained why antibiotics are not always the best thing to treat a cold with provided Kerry with information about how long she might expect the symptoms to last addressed Kerry's hidden underlying concerns about not treating the cold with an antibiotic, and provided Kerry with a strategy of self-management with an appropriate safety-net should Chloë get worse.
This will empower Kerry to manage her childrens' minor respiratory infections herself in future and encourages her to use primary care services sensibly.
Key points
60% of total antibiotic prescriptions in the UK are for respiratory tract infections. Most patients with minor respiratory tract infections do not need antibiotics. With good communication skills these patients will be satisfied and accept no prescription or a delayed prescription. There are some patients who need antibiotics on presentation - these include patients with other illnesses, the elderly with risk factors for severe disease, patients with severe illness. Consider immediate prescription in patients under the age of 2 with bilateral otitis media, patients with otitis media and otorrhoea, and patients with sore throat who fulfil the Centor criteria. For all patients, whether prescribing antibiotics or not, ensure adequate safety netting should symptoms not improve within expected limits, or deteriorate.