
Abstract
‘Problem drinking’ is a major national concern as it can lead to long-term serious physical and mental health problems. Alcohol can mimic or accentuate many of the symptoms of depression: low mood, low energy, changes in appetite, weight or sleep pattern, poor concentration, feelings of guilt or worthlessness and suicidal ideation. Many people with depression can develop an alcohol problem as they may ‘self-medicate’ to feel more energetic or cheerful. In severe cases, alcohol misuse can lead to impaired judgement and increase the risk of suicide. Patients with severe depression and alcohol dependence coexisting are considered to have a ‘dual diagnosis’ and often require support from mental health specialist services such as community alcohol team in addition to primary care support.
The GP curriculum and alcohol and depression
Familiar with ways of identifying excess alcohol consumption Aware of the morbidity (physical, psychological and social) caused by alcohol Aware that they can have a major impact in reducing alcohol consumption in their patients by a simple technique called brief intervention
Manage people experiencing mental health problems in primary care, bearing in mind that several interventions may be effective for each mental health condition, including different forms of talking therapy, medication and self-help Describe specific interventions and guidelines for individual conditions such as depression using best practice as described in the National Institute for Health and Clinical Excellence (NICE) guidelines Demonstrate how to screen, and diagnose, people experiencing mental health problems using effective and reliable instruments where they are available Describe how to access health and social care organizations, both voluntary and statutory, that are an essential component of managing people with mental health problems Describe when it is appropriate to refer to and collaborate with the specialist mental health services
This article describes the key features of alcohol misuse and depression to help GPs recognize these conditions and provide a management plan to support these patients in the primary care setting. As a GP, one should be able to screen patients for alcohol misuse and depressive symptoms, diagnose, assess severity, educate and manage patients appropriately while encouraging patient autonomy and self-help strategies. It is essential that GPs can identify those at risk of suicide and know when to refer to mental health specialist services.
Epidemiology
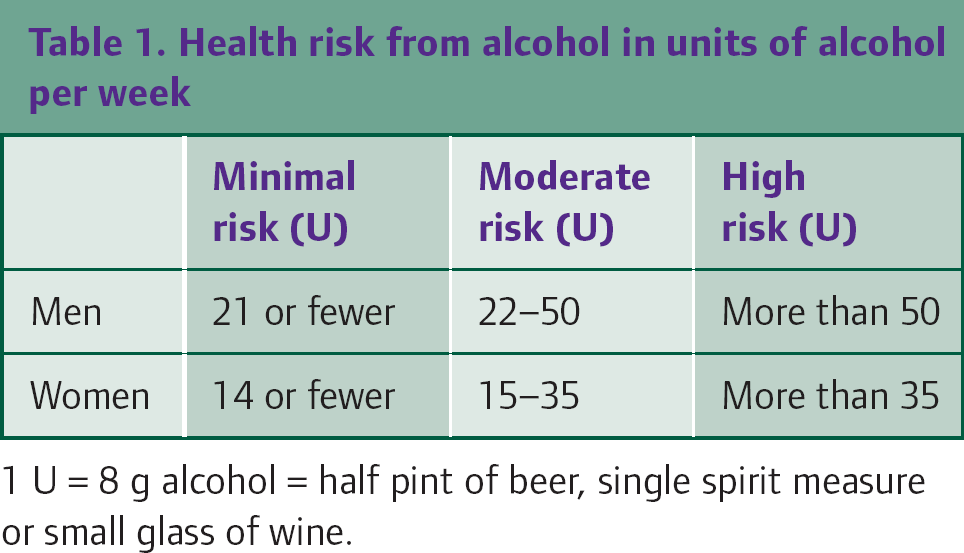
Thirty-four percent of men and 20% of women in the UK exceed the recommended number of weekly units for sensible drinking (Table 1). One in 15 men and one in 50 women suffer from alcohol dependence, and 40% of dependents have symptoms that resemble a depressive illness. However, when these same patients drink within normal limits, only 5% of men and 10% of women have symptoms meeting the diagnostic criteria for depression—not that different from the rates of depression in the general population. Conversely, about 5–10% of people with a depressive illness have symptoms of an alcohol problem.
Health risk from alcohol in units of alcohol per week
Cause or effect?
It has been well established that excess alcohol consumption increases the risk of developing depression. Self-harm and suicide are more common in patients with alcohol problems. Alcohol feeds depressive symptoms increasing both their frequency and severity. Furthermore, depressed patients may turn to alcohol to ‘drown their sorrows’ and thus are at increased risk of developing an addiction.
Alcohol is a central nervous system depressant; however, patients mistakenly believe that alcohol has the ability to ease symptoms as it has a short-term euphoric effect. Hangovers can create a cycle of waking up feeling ill, anxious, jittery and guilty. Alcohol can also lead to social disruption such as arguments with friends or family, trouble at work, memory and sexual problems, thus mimicking or aggravating coexisting depressive symptoms.
Alcohol has a disruptive effect on circadian rhythms and heavy consumption of alcohol has a detrimental effect on the second half of the sleep cycle. In addition to bringing about fitful dreams, consuming alcohol before retiring may prevent the onset of rapid eye movement (REM) sleep. This destabilizes levels of serotonin and dopamine in the brain, which, in turn, can precipitate a depressive disorder.
Alcohol
‘Harmful drinking’ is defined as a pattern of drinking that causes damage to physical health (e.g. liver disease) or mental health (such as depression secondary to heavy consumption of alcohol). ‘Hazardous drinking’ is defined as the regular consumption of over 40 g of pure ethanol (5 U) per day for men and over 24 g of pure ethanol (3 U) for women. ‘Binge drinking’ is defined as consumption of more than 8 U of alcohol for men and 6 U of alcohol for women on one occasion.
A person with alcohol dependence has a strong desire to drink alcohol, has difficulty controlling use, persistently consumes alcohol despite knowing its harmful effects, shows increased tolerance for alcohol and shows signs of withdrawal when without alcohol. Consuming over 40 g/day of pure ethanol doubles a man's risk for liver disease, hypertension, some cancers and violent death. For women, consumption of over 24 g/day of pure ethanol increases risks of liver disease and breast cancer.
Box 1 summarizes the physical, psychiatric and social associations of excess alcohol consumption that may present to the GP. Be suspicious of alcohol as a cause of ‘blackouts’, accidents, obesity, pancreatitis, dyspepsia, impotence, anxiety or panic, insomnia, poor employment record or a criminal record. Be aware of risk factors such as employment in the licensing trade, family history of alcohol problems or social isolation.
Screening
There are two well validated questionnaires that GPs can use to screen and assess severity of alcohol misuse: The CAGE questionnaire (Box 2) screens for an alcohol problem and if positive, the Alcohol Use Disorders Identification Test (AUDIT) devised by the World Health Organization can be used to assess whether the patient is a hazardous drinker or has alcohol dependence (Box 3).
Manifestation of alcohol problems

Patients may feel ashamed and not want to admit how much they drink. Under-reporting is quite common, so reassure the patient and use a non-judgemental relaxed approach.
When taking an alcohol history, use non-confrontational questions to begin the discussion. Establish the quantity consumed, time of day of the first alcoholic drink and drinking pattern. The GP can assess whether there are withdrawal symptoms by asking if the patient has experienced any of the following:
Morning shakes, nausea or retching (within few hours of not having a drink and lasting beyond 48 hours) Hyperactivity Anxiety and a coarse peripheral tremor Mild pyrexia and sweating Tachycardia and hypertension ‘Blackouts’, seizures, auditory and visual hallucinations Delirium tremens
CAGE screening tool for harmful drinking—needs permission
Have you ever felt you should Have people Have you ever felt bad or Have you ever had a drink first thing in the morning to steady your nerves or to get rid of a hangover? (
If the patient gives two ‘yes’ responses, the screening test is POSITIVE and the AUDIT tool
Severity
Once problem drinking or alcohol dependence has been identified, ask the patient to keep a diary for the following week to confirm the amount drunk. Examine for the smell of alcohol, tremor, sweating, slurring of speech, hypertension and signs of chronic liver disease:
Jaundice Excoriation marks secondary to pruritus Spider angiomata/naevi (mainly found on trunk and face) Skin telangiectasias (called ‘paper money skin’) Palmar erythema Bruising Petechiae or purpura Hair loss White nails (horizontal white bands or a proximal white nail plate: sign of hypoalbuminaemia) Finger clubbing Dupuytren's contracture Hepatomegaly and a nodular liver Oedema Gynaecomastia and loss of male hair pattern Hypogonadism, testicular atrophy or amenorrhoea Evidence of type 2 diabetes Signs of portal hypertension include: Ascites (can be detected clinically when at least 1.5 l of fluid is present) Caput medusae (veins seen radiating from the umbilicus) Enlarged spleen
Blood tests are useful to assess the extent of alcohol-related disease and to detect cases where there is reason to believe that the patient is under-reporting. Request the following:
Full blood count—looking for macrocytosis Liver function tests (LFTs), including gamma glutamyl transpeptidase (GGT) levels Fasting lipid profile Fasting serum glucose
As well as being raised in patients who consume too much alcohol, the mean cell volume (MCV) can also be raised in people with vitamin B12 deficiency, folic acid deficiency, thyroid disease, chronic liver disease and during pregnancy. GGT is raised in only one-third of those with an alcohol problem, and an elevated level is not specific for misuse. However, a raised MCV together with a raised GGT detects 75% of problem drinkers.
Chronic alcohol consumption is also associated with dyslipidaemia, notably hypertriglyceridaemia and chronic pancreatitis, which can lead to diabetes. Deranged LFTs warrant an ultrasound scan to detect fatty liver, cirrhosis and even liver cancer. Severely disordered liver function may require a referral to a liver unit. For patients with alcohol dependence, an upper gastro-intestinal endoscopy may be useful to detect oesophageal varices.
Management
Patients with an alcohol problem and depressive symptoms should be treated for the alcohol problem first. There is good evidence that a high proportion of depression resolves with standard treatments for harmful drinking and alcohol dependence.
Brief intervention
GPs can have a major impact in reducing alcohol consumption by a simple technique called a brief intervention. Brief interventions can range from 5 to 10 minutes and are targeted at people drinking excessively but not yet experiencing major problems from their consumption. Brief interventions have been shown to produce a 13–34% reduction in weekly drinking, which means 2.9–8.7 fewer mean drinks per week.
The aim of the intervention is to:
Convince the patient that he or she is drinking harmful levels of alcohol and encourage reduction of consumption to sensible limits, thus reducing the risk of future health problems Explain the dangers of excess drinking: liver damage, cardiovascular damage, cerebral damage, peripheral neuropathy and cancers of the mouth, larynx, throat lips and oesophagus Assess patients who drive to ascertain whether other people are at risk. If that is the case, patients should be advised not to drive and to inform the Driver and Vehicle Licensing Authority (DVLA) Assess whether the patient's job means that others are being put at risk. For example, an airline pilot who is drinking excessive amounts of alcohol may put himself, his crew and all his passengers at risk Agree on a set goal, which is either abstinence or lower risk drinking, and discuss methods to achieve this
Where possible, support any advice given with written self-help materials and information on local support organizations. Offer a follow-up appointment in 1 month, then three monthly for as long as the patient seems to be at risk. Monitor progress by asking the patient to keep an alcoholic drink diary for 1 week before each appointment. Sometimes it also helps to use GGT monitoring as a motivational tool to encourage the patient.
AUDIT screening tool to assess severity of alcohol problem
How often do you have a drink containing alcohol?
Never Monthly or less 2–4 times a month 2–3 times a week 4 or more times a week How many standard drinks containing alcohol do you have on a typical day when drinking?
1 or 2 3 or 4 5 or 6 7 to 9 10 or more How often do you have six or more drinks on one occasion?
Never Less than monthly Monthly Weekly Daily or almost daily During the past year, how often have you found that you were not able to stop drinking once you had started?
Never Less than monthly Monthly Weekly Daily or almost daily During the past year, how often have you failed to do what was normally expected of you because of drinking?
Never Less than monthly Monthly Weekly Daily or almost daily During the past year, how often have you needed a drink in the morning to get yourself going after a heavy drinking session?
Never Less than monthly Monthly Weekly Daily or almost daily During the past year, how often have you had a feeling of guilt or remorse after drinking?
Never Less than monthly Monthly Weekly Daily or almost daily During the past year, have you been unable to remember what happened the night before because you had been drinking?
Never Less than monthly Monthly Weekly Daily or almost daily Have you or someone else been injured as a result of your drinking?
No Yes, but not in the past year Yes, during the past year Has a relative or friend, doctor or other health worker been concerned about your drinking or suggested you cut down?
No Yes, but not in the past year Yes, during the past year
Scores for each question range from 0 to 4, with the first response for each question (e.g. never) scoring 0, the second (e.g. less than monthly) scoring 1, the third (e.g. monthly) scoring 2, the fourth (e.g. weekly) scoring 3 and the last response (e.g. daily or almost daily) scoring 4. For questions 9 and 10, which only have three responses, the scoring is 0, 2 and 4.
A score of 8 or more is associated with harmful or hazardous drinking. A score of 13 or more in women, and 15 or more in men, is likely to indicate alcohol dependence.
Bear in mind the patient may not be receptive to intervention on first consultation and repeated consultations may be necessary. Further information on identification of problem drinkers and provision of brief advice can be obtained from the Department of Health at the following website: www.alcohollearningcentre.org.uk.
Alcohol dependence
Patients who have an addiction and severe depression, especially with suicidal ideation, should be referred to the community alcohol team. These teams offer specialist care, detoxification, individual and group counselling and support.
Warn the patient that persistent alcohol misuse or dependency must be reported to the DVLA and will result in suspension of the individual's driving license. Driving licenses may be restored for car drivers after at least 6 months of abstinence or controlled drinking.
Use the methods described in the brief intervention to encourage the patient to seek a goal of abstinence. Involve family and friends and alcohol support organizations to provide support. Encourage the patient to seek help from Alcoholics Anonymous as evidence supports the use of their 12 step facilitation programme. Identify others who will attempt to sabotage the patient's attempts at abstinence because of their own drinking habits and advise patients to avoid these individuals.
Detoxification refers to the planned withdrawal of alcohol and carries risks. It is the first step to achieving abstinence in patients with alcohol dependence. Community detoxification is an effective and safe treatment for patients with mild to moderate withdrawal symptoms. Detoxification for those with severe symptoms should be managed as an inpatient and these patients should be referred to community alcohol teams for supervised detoxification.
Specialist services use protocols specifying daily monitoring of breath alcohol level and withdrawal symptoms and benzodiazepine adjustment. When medication to manage withdrawal is not needed (Fig. 1), patients should be informed that at the start of detoxification, they may feel nervous or anxious for several days, with difficulty in going to sleep for several nights. Tapered dosing of benzodiazepines should be used in primary care to manage withdrawal
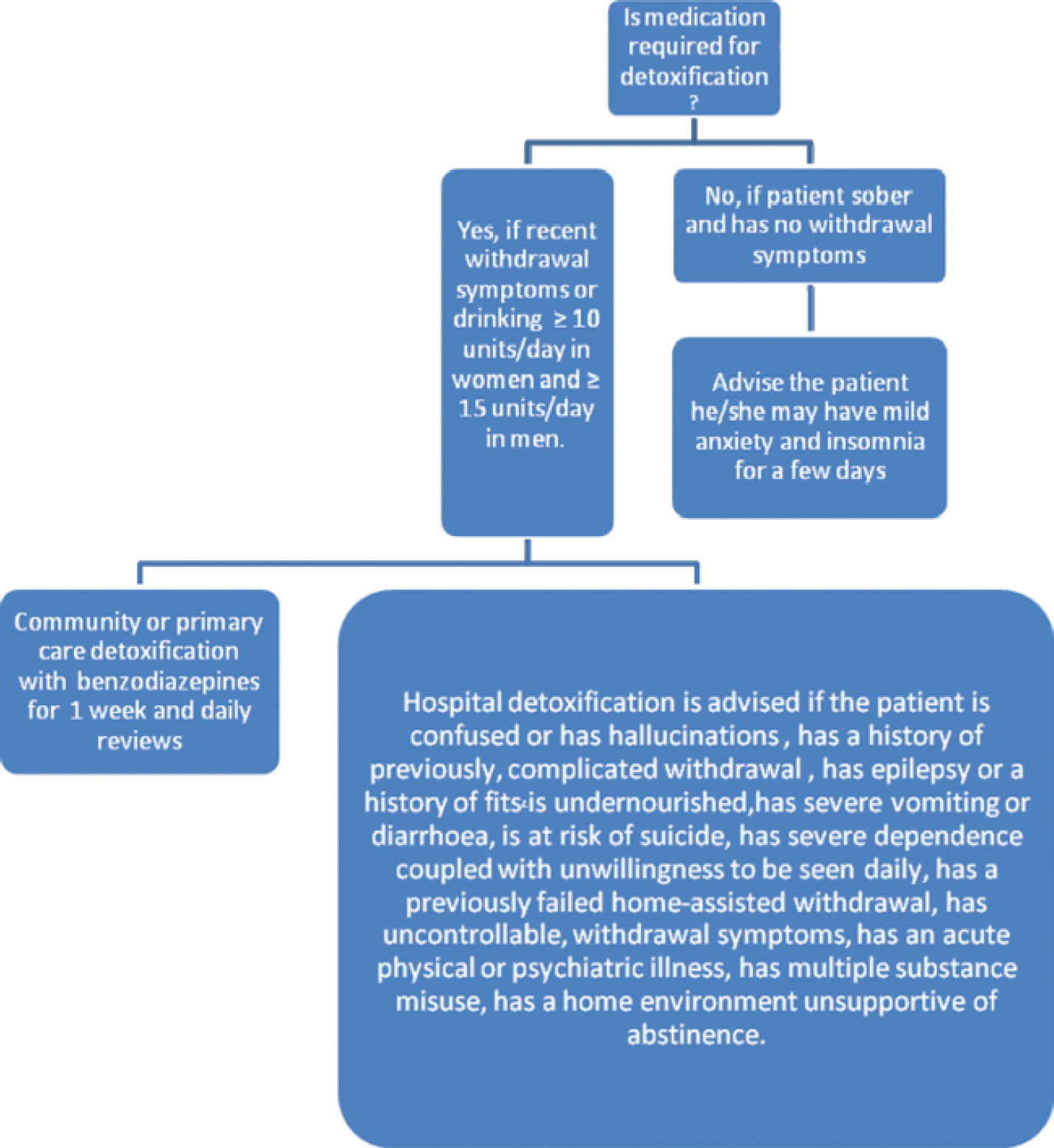
Assisting withdrawal from alcohol.
symptoms in alcohol detoxification, but for a maximum period of 7 days. For patients managed in the community, chlordiazepoxide is the preferred benzodiazepine. Although chlordiazepoxide is an effective treatment, there are well-documented fatal interactions with alcohol, which render it unsafe to use without close supervision; therefore, it should not be used by GPs without community alcohol team input.
Vitamin supplements
Patients with any sign of Wernicke–Korsakov syndrome (confusion; ataxia, especially truncal ataxia; ophthalmoplegia; nystagmus; memory disturbance; hypothermia and hypotension; coma) should receive Pabrinex in a setting with adequate resuscitation facilities. Pabrinex contains thiamine, riboflavin, pyridoxine hydrochloride, ascorbic acid and nicotinamide. The treatment should be according to British National Formulary (BNF) recommendations and should continue over several days, ideally in an inpatient setting. Patients detoxifying in the community should be given intramuscular Pabrinex (one pair of ampoules daily for 3 days) if they present with features, which put them at risk of Wernicke–Korsakov syndrome.
Patients who have a chronic alcohol problem and whose diet may be deficient should be given oral thiamine indefinitely. The BNF recommended dose for treatment of severe deficiency is 200–300 mg daily.
Delirium tremens
Major withdrawal symptoms from alcohol usually occur 2–3 days after the initiation of abstinence and can last up to 7 days. Delirium tremens has a 20% mortality rate and therefore requires emergency hospital admission. The risk is significant in any patient who drinks 12 U or more per day; however, it may occur in patients drinking as little as 8 U/day.
Delirium tremens is defined as withdrawal symptoms complicated by disorientation, hallucinations or delusions. Autonomic overactivity is a potentially fatal aspect of this condition. General features include fever, tachycardia, raised blood pressure and respiratory rate. Psychiatric features include vivid visual and tactile hallucinations, acute confusional state and apprehension. Neurological signs include tremor, fits and fluctuating consciousness levels. There is often a coexisting medical condition such as pancreatitis, pneumonia or other infection, which may lead to additional life-threatening complications.
Long-term management
Patient motivation, self-help and support organizations such as Alcoholics Anonymous are essential in maintaining abstinence, as well as counselling and psychological therapies, which help in preventing relapse. Patients need to know that if they relapse, there are still support strategies in place. Encouragement to contact the GP if a relapse has occurred is vital to help subsequent attempts have a more successful long-term outcome.
There is good evidence for the use of some medications in improving drinking behaviour as an adjunct to psychosocial interventions. Consider acamprosate to reduce the craving and disulfiram to reduce the number of days drinking takes place. Disulfiram acts as a deterrent in the knowledge that it is dangerous to drink alcohol from 12 hours before the first dose until 1 week after the last dose.
The GP should offer regular follow-up and monitor for underlying depression. The first assessment for depression should be made at least 2 weeks after the patient has stopped drinking. If depressive symptoms persist for more than 2 weeks following treatment for alcohol problems, consideration should be given to using a selective serotonin reuptake inhibitor (SSRI) antidepressant in addition to self-help guides, patient education, organized support groups and psychological therapies.
Detecting depression
Like ‘problem drinking’, depression is also a sensitive and stigmatized subject and effective communication skills can encourage the patient to open up about depressive symptoms within the consultation. Despite its high prevalence, 30–50% of cases of depression are not detected and polls indicate that 60% of people feel too embarrassed to consult their GP. The psychological and social situation of some patients makes them vulnerable to depression. GPs should be proactive and screen for symptoms. NICE recommends routine screening for specific high-risk groups:
Patients with significant physical illness and their carers—this includes not only people on chronic disease registers for diabetes, stroke and coronary heart disease but also patients with other chronic conditions such as those with Parkinson's disease, multiple sclerosis or spinal injury Patients with other mental health problems, including alcohol misuse, anxiety, dementia or multiple physical complaints Patients suffering major life events, such as childbirth, long-term or recent unemployment, family illness and bereavement Patients with a history of divorce or relationship difficulties and physical, sexual or emotional abuse
Depression in people from the African-Caribbean, Asian, refugee and asylum-seeking communities is easy to overlook, although the prevalence is 60% higher than in the Caucasian population, so consider regular screening in these populations groups also.
Box 4 provides the two recommended questions for use in screening. If a positive response is given for either question, GPs should use a formal assessment tool such as the International Classification of Disease (ICD-10) checklist or Patient Health Questionnaire (PHQ-9) to formulate a diagnosis and assess severity.
NICE depression screening questions
During the last month, have you often been bothered by feeling down, depressed or hopeless? AND During the last month, have you often been bothered by having little interest or pleasure in doing things?
If the patient's response to BOTH questions is ‘no’, the screen is negative.
If the patient responds ‘yes’ to EITHER question, the screen is POSITIVE.
A depression assessment tool such as the PHQ-9 or the ICD-10 checklist should now be used to assess severity.
The ICD-10 checklist to assess severity of depression
Have any of the following occurred most of the time for 2 weeks or more:
Sleep disturbance (difficulty falling asleep/early morning wakening) Appetite disturbance (appetite loss/increase) Poor concentration or indecisiveness Agitation or slowing of movement Decreased libido Low self-confidence Suicidal thoughts or acts Guilt or self-blame
Conclusion:
Positive to A, B or C and:
Four of the associated symptoms above = MILD (able to continue functioning)
Five to six of the associated symptoms = MODERATE (difficulty with normal activities)
Seven or more of the associated symptoms = SEVERE (distressed; suicidal and somatic symptoms common)
Differential diagnosis of depression
Patients with schizophrenia or other psychotic illnesses can present with depressive symptoms, so it is important to exclude this by looking for evidence of a thought disorder, delusions or hallucinations. Another differential diagnosis is bipolar affective disorder; therefore, it is essential to enquire about manic features. Latrogenic causes of depression include antihypertensives, steroids, beta blockers and H2 receptor blockers, so look into the medication history. Also consider life events such as childbirth, bereavement, work stress, unemployment, family illness and divorce.
Signs, symptoms and severity
The patient's general appearance may reveal signs of depression. Self-neglect, the smell of alcohol and cachexia can be spotted easily. A depressed or tired-looking patient, poor rapport with monotonous speech or monosyllabic words, avoidant eye contact, a jumpy or fidgeting patient, a feeling of distance, poor concentration and psychotic features can also be picked up during the course of the consultation.
NICE recommends the categorization of patients by mild, moderate or severe levels of depression on the basis of depression assessment tools, so as to guide clinical decision making.
Suicide and risk
In all patients with an alcohol problem, depression or a dual diagnosis, GPs must assess the risk of suicide and harm to others in a sensitive but probing manner. People misusing alcohol are a high-risk group and even among non-problem drinkers, alcohol is often consumed prior to the suicide attempt. In total, 15–25% of suicides are associated with alcoholism. Recent evidence shows that asking about suicidal ideation directly does not increase the patient's risk of a suicidal or parasuicidal attempt, so enquire about any intentions, plans and actions past and present. Explore the likelihood that the patient will act on thoughts or plans and ask what is stopping the patient from killing or harming himself or herself.
Ask:
Have you thought how nice it would be if you didn't wake up in the morning? Have you thought about killing yourself? Have you decided how to do it? Have you decided when to do it?
If the patient answers ‘yes’ to any of these questions, explore further.
Box 6 provides a list of risk factors that should also be taken into consideration and Table 2 offers a risk management plan. It is also important to ask about risk to others especially where people are not known to the practice. Safeguarding the patient and others, especially children, is paramount. A forensic history may be useful in ascertaining the risk to others.
Categorizing risk of suicide

Advise patients and carers to be vigilant for changes in mood, negativity and hopelessness and suicidal intent, particularly during high-risk periods such as during initiation of and changes to medication and increased personal stress. Advise patients and carers to make contact if concerned.
Assess whether patients with suicidal ideas have adequate social support and are aware of appropriate sources of help and advise them to seek help if the situation deteriorates. Where a patient presents considerable immediate risk to self or others, consider an urgent referral to a specialist mental health service. Make contact with patients with depression who do not attend follow-up.
Risk factors for suicide
History of previous attempts—were they planned or violent; was a suicide note left? Intense feelings of worthlessness or hopelessness Major mental illnesses including severe depression Suicidal ideation or evidence of planning Chronic physical illness or chronic pain Recent bereavement or other significant loss including redundancy/unemployment Male gender—the male:female ratio for suicide is 4:1 Old age—patients over the age of 75 years have three times the risk of 15- to 24-year-olds Age 40–60 years Alcohol or other substance misuse Previous inpatient psychiatric treatment Family history of mental illness, suicide or alcoholism AIDS or HIV-positive patients Marital status—divorced people are most likely to attempt suicide, followed by widowed people, then single people, with married people being least likely to commit suicide Living alone
Management of depression
NICE guidelines offer recommendations within a stepped care framework that aims to match the needs of people with depression to the most appropriate services, depending on the characteristics of their illness and their personal and social circumstances (Fig. 2). Each step represents increased complexity of intervention, with higher steps assuming interventions in previous steps.

The stepped care for depression.
The following are key implementations for primary care:
Watchful waiting
Watchful waiting can be employed as a management strategy or depression in the primary care setting as the patient may not want treatment and/or may recover with no intervention. A follow-up assessment should be made 2 weeks later.
Guided self-help
Advice on sleep hygiene and structured exercise programmes of up to three sessions per week of moderate duration (45 minutes to 1 hour) for between 10 and 12 weeks can help alleviate depression. Guided self-help material and limited support over 6–9 weeks, including follow-up, can also be effective.
Psychological treatments
Psychological interventions can be introduced in primary care and many practices employ a mental health worker such as a counsellor, mental health nurse, psychologist or psychotherapist. In mild and moderate depression, consider treatment specifically focused on depression [problem-solving therapy, brief cognitive behavioural therapy (CBT) and counselling] of six to eight sessions over 10–12 weeks. Computerized CBT is also now available. Although counselling is popular, evidence of efficacy in depression is lacking; however, it has been shown to assist patients in maintaining abstinence or ‘controlled drinking’ within safe limits.
Prescribing antidepressants
Antidepressants are not recommended for the initial treatment of mild depression because the risk:benefit ratio is poor. However, if depression persists, consider initiating a selective serotonin reuptake inhibitor (SSRI).
In moderate to severe depression, dysthymia and persistent mild depression offer antidepressant medication to all patients routinely, before psychological interventions. Discuss the patient's fears of addiction and reassure that craving and tolerance do not occur. When starting treatment, tell patients about the risk of discontinuation symptoms and potential side effects. Inform patients about the delay in onset of effect, the time course of treatment and the need to take medication as prescribed. Patient information leaflets are useful in providing all this information. SSRIs have been shown to improve depression outcomes in those who have had standard treatment of alcohol dependence.
Monitoring
The PHQ-9 depression tool can be used to assess severity and monitor response to treatment. The PHQ-9 score, which is out of 27, has acceptable reliability, validity, sensitivity and specificity as an assessment tool for the diagnosis of depression in primary care. The definition of improvement can be identified in a reduction of two or more points from the baseline score. Patients are not improving if they drop one point, there is no change in their score or if it increases. The definition of remission is a PHQ-9 score of less than 5 and that is the eventual goal of treatment in those who are acutely depressed.
Referral to local mental health service
Refer to your Community Mental Health team if the patient has any of the following:
Psychotic features are present Risk of real suicide and self-neglect Admission is being considered; severe depression, risk of self-neglect, social isolation, little family support and poor compliance Selection of an antidepressant is difficult due to associated physical illnesses or drug interactions Other forms of treatment are required that are not available in primary care (e.g. CBT) Patient is a child or adolescent with major depressive illness Poor response to an appropriate antidepressant in maximum dosage, with good compliance, taken for an adequate period of time
Long-term outcomes
‘Problem drinking’ is a continuum and needs regular follow-up to encourage motivation and help support patients.
Many people who successfully detox will relapse at some point and may have quite a few attempts until they are permanently abstinent. It is thought that relapses are less likely with counselling and other support strategies. The GP and community alcohol teams may provide ongoing support once abstinence has been achieved. Self-help groups such as Alcoholics Anonymous have also helped many patients remain abstinent. Once the alcohol problem has been alleviated, it is easier to assess and treat any underlying depression. Regular access to GP and primary care mental health workers, in addition to CBT and antidepressant treatment, can help patients make a good recovery.
Key points
Problem drinking is very common in the UK and can lead to physical and mental health problems. Despite the prevalence of patients presenting to GPs with problems relating to heavy alcohol intake, they often fail to make the association. Screening for alcohol problems is important to identify patients who may be unaware of the implications and provide early intervention Once harmful drinking has improved or alcohol dependence has been treated, it is important to assess for any underlying depressive disorder Alcohol can mimic depression and depressed patients may self-medicate with alcohol, developing tolerance and dependence Treatment encompasses patient education, self-help, psychological therapies, medication and specialist services such as community alcohol teams and dual diagnosis services. Relapse is common in those with alcohol dependence thus emphasizing the importance of regular monitoring in primary care
Footnotes
Acknowledgement
We would like to thank Dr Lesley Ayling for her help with the writing of this article under the InnovAiT ‘buddy’ scheme.