
Abstract
Stable angina is a common presentation in primary care. It is a symptom indicative of myocardial ischaemia rather than a disease itself. Two million people in the UK suffer from angina, and coronary heart disease accounts for around one in six deaths in the UK. Therefore, it is of pivotal importance that doctors should be informed about the symptoms of angina and their management.
The GP curriculum and stable angina
have a good knowledge of the presenting features and management of coronary heart disease (CHD), including stable angina and acute coronary syndromes be able to elicit appropriate signs and symptoms and order the necessary investigations and/or referrals for people presenting with chest pain
form a reasoned approach to the diagnosis of cardiovascular symptoms such as chest pain demonstrate an understanding of the importance of risk factors in the diagnosis and management of cardiovascular problems intervene urgently when patients present with a cardiovascular emergency, for example unstable angina
Pathology
Angina pain results from inadequate blood supply to meet the oxygen demands of the myocardium and thus myocardial ischaemia. This may be as a result of restricted blood flow to the myocardium, increased oxygen demand from the myocardium or a combination of the two. Coronary artery disease is the most common cause. This may take the form of stenotic atheromatous disease of the coronary arteries, thrombosis within the coronary arteries (Fig. 1) or coronary artery spasm (Prinzmetal angina). Rarer causes include hypertension, valve disease (particularly aortic stenosis), hypoperfusion during arrhythmia, hypertrophic obstructive cardiomyopathy, arteritis or conditions that require increased cardiac output such as anaemia or thyrotoxicosis.
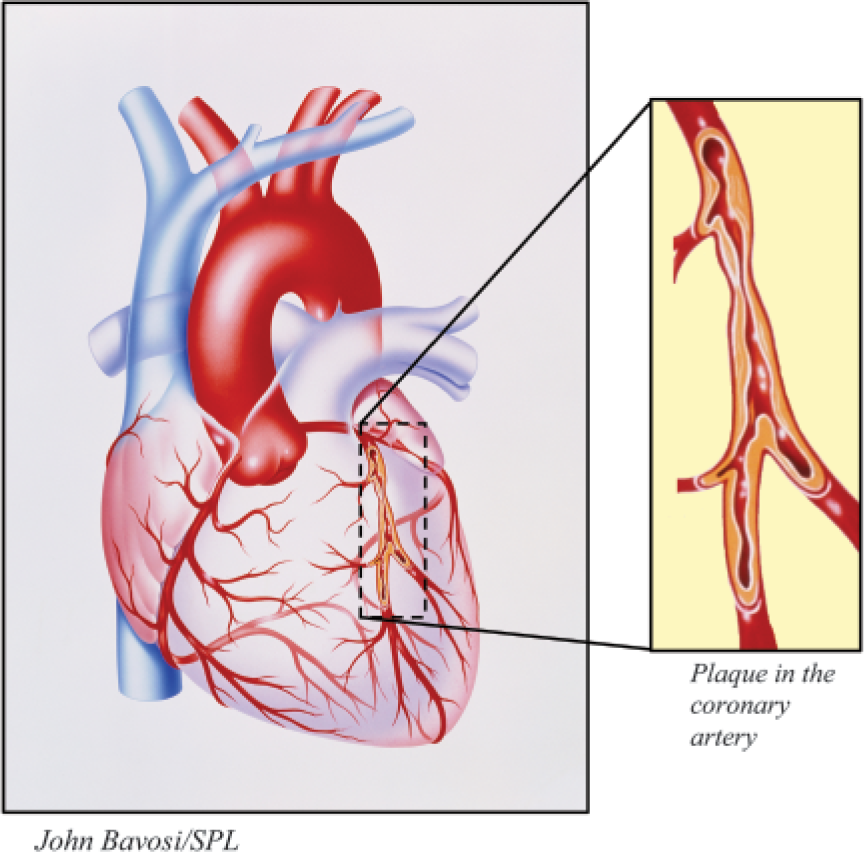
Atherosclerotic plaque in a coronary artery causing narrowing, reduced blood flow and angina.
Epidemiology and risk factors for angina
It is estimated that about 2% of the British population is at any time affected by ongoing or recent symptoms of angina (Joint Health Surveys Unit, 2008). There is a higher incidence of angina in men than in women and a gradual increase in prevalence with age. Table 1 summarizes modifiable and non-modifiable risk factors for angina. In patients with angina, risk of death is between 0.5 and 4% per year. This figure is doubled when the patient has coexistent left ventricular dysfunction. Death may be sudden or occur after myocardial infarction or acute left ventricular failure.
Risk factors for angina

Presentation of stable angina
When assessing a patient in the GP surgery with possible angina, use your history, examination and investigation to confirm features that are compatible with a diagnosis of angina and exclude features that might suggest an alternative cause of chest pain (Box 1).
History
Diagnosis of angina is usually made based on a history of chest pain. Presence of risk factors such as smoking, family history, diabetes or personal history of other forms of cardiovascular disease increases the likelihood that chest pain is caused by myocardial ischaemia.
Typically, patients present with episodic central-crushing, or band-like, chest pain. The pain may radiate to the jaw or neck and/or to one or both arms. However, pain in the arms or neck may be the only symptom, and the description of the chest pain may be atypical. Ask about frequency, severity, duration and timing.
Typically, angina pain is precipitated by exertion, cold, emotion and/or heavy meals. Pain is relieved by rest or use of a glyceryl trinitrate (GTN) spray. Relief of pain by antacids suggests an oesophageal cause of pain but does not exclude angina. Sometimes, there may be other associated symptoms, such as palpitations, sweating, nausea or breathlessness during attacks.
Differential diagnosis of stable angina
Acute myocardial infarction or unstable angina Other cardiac causes of pain—Prinzmetal angina and pericarditis Gastro-intestinal disease—oesophageal spam, gastro-oesophageal reflux and gallstone disease Pulmonary disease—pleurisy, pneumothorax and pulmonary embolus Musculoskeletal pain—costochondritis, rib pain, radiculopathy, shingles and muscular injury (e.g. as a result of coughing)
Examination
There are usually no physical signs of angina, although anaemia may exacerbate symptoms. Check body mass index and blood pressure as these are modifiable risk factors for both primary and secondary prevention of CHD. Look for murmurs (especially ejection systolic murmur of aortic stenosis), evidence of peripheral vascular disease and carotid bruits. Examine the chest and abdomen to exclude other possible causes of chest pain (Box 1).
Primary care first-line investigations
Investigations in primary care are aimed at identification of possible causes of angina, stratification of risk and establishment of a diagnosis of angina. Baseline blood tests include a full blood count to exclude anaemia, a fasting lipid profile to identify patients with hyperlipidaemia and gain a baseline measurement of serum lipids for secondary prevention purposes and a fasting blood glucose to exclude diabetes. In addition, consider checking an erythrocyte sedimentation rate or C-reactive protein to exclude arteritis and thyroid function tests if there is any clinical suspicion of thyrotoxicosis. Consider checking renal and liver function at the same time as the results of both these tests will be required should drug treatment be started.
A 12-lead resting electrocardiogram (ECG) provides information on rhythm, presence of heart block, previous myocardial infarction, myocardial hypertrophy and myocardial ischaemia. The most familiar ECG patterns of ischaemia are horizontal or downsloping ST segment depression of 1 mm or more (Fig. 2) and T-wave flattening or inversion (Fig. 3a). These signs of ischaemia can be isolated to ECG leads overlying the involved myocardium and suggesting localized ischaemia or they can be present in many ECG leads, suggesting more widespread ischaemia. Other less commonly seen signs of ischaemia include wide-based tall T waves (Fig. 3b) and U-wave inversion (Fig. 3c).
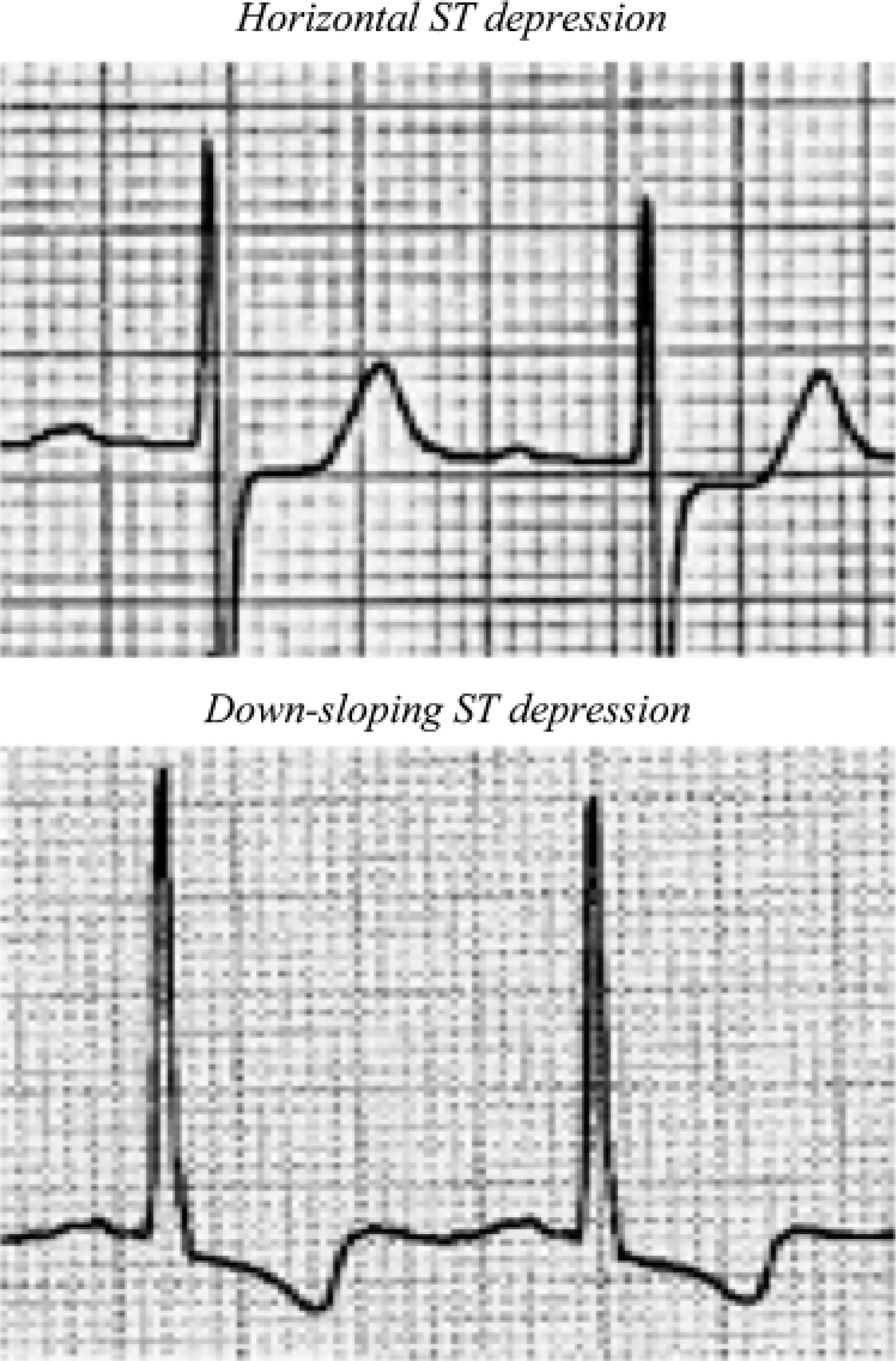
ST depression indicating myocardial ischaemia.
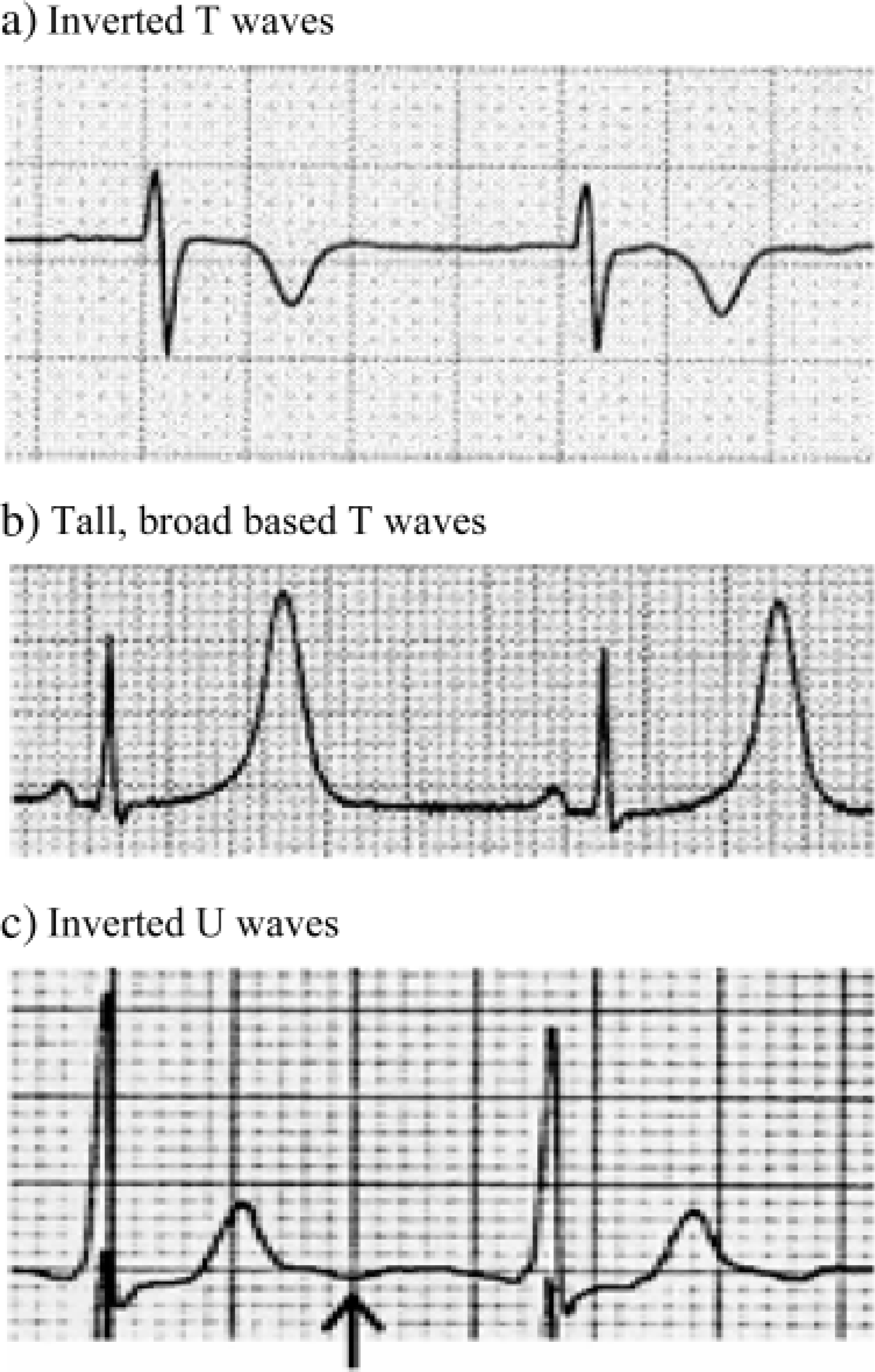
Other electrocardiogram changes that may indicate myocardial ischaemia: (
It is important to remember that a normal ECG does not exclude coronary artery disease but an abnormal ECG identifies those at higher risk of cardiac events in the next year. In addition, consider a chest X-ray to exclude ventricular enlargement, pulmonary changes of left ventricular failure and other lung disease that may cause chest pain.
Referral of patients with suspected stable angina
Consider emergency admission for any patient with symptoms of unstable angina. These are ischaemic chest pain on minimal or no exertion (e.g. at night when in bed) or angina that is rapidly worsening in intensity, frequency or duration.
For patients with new-onset intermittent chest pains, referral to a rapid-access chest pain clinic is usually the best option. These clinics have been developed to allow quick assessment of patients with new-onset suspected angina to meet the target of specialist assessment within 2 weeks specified in the National Service Framework for Coronary Heart Disease. The format of these clinics does vary slightly from area to area as do referral criteria, but they all provide
prompt specialist assessment to confirm or refute angina as a cause of symptoms estimates of cardiac risk information on treatment options available information regarding modifiable risk factors assessment of the merits of revascularization for the individual patient and referral for further investigations and intervention as appropriate initiation of treatment to relieve symptoms and reduce risk reassurance to patients who do not have significant coronary artery disease
Rapid-access chest pain clinic referral criteria usually exclude those with pre-existing known CHD, such as those who have suffered a myocardial infarction and develop angina afterwards, or those with pre-existing angina who experience a worsening of their symptoms. They may also exclude patients with other cardiac disease such as known valve disease or cardiomyopathy. These patients should be referred for outpatient specialist review. The degree of urgency depends on the symptoms they are experiencing. Quality and Outcomes Framework (QOF) points are available for referral of patients with newly diagnosed angina for exercise testing and/or specialist assessment.
Specialist investigations
Exercise tolerance testing
Unless contraindicated, all patients with angina require an exercise tolerance or stress test to allow risk stratification. In most areas, this is arranged by the rapid-access chest pain clinic. Contraindications to stress testing are listed in Box 2. Advise patients to take their usual medication before going for the test unless instructed otherwise by their cardiologist.
Contraindications to exercise testing
Symptoms uncontrolled by maximal medical treatment Proven or suspected aortic stenosis or cardiomyopathy Physically incapable of performing the test for reasons other than angina Results of stress testing would not affect management Left bundle branch block on ECG
Coronary angiography
Coronary angiography involves passing a catheter, usually through the femoral or brachial artery, to the heart. Contrast is injected into the coronary arteries to assess their anatomy and patency. Angioplasty and stenting are sometimes performed at the same time as angiography. The most common complications of coronary angiography are haemorrhage at the site of insertion (0.56%) and arrhythmia (0.56%). Other complications include myocardial infarction (0.07%), stroke (0.07%), thromboembolism, trauma to the heart or heart vessels and death (0.14%).
Radionucleotide imaging
Radionucleotide imaging involves intravenous administration of a gamma-emitting radionucleotide and gamma camera monitoring. Radionucleotide angiography uses 99mTc-labelled red blood cells to calculate left ventricular ejection fraction and assess ventricular action. Myocardial perfusion scintigraphy uses thallium201, injected intravenously during exercise testing to demonstrate areas of poorly perfused myocardium.
Cardiac magnetic resonance imaging
Cardiac magnetic resonance imaging and magnetic resonance angiography are being used increasingly to provide detailed structural information about the heart and rapid angiographic images.
Management of stable angina in primary care
All patients with angina should be on the practice CHD register to ensure regular follow-up, at least on an annual basis. QOF points are available for keeping a register of patients with CHD and reaching management targets for patients with angina (Table 2). All patients with angina should be offered annual influenza vaccination and a once-only pneumococcal vaccination.
Quality and Outcomes Framework points for patients with CHD (2009/10)
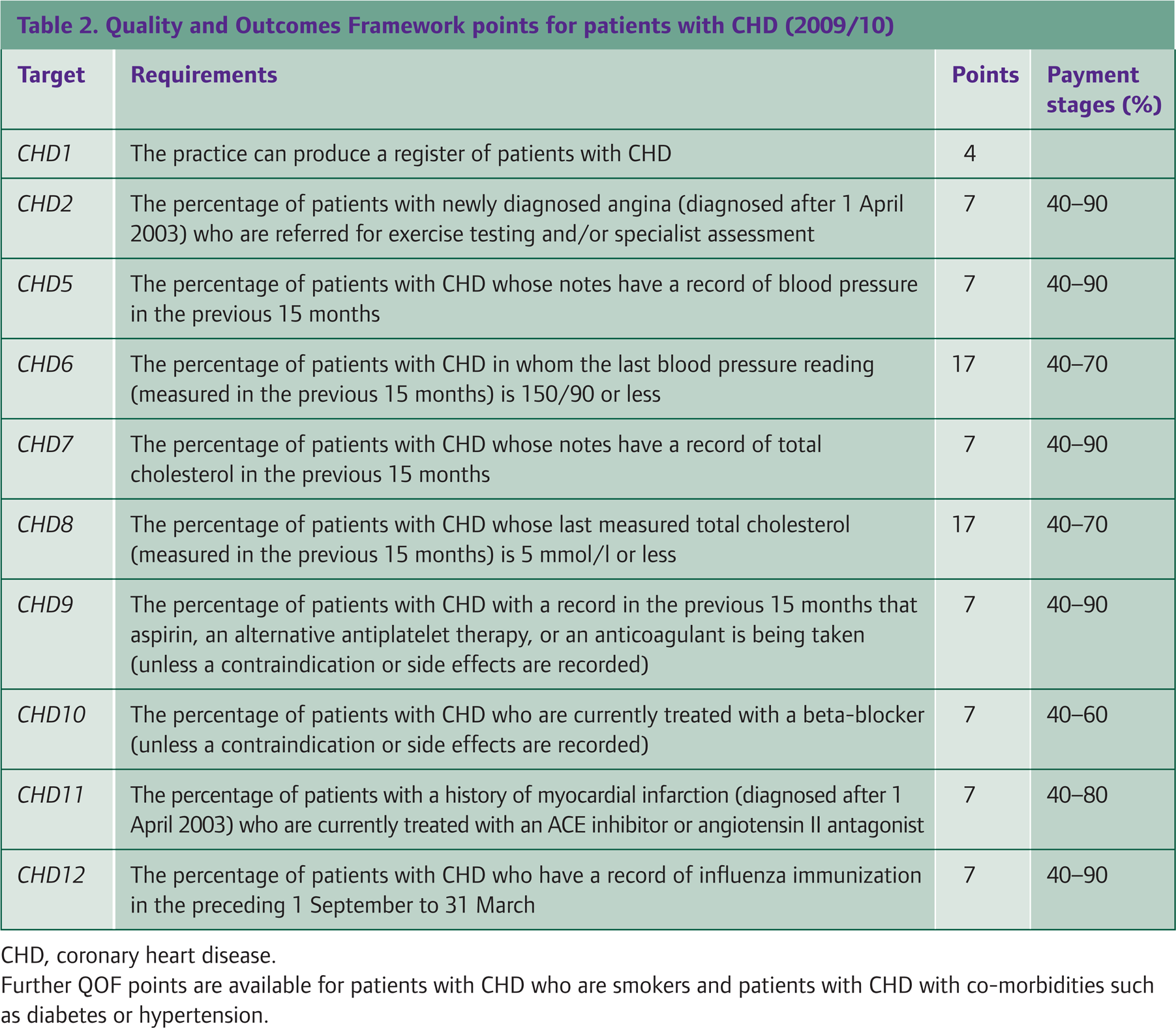
CHD, coronary heart disease.
Further QOF points are available for patients with CHD who are smokers and patients with CHD with co-morbidities such as diabetes or hypertension.
Advice about driving
Patients who drive should inform the Driver and Vehicle Licensing Agency and their insurance company of the diagnosis of angina. Advise patients with angina to stop driving if they have an attack while at the wheel, at rest or with emotion until symptoms are controlled. For vocational drivers, their licence is revoked until they have been symptom free for more than 6 weeks. Renewal of a vocational driving licence requires medical examination and exercise ECG.
Advice about work and benefits
Patients suffering from angina may not be able to undertake heavy work. It is important to give advice and support patients unable to perform their usual work as a result of angina. In addition, special rules for people with a diagnosis of angina apply for some occupations. For example, merchant seamen or airline pilots cannot usually work if they have angina. If patients are unable to perform normal work duties, advise them to contact their occupational health department. Employers must make reasonable adjustment under Disability Discrimination legislation, but this is a complex field, and independent advice from the Citizens Advice Bureau, a trade union or the Arbitration and Conciliation Advisory Service is advised.
Patients of working age with symptoms of angina that restrict their ability to work may be eligible for Statutory Sick Pay and/or Employment and Support Allowance. Patients disabled as a result of angina who have difficulties with everyday activities may also qualify for Disability Living Allowance (less than 65 years) or Attendance Allowance (65 years of age or older). Further information is available on website www.direct.gov.uk/disability.
Advice about sexual intercourse
For patients at high risk of a cardiovascular event, undertaking sexual activity may constitute a significant risk. Advise patients with unstable or severe angina to refrain from sexual intercourse. For patients with mild-to moderate-intensity stable angina, unless advised otherwise by a cardiologist, sexual intercourse is safe. However, it may be wise to advise patients to abstain from intercourse if the patient has
New-onset chest pain where a specialist has not yet confirmed the diagnosis of angina Exercise testing has suggested angina but further evaluation (e.g. with coronary angiography) is awaited
Non-drug treatment
Non-drug treatment of angina is aimed at secondary prevention of CHD. Therefore, it is important to offer lifestyle advice to reduce CHD risk to all patients with angina. A multifactorial approach that addresses all risk factors is of most benefit as the effect of modifying several risk factors is multiplicative. The major points to cover are listed in Box 3. Reinforce your advice with written information. In addition, cardiac rehabilitation may be helpful for patients with severe angina and/or after surgery.
Lifestyle advice for patients with angina
Smoking cessation Hypertension—check blood pressure and treat if it is greater than 140/90 mmHg Diet — advise healthy diet: oily fish, low cholesterol, increase in fruit and vegetables (five portions a day) and reduce salt. If the patient is obese, aim to reduce weight until body mass index is less than 25 kg/m2. Alcohol—reduce excess consumption. Targets: less than 3 units per day for men and less than 2 units per day for women. Exercise—increase aerobic exercise within the limits set by the disease state Diabetes—treat any underlying diabetes
QOF points are available for identifying patients with CHD who are smokers. Further points are available for providing smoking cessation advice or referral to a smoking cessation service.
Drugs for symptom control
Drugs to control angina symptoms may be given as required or regularly. GTN spray is used for ‘as required’ symptom relief for angina. Advise patients to take one to two puffs under the tongue as needed in response to pain and before engaging in activities that bring on the pain. Sublingual GTN tablets are an alternative to GTN spray but deteriorate after 8 weeks and then need replacement. A common side effect in both cases is headache. Always warn patients to call for help (dial for an emergency ambulance or ring the emergency GP) if their angina chest pain lasts for more than 20 minutes despite GTN spray.
Drugs used for regular symptom control for patients with angina are summarized in Table 3. Guidance within the QOF (2009) suggests that all patients with angina should be taking a beta-blocker (such as atenolol 50–100 mg daily) unless contraindicated or not tolerated. Points are available within the QOF for prescribing beta-blockers for patients with angina. Although the trial evidence of reduced mortality and morbidity in patients taking beta-blockers relates mainly to patients who have had a myocardial infarction, the evidence has been extrapolated to all patients with CHD. Consider a highly selective agent if the patient has asthma, chronic obstructive pulmonary disease or left ventricular dysfunction.
Drugs for symptomatic treatment of angina

Add further medication in a stepwise manner according to symptom control:
Step 2: If symptoms are not controlled with a beta-blocker, or beta-blockers are contraindicated or not tolerated, add a long-acting dihydropyridine calcium channel blocker (e.g. amlodipine 5 mg daily). Avoid combination of beta-blockers and rate-limiting calcium channel blockers (such as verapamil or diltiazem) due to the risk of bradycardia and asystole.
Step 3: There is little evidence to support combination therapy with three agents. If treatment with a beta-blocker and calcium channel blocker is ineffective, consider adding a long-acting nitrate or nicorandil and/or re-referral for further specialist assessment.
Drugs for secondary prevention
It is important to note that cardiac risk scores to not apply to patients with angina. All patients with proven angina are at high risk of cardiovascular events and require preventive drug treatment.
Aspirin reduces mortality in patients with angina by 34%. Unless contraindicated, give 75 mg daily to all patients with angina. Consider prescribing clopidogrel (75 mg daily) if the patient is aspirin intolerant.
Reduction in total cholesterol and low-density lipoprotein (LDL) cholesterol by 25–35% using statin therapy results in a 25–35% drop in CHD mortality in patients with angina. Trial data suggest that all patients with proven CHD benefit from reduction in total cholesterol and LDL irrespective of their initial cholesterol levels. Simvastatin is the first choice agent (NICE CG67, 2008). Although the QOF sets an audit standard of total cholesterol of less than 5 mmol/l for QOF points to be awarded, aim
to reduce total cholesterol by 25% or to less than 4 mmol/l (whichever is the lower value) and to reduce LDL cholesterol by 30% or to less than 2.0 mmol/l (whichever is the lower value)
Measure serum lipids 3 months after starting treatment or 4–6 weeks after any dose change. If the cholesterol level is stable and within target range, thereafter measure serum lipids 6–12 monthly. Consider increasing simvastatin to 80 mg daily if target lipid levels are not met.
It is important to control hypertension in all patients with angina and monitor blood pressure regularly (at least annually). A reduction of 5–6 mmHg in blood pressure sustained over 5 years reduces coronary events by 20–25% in patients with angina. The QOF sets an audit standard of 150/90 mmHg for QOF points to be awarded, but NICE CG34 (2006) recommends a target of 140/85 mmHg for patients with CHD.
In addition to their role in reducing blood pressure, angiotensin-converting enzyme (ACE) inhibitors significantly reduce cardiovascular deaths (relative risk 0.83) and all-cause mortality (relative risk 0.87) in patients with angina, even in the absence of left ventricular dysfunction. Start all patients on a low dose of an ACE inhibitor, such as ramipril, and titrate the dose upwards to the maximum dose tolerated.
Referral for further cardiology assessment
Further assessment by a specialist cardiologist is recommended if
The patient has unstable angina or rapidly progressive symptoms (admit as an emergency) The angina is not controlled by medication (speed of referral will be determined by frequency and severity of symptoms) If diagnosis is in doubt There are any other factors that warrant a specialist opinion, for example if occupation is affected
Revascularization
In some patients, revascularization procedures may be indicated. Decision to refer for a revascularization procedure must be made by a consultant cardiologist and is based on symptoms, investigation findings and response to medical treatment. There are two major types of revascularization interventions, open bypass surgery or coronary artery bypass grafting (CABG), and percutaneous interventions. Percutaneous interventions include balloon angioplasty and coronary artery stenting. Choice of intervention depends on the nature and extent of the coronary artery lesions.
CABG has been shown to reduce CHD mortality over 5, 7 and 10 years by up to 16%. It also reduces symptoms of angina in 80–90% of those who underwent the operation. However, CABG is a major surgical procedure involving general anaesthesia, sternotomy and then bypass of the blocked or stenosed coronary arteries using venous grafts from the leg veins or arterial grafts from the intercostal arteries. The operation itself carries a mortality rate of 1–4%.
Balloon angioplasty is an angiographic procedure in which a tightly folded balloon is passed along a guide wire through a narrowing in the coronary artery. The balloon is then inflated with water, stretching open the artery and thus increasing blood flow through it. Simple balloon angioplasty improves symptoms for 70% of those undergoing the procedure, although evidence of a reduction in mortality is lacking. However, when performed in isolation, a small number of patients experience coronary artery collapse within hours of the procedure requiring emergency CABG. Furthermore, with time, about 30% of stents restenose requiring a repeat procedure or CABG at a later date.
Drug-eluting stents (also known as coated or medicated stents) are metal stents that can be placed within the coronary artery following balloon angioplasty to hold it open. The metal stent is coated with a pharmacologic agent (the ‘drug’) that is known to interfere with the process of restenosis. Patients who have a drug-eluting stent are also required to take clopidogrel (75 mg daily) in addition to their aspirin for a year after the procedure to reduce the risk of restenosis. Like simple angioplasty, angioplasty with coronary artery stenting improves symptom control by about 70% but abolishes the problem of coronary artery collapse early after the procedure. Using a drug-eluting rather than bare metal stent, the restenosis rate is significantly reduced to about 5%.
Prinzmetal (variant) angina
Prinzmetal angina is angina that occurs at rest due to coronary artery spasm. ECG shows ST elevation. In the surgery, it is impossible to tell Prinzmetal angina apart from ischaemic CHD. GTN alleviates immediate episodes. Therefore, it is important to refer to cardiology to exclude atherosclerotic angina. Calcium channel blockers are used to prevent symptoms.
Cardiac syndrome X
Cardiac syndrome X is the term that describes patients who experience symptoms of stable angina, mainly triggered by emotional responses rather than exercise or other physical stressors. These patients have a positive exercise ECG (ST depression only); however, the coronary arteries are normal when coronary angiography is performed. As yet, the cause of this condition is not clear, but possible causes include coronary artery spasm and microvascular abnormalities.
Key points
Angina is a common condition affecting about 2% of the British population at any time Presence of angina usually indicates myocardial ischaemia, most commonly as a result of coronary atherosclerosis Diagnosis in primary care is made on the basis of history of chest pain Patients with new suspected angina should be referred for specialist assessment through a rapid-access chest pain clinic Treatment involves lifestyle advice, drugs for symptom control, drugs for secondary prevention of atherosclerotic disease and, in some cases, revascularization