
Abstract
Although they do not account for a large proportion of reasons for consultation with a GP, knowledge of conditions affecting the penis is important. The sensitive nature of these conditions means that doctors need to be confident in order to minimize embarrassment to the patient and to successfully diagnose and manage such problems. The aim of this article is to highlight the conditions most frequently seen in primary care and to introduce a few others which often require referral to secondary care.
The GP curriculum and conditions affecting the penis
This article will address various aspects of the curriculum, specifically seeking to explore the following statements:
Curriculum statement 10.2: Men's health. This requires familiarity with the symptoms of a sore or painful penis, penile ulceration and erectile dysfunction. Knowledge is also required about circumcision (for both religious and non-religious reasons), sexually transmitted infections and acute management of paraphimosis and priapism.
Curriculum statement 11: Sexual health. This requires familiarity with the symptoms of genital skin conditions, including rashes, ulcers and lichen sclerosus and penile urethral discharge.
Penile skin conditions
The penis can be affected by dermatological conditions just like any other area of skin. Common conditions include lichen simplex, atopic dermatitis, seborrhoeic dermatitis, psoriasis, lichen sclerosus or lichen planus. These can generally be identified through the presence of the skin condition elsewhere on the body. Due to the moisture environment, the skin lesions may appear slightly atypical but diagnosis should be apparent from the lesions elsewhere. Most of these conditions present as itching, although there may also be soreness.
Lichen planus may cause scarring if untreated. Lichen sclerosus (sometimes called balanitis xerotica obliterans) is important to diagnose because if longstanding and untreated, there is a 5% incidence of malignant change in the form of squamous cell carcinoma. Lesions are usually found on the foreskin, coronal sulcus and glans penis and appear as white areas. It can cause pain with erections due to tightening of the skin, and there is the risk of phimosis.
Penile pearly papules (see Fig. 1) are small skin-coloured lumps that are usually located on the glans penis. They are often all the way around the head of the penis, sometimes in rows. These can be mistaken for molluscum contagiosum or genital warts. Treatment is not necessary, and if cosmetic treatment is undertaken, there is a risk that scarring may occur.

Penile pearly papules.
Peyronie's disease occurs due to asymmetrical fibrosis in the connective tissue of the penis. It occurs more often on the upper than the lower side of the penis. Severity of cases varies, ranging from redness and inflammation to a hardened plaque that causes the penis to bend when erect. It may also be associated with Dupuytren's contracture. On examination, there is a palpable lump. In many cases, Peyronie's disease resolves spontaneously, often within 2 years, but in severe or persistent cases, surgical intervention may be required.
Infective conditions
Balanitis
Balanitis is inflammation of the glans penis and may also involve the foreskin (balanoposthitis). It is more common in children. It typically presents with penile soreness, itching and offensive smell or discharge from beneath the foreskin. Erythema of the glans penis, possibly extending to the foreskin, is typically seen. There may also be swelling and difficulty in foreskin retraction.
Balanitis is not always infective. It may be due to poor hygiene which causes irritation by smegma. Smegma is the combination of secretion from sebaceous glands and desquamation of epithelial cells that collects beneath the foreskin. It is uncommon in circumcised men and may be related to foreskin dysfunction. In those with poor hygiene, there is a predisposition to secondary infection. Another non-infective cause is a contact dermatitis in response to substances such as toiletries or condoms.
The most common infective causes of balanitis are Candida albicans and Group B β-haemolytic streptococcus. However, infection with other organisms is also possible, particularly those which cause sexually transmitted infections (including Chlamydia and Gonorrhoea). Therefore, a history of recent infection in a partner should be sought.
Sub-preputial swabs are not essential in routine diagnosis and management, although they may be useful in cases that are particularly severe, resistant to treatment or recurrent. In men with candidal balanitis, the possibility of diabetes should be considered.
Management depends on the likely cause. Patients should be advised to maintain good hygiene, being careful to wash beneath the foreskin. Any potential irritating substances such as soap, lubricants and latex condoms should be avoided. Topical hydrocortisone 1% can be used for up to 14 days to relieve irritation in all cases. In addition
In a non-specific balanitis, when candidal infection is uncertain, a combination cream of hydrocortisone with an imidazole cream (e.g. clotrimazole 1%) can be used In cases where candidal infection is certain, oral fluconazole can be used as an alternative In cases where bacterial infection is suspected, amoxicillin or erythromycin are the most appropriate first-line antibiotics. However, if the sexual history reveals a likely alternative cause, subsequent modification of antibiotic choice may be needed.
In men who have acute balanitis and suspected urethritis, ulceration or lymphadenopathy, referral to a genitourinary medicine clinic is necessary because the chances of a sexually transmitted infection are much greater.
Herpes simplex
Herpes simplex infection is predominantly caused by the herpes simplex type II virus, although the epidemiology of this is changing and an increasing number of cases are now caused by type I. Once infected, attacks tend to be recurrent.
Herpes infection typically starts with prodromal symptoms such as itching and tingling. Subsequently, vesicles develop which progress into an extremely painful ulcer. It is usual for there to be dysuria, tender inguinal lymphadenopathy and systemic upset. The first attack tends to be the most severe and lasts longer than subsequent attacks.
Diagnosis is usually by history and examination. Viral culture is the gold standard but depends on the timing of the swab. If the infection is a suspected first episode, the patient should be referred to the genitourinary medicine clinic for diagnosis, treatment, screening for other sexually transmitted infections and follow-up. Treatment is usually with aciclovir 200 mg five times a day for 5 days, but needs to be commenced within 5 days of the appearance of lesions and while new lesions are still forming. Analgesia, topical 5% lidocaine ointment and saline baths may also be helpful.
Syphilis
Infection with Treponema pallidum is re-emerging in the community. Symptoms appear 9–90 days following exposure. Primary syphilis is the initial presentation. A papule usually appears on the penis which ulcerates to become a painless, hard chancre. Local lymphadenopathy occurs, with nodes which are large but painless, in contrast to herpes simplex infection. Referral to the genitourinary medicine clinic is required for treatment and follow-up. If detected in the primary syphilis stage, cure is relatively easy with a 2 week course of antibiotics, and progression can be prevented.
Genital warts
Genital warts result from infection by one of the many types of human papilloma virus. They are the most common sexually transmitted infection (see Fig. 2). In addition to affecting the penis, they may also be found on the scrotum and anus. Transmission is due to skin-to-skin contact. Many are asymptomatic apart from unpleasant appearance. However, warts may cause pain, itching or bleeding.

Penile warts.
Treatment is usually under the supervision of a genitourinary medicine clinic. First-line treatment is with topical agents such as podophyllin and imiquimod. Other treatments include cryotherapy, trichloroacetic acid which is applied in the clinic or curettage.
Conditions affecting the foreskin
Phimosis
The foreskin typically does not retract before 2 years of age. By 4 years of age, 90% of boys will have a retractable foreskin. A patient has a phimosis if the prepuce is non-retractable after this age. Common symptoms include poor urine flow, ballooning of the foreskin at urination and recurrent balanitis. Phimosis is occasionally primary, due to congenital abnormalities. However, it is more commonly secondary to other conditions which cause scarring, including recurrent balanitis, traumatic foreskin retraction or balanitis xerotica obliterans.
Physiological phimosis rarely requires surgical intervention. Topical steroids may be of use in these cases. In pathological phimosis, spontaneous resolution does not occur. Topical steroids also have a role in those with mild scarring. In patients with more severe scarring who develop complications such as disruption to urine flow, pain and recurrent infections, circumcision is indicated. This tends to occur in older children where chronic infections may cause a fibrous foreskin and the histological changes of balanitis xerotica obliterans.
Paraphimosis
Paraphimosis is inability to reduce a retracted foreskin. It commonly occurs following failure to replace the foreskin following catheterization. There is oedema and pain and as time passes it becomes harder to retract the foreskin. It is a surgical emergency. Manual reduction may be possible following cooling and application of local anaesthetic jelly. However, referral may be required for a dorsal slit and consideration of circumcision, especially if recurrent.
Circumcision
Male circumcision is the most common surgical procedure in the world and has sparked a lot of debate. It may be done for either religious or medical reasons. Neonatal circumcision on the eighth day of life is practised in the Jewish faith and is performed by a mohel. The Muslim faith also carries out circumcision, although the timing is less strict. In England, circumcision is not carried out on the National Health Service (NHS) purely on the grounds of religion. The situation in Scotland is slightly different. Often the GP is not involved in religious circumcision as there are usually people within the community of the faith who typically carry out the procedure. If this is not the case, the GP is able to refer the family to a private clinic. The ideal time for circumcision is thought to be between 6 and 9 months of age.
It is widely considered that circumcision is over-performed in this country. This is often because of premature intervention in boys with a non-retractile foreskin. The one absolute medical indication for circumcision in children is scarring of the opening of the foreskin making it non-retractable (pathological phimosis). This is unusual before 5 years of age. Circumcision in children is also sometimes required for recurrent severe episodes of balanoposthitis.
In adults, circumcision may be required for paraphimosis. Very occasionally it may also be performed in the context of recurrent urinary tract infection, especially if with Proteus spp., and once other causes have been excluded. There are also relative indications for circumcision in adults, including the prevention of penile and cervical cancer, the prevention of sexually transmitted infection including human immunodeficiency virus, and the prevention of urinary tract infection. However, the evidence base for the role of circumcision in these cases is limited and thus a contentious issue.
Complications of circumcision can be drastic. Apart from bleeding and the usual problems related to skin healing, complications include abnormal rotation or chordee of the penis, meatal stenosis, partial or total penile amputation and formation of urethral fistula. Alterations in penile sensation are also well documented.
Congenital conditions
Hypospadias and epispadias
Hypospadias occurs when the urethral meatus is located on the ventral side of the penis, proximal to the site of the normal opening, as illustrated in Fig. 3. Epispadias occurs when the meatus is located on the dorsal aspect of the penis. More proximal hypospadias or epispadias are often associated with other urinary tract abnormalities. As a minimum, these cases should undergo an ultrasound examination of the urinary tract and referred to a paediatric surgeon. Depending on the severity, which is judged by the presence or absence of a socially acceptable urine flow and sexual function, surgery may be required. It is important to note that once a hypospadias has been diagnosed, circumcision should be strongly advised against, in case the foreskin is required for any later reconstruction.
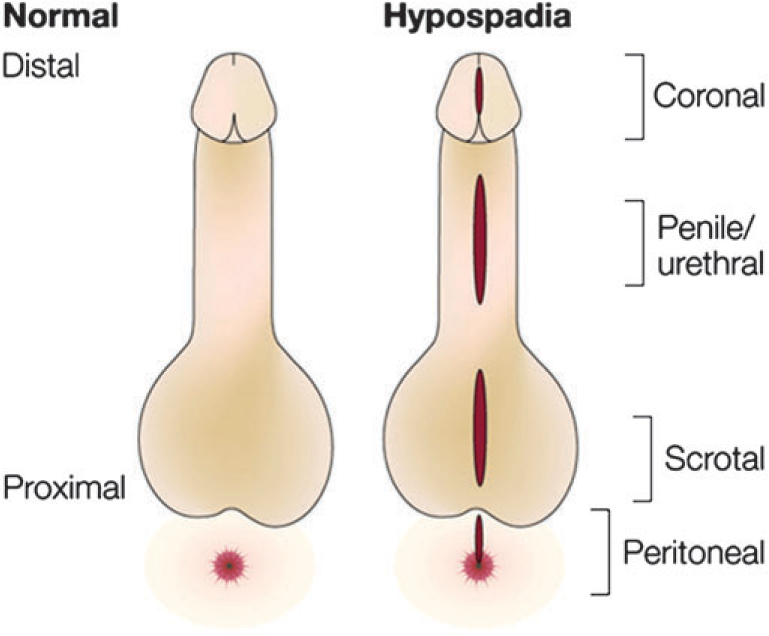
Types of hypospadias.
Acquired conditions
Erectile dysfunction
Erectile dysfunction is an entire topic in itself and outside of the scope of this article. Therefore, only a brief overview is given below.
Causes broadly fall into two categories — psychological and organic. Psychological causes may be mental health issues, anxiety or social issues and will not be discussed any further here. Organic causes are listed in Table 1.
Drug-induced causes of erectile dysfunction

History, examination and investigations seek to establish the cause as this is likely to have considerable impact on the success of any treatment. Correction (where possible) of any organic causes is a prerequisite. Treatments can be oral, injectable, intraurethral, mechanical (the use of vacuum devices) or surgical.
The most commonly prescribed treatments in primary care are oral medications. Phosphodiesterase inhibitors such as sildenafil and tadalafil are usually considered first line. There are some important circumstances in which they are contraindicated though. Nitrates interact with phosphodiesterase inhibitors to cause severe hypotension. Other contraindications include hypotension (blood pressure below 90/50 mmHg), severe hepatic impairment, recent stroke or myocardial infarction or hereditary degenerative retinitis pigmentosa. Other interventions are usually initiated by specialist clinics.
Not all patients are eligible for drug treatment for erectile dysfunction on the NHS. Box 1 lists those who are eligible. Others, unfortunately, have to be issued with private prescriptions for any medication prescribed.
Eligible groups for NHS treatment of erectile dysfunction
Diabetes Multiple sclerosis Parkinson's disease Poliomyelitis Prostate cancer Prostatectomy — includes transurethral resection of the prostate Radical pelvic surgery Renal failure treated by dialysis or transplant Severe pelvic injury Single-gene neurological disease Spinal cord injury Spina bifida
The Department of Health (England) has recommended that treatment should also be available from specialist services (commissioned by Health Authorities and Primary Care Trusts and operating under local agreement) when the condition is causing severe distress.
In all cases, NHS prescriptions for patients eligible for treatment should be endorsed ‘SLS’.
Priapism
Priapism is defined as the presence of a persistent painful erection lasting for longer than 6 hours, outside of the context of sexual drive. It is always pathological. It may be as a consequence of treatment for erectile dysfunction, haematological conditions such as leukaemia or sickle cell disease, trauma to the spinal cord or penis or due to a pelvic tumour. If caught early, conservative treatment is likely to be successful. This works by reducing the amount of blood in the penis. Exercise (such as running up and downstairs) can redirect blood flow away from the penis, and ice packs can cause vasoconstriction. On presentation in primary care, emergency urological referral is indicated, even if not persisting for 6 hours. Drainage of the corpora cavernosa may be required.
Penile fracture
Penile fracture is uncommon but frequently misdiagnosed. It is traumatic rupture of the corpus cavernosum. One or both may be affected, and there may also be damage to the urethra. It typically occurs with the penis in an erect state. Often it arises as a sexual injury or from bending the penis down to void with an early morning erection. It can also occur with a shearing force.
At the time of injury a ‘crack’ is usually heard. This may be painless, although if there is severe injury, pain can be intense. There is immediate loss of erection with failure to regain it. Over subsequent hours, the blood seeps into the surrounding tissues. In a typical penile fracture, the normal external penile appearance is completely obliterated because of significant penile deformity, swelling and ecchymosis (the so-called ‘eggplant’ or ‘aubergine’ deformity).
On examination, there is usually significant soft tissue swelling of the penile skin, penile bruising and haematoma formation. The penis tends to assume an S-shape deformity. Blood may be seen at the meatus if there is damage to the urethra. If the presentation is atypical with minimal bruising and a straight penis, the defect in the tunica is often palpable. It is usually very tender. This is a surgical emergency and needs to be referred immediately.
Other traumatic penile injuries include penile amputation, penetrating penile injuries and penile soft tissue injuries. These all typically require urological surgical input and thus also need immediate referral. They are usually identified based on history. In all these cases, the aim of treatment is to preserve penis morphology and length, maintain erectile function and to enable the individual to continue voiding while standing.
Malignant conditions
Penile intraepithelial neoplasia
Penile intraepithelial neoplasia is an uncommon premalignant condition affecting the epidermis of the penis. It is also known as Bowen's disease of the penis or squamous cell carcinoma in situ. It is almost always found in uncircumcised men. It is usually located on the inner aspect of the prepuce or on the glans penis and at these sites, red plaques are found, as seen in Fig. 4. The texture of the surface is variable. There may be redness, inflammation, itching, crusting, scaling, pain, ulceration, bleeding or symptoms related to phimosis.

Penile intraepithelial neoplasia.
If penile intraepithelial neoplasia is suspected, the patient should be referred for biopsy as it can easily be confused with other causes of chronic balanitis. Management is by a specialist team and there are several different options, including topical treatment, curettage, cryotherapy and radiotherapy. If left untreated, up to a third of cases develop into squamous cell carcinoma.
Penile cancer
Penile cancer is almost always a squamous cell carcinoma, as illustrated in Fig. 5. It develops between the glans penis and the foreskin. It may be a development of a penile carcinoma in situ or leucoplakia. Metastasis is rare, although local lymph node involvement is common. Local spread often involves the distal urethra causing difficulties with micturition, but urinary retention as a consequence is rare. Although it has not been proved that circumcision is preventive, penile cancer is considerably less common in those who have been circumcised. Risk factors include human papilloma virus infection, poor hygiene and genital herpes. It is most common in older patients and may present as ulceration or a papillary growth. There may also be an offensive or bloodstained discharge. Penile cancer may be hard to distinguish from chronic balanitis. If you suspect that a patient might have penile cancer, refer urgently for a biopsy. If confirmed, treatment is either by radiotherapy or surgery. The 5 year survival rate is good and up to 80% in those cases without inguinal node involvement.

Penile squamous cell cancer.
Key points
Due to the sensitive nature of penile conditions, the doctor needs to be confident in their knowledge and mindful of the possibility of the patient's embarrassment Skin conditions can affect the penis just like anywhere else on the body, although the appearance may vary slightly The suspicion of sexually transmitted infections should prompt referral to a genitourinary medicine clinic for further screening and monitoring of treatment Circumcision is frequently over-performed in this country and time should be used as a tool to aid the decision as to whether it is actually necessary Persistent skin conditions and ulceration should provoke consideration of penile malignancy and skin biopsy should be performed to confirm the diagnosis