
Abstract
Head lice infestation results from colonization of hairy skin by Pediculus capitis, a wingless blood-feeding parasite of the order Phthiraptera. Head lice remain a significant problem as they may cause intense pruritus, and infestation is socially and psychologically stigmatizing. The prevalence of infestations has been increasing and is higher in children aged 4–11 years, in parents of young children and in urban areas. This possibly results from an increase in social mixing and movement around the country. Over a third of children in the United Kingdom will host head lice during any year and surveys show that one to two of every 10 children have head lice at any one point in time. This article aims to provide an overview of head lice infestation and its management in primary care.
The GP curriculum and head lice infestations
Manage primary contact with patients who have a skin problem
Work with patients to empower them to look after their own health and take responsibility for managing their skin problems
Promote skin well-being by applying health promotion and disease prevention strategies appropriately
Have knowledge of treatments commonly used in primary care (including an awareness of appropriate quantities to be prescribed and how to apply them)
Manage primary contact with children and their families
Ensure that parents or carers, children and young people receive information, advice and support to enable them to manage minor illnesses themselves, using community pharmacists where appropriate
Develop and apply the primary care consultation to bring about an effective doctor, patient and family relationship to enable parents or carers, children and young people to be routinely involved and supported in making informed decisions and choices about their care
Achieve concordance, including active listening and shared decision-making with children, young people and parents
Give information on medicines to children, young people and parents in a clear way
Promote health and well-being by applying health promotion and disease prevention strategies appropriately
The life cycle of the head louse
There are three stages to the life cycle of the head louse: the egg, the nymph and the adult louse. Lice eggs are attached to hair shafts with a type of glue and take a week to hatch. They are oval and white or light yellow in colour and 0.3–0.8 mm in size. Technically, nits (Fig. 1) are empty lice eggs that remain attached to the hair shafts, but in general usage ‘nits’ has been adopted as a popular term for head lice infestation. The nits are extremely tough and can stay in the hair for months or years.

Nits. Reproduced with permission from DermNet NZ, website of New Zealand Dermatological Society Incorporated.
Nymphs are immature lice. Outwardly they appear the same as adult lice, just smaller in size. Nymphs start feeding immediately — bites are normally painless. Nymphs take about 9–10 days to mature into adults.
Adult lice (Fig. 2) are wingless and about the size of a sesame seed when matured. They are grey or brown in colour, and the legs have claws to grasp hair shafts firmly. Male and female lice mate within a day of becoming adults, and a female can lay up to 150 eggs in her 30 day life. They feed by piercing the skin and sucking blood from the scalp of their host. Transmission is from close head-to-head contact. Lice are unable to fly, jump or swim. Contrary to popular public belief, head lice are not transmitted by pets nor are they more common on dirty hair.

Adult Pediculus capitis. CDC/Dr Dennis D. Juranek.
Symptoms and signs
Head lice infestation is normally asymptomatic. If symptomatic, the main symptom is scalp pruritus that results from the host's reaction to lice saliva following bites. This is a delayed hypersensitivity reaction and can take weeks to manifest fully. Head lice have a particular affinity for hair of the scalp and neck and itching occurs most aggressively over the occiput. Pruritus can persist for weeks following treatment.
Inspection of the scalp of an affected individual reveals the bite sites as red lesions; the lice themselves, as grey or reddish brown insects, crawling on the scalp and nits (oval shaped, small and yellow—white in colour) firmly attached to hair shafts. On occasion, the bites can become secondarily infected causing impetigo and crusting at bite sites. Lymphadenopathy is rare and is more common if bites have become infected.
Diagnosis
The diagnosis of head lice infestation can only be made if there are living lice present. The presence of nits alone is inadequate. If one member of the family has been diagnosed, the whole family must be checked.
There are two ways of detecting head lice infestation: visual detection or with a louse comb. Visual detection underestimates the level of active infection and a louse comb is four times more effective in detecting active infection. The teeth of the comb must be no more than 0.3 mm apart. The entire head is combed thoroughly with a louse comb and its teeth examined for the presence of live lice after each combing (Box 1). Usual infestation consists of around 30 lice per head.
Step by step instructions for children and parents for wet detection combing
Note: It is important that all members of the family are checked for head lice on the same day. It takes 20–30 minutes to thoroughly check a head for head lice.
Wash the hair using ordinary shampoo and apply a conditioner
Comb the hair with an ordinary comb initially until the comb moves freely
Then start combing with the detection comb with the teeth of the detection comb touching the skin of the scalp at the top of the head
Draw the detection comb carefully towards the edge of the hair
Look carefully at the teeth of the comb in good light
Do this repeatedly in all directions, working around the head
Rinse the conditioner off and repeat the process with wet hair
If there are head lice, you will find one or more 1–4 mm long lice on the teeth of the comb. If you are unsure, brush the louse onto a piece of white paper and observe it for movement — it will move if it is a live louse.
If it is unlikely that a family will comply with wet detection combing because of poor motivation or because there are a number of children in the family, dry detection combing is an alternative. The technique is much the same, but without the washing or conditioner, it takes less time to perform.
Differential diagnosis
Pediculus capitis infestation can be confused with pubic lice (Phthirus pubis) or body lice (Pediculus humanus) but the location is key to diagnosis. Pubic lice are found in pubic hair, eyebrows, eyelashes, axillary hair, moustaches and beards. Body lice are generally found on clothes, despite feeding on the body.
Nits may be confused with seborrhoeic scales, hair muffs (secretions from the hair follicle that appear wrapped around the hair shaft) and hair spray residue. Here, the key is the response after combing — nits remain firmly adhered to hair despite combing.
As patients often present to the GP with an itchy scalp rather than head lice infestation per se, it is also important to bear in mind the common differential diagnoses of an itchy scalp:
Seborrhoeic dermatitis
Eczema
Hair product allergy
Scalp psoriasis
Tinea capitis
Scalp cellulitis
Psychogenic itch
Management
General measures
Only treat head lice infestation if living lice have been detected. The goals of treatment are not only to eliminate live lice and eggs but also to prevent both reinfestation and transmission. All affected family members must be treated simultaneously. The main first-line treatments are wet combing, insecticide or dimeticone (Table 1). No treatment is 100% effective. For women who are pregnant or breast feeding, wet combing or dimeticone are the best options, but if an insecticide is essential, the National Teratology Information Service recommends malathion.
Advantages and disadvantages of treatment strategies for head lice infestation
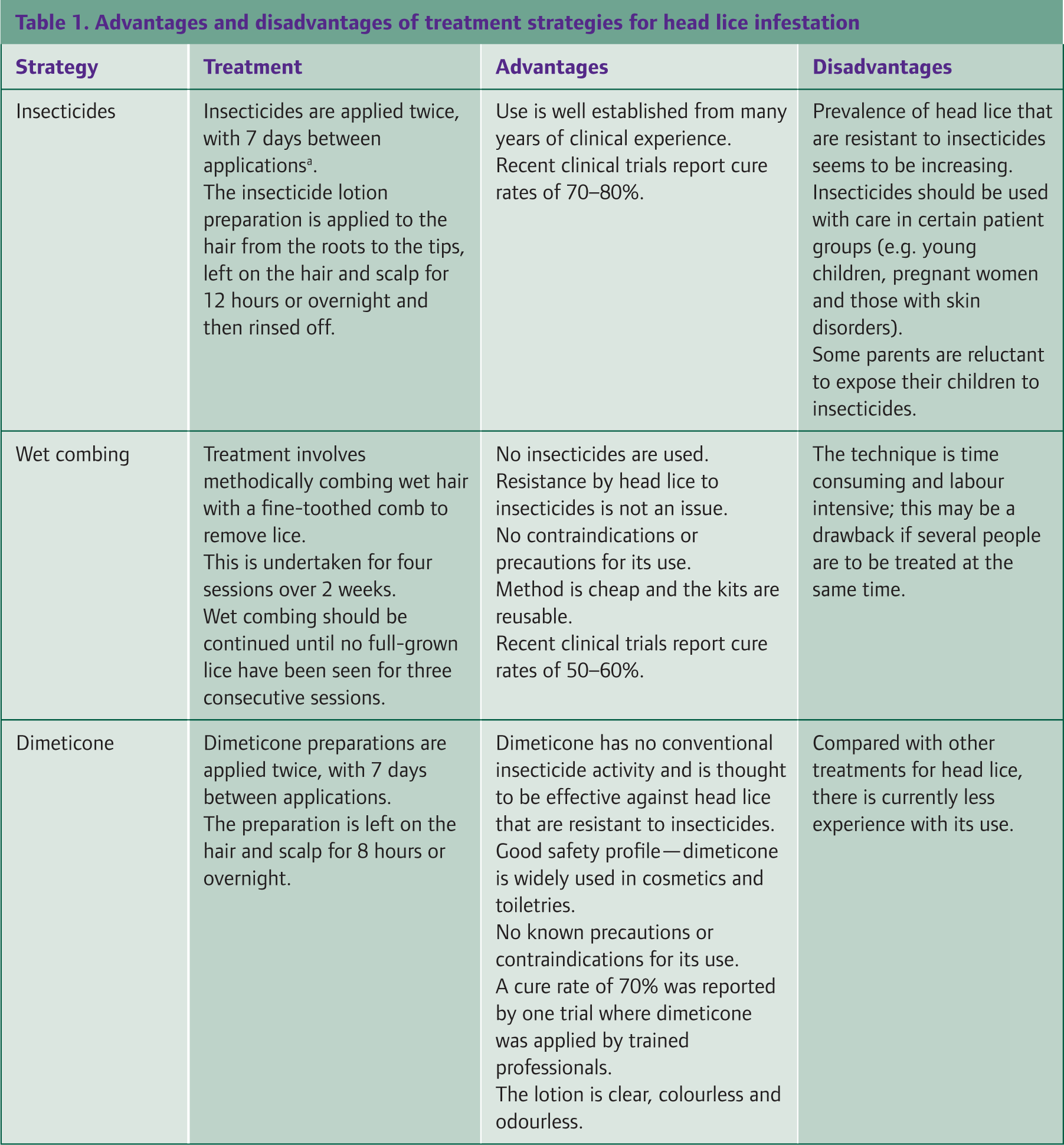
The recommendation for a second application of insecticide 7 days after the first is unlicensed for phenothrin: the package insert states that a single application is sufficient. However, malathion is now licensed for a second application of insecticide after 7 days. Insecticides should not be used more than once a week and should be used for not more than 3 consecutive weeks. Reproduced with permission from NHS Clinical Knowledge Summaries.
Offer the patient and/or parent a choice of treatments, explaining the advantages and disadvantages of each. Make them aware that without treatment, head lice infestation will persist and is unlikely to resolve spontaneously.
All treatment modalities require more than one treatment: insecticides need two applications a week apart, and wet combing must be done every 4 days for at least 2 weeks. Compliance is essential for successful treatment.
There is no evidence that washing clothing or bedding that has been in contact with affected individuals reduces the reinfestation rate. Head lice away from the human host rarely survive long enough to cause reinfestation. There is no justification for school exclusion for children with head lice.
Wet combing
Wet combing involves wetting the hair and combing with a louse comb, as for detection purposes, for 30–60 minutes every 4 days for at least 2 weeks (four applications). Continue combing every 4 days until the absence of grown lice is seen for three consecutive sessions. The use of shampoo or conditioner can facilitate combing. The first session should remove all currently hatched head lice and subsequent sessions newly hatched lice.
Mechanical removal is usually less effective than insecticides as it requires a great deal of motivation from the family to do correctly. In current practice, wet combing remains a first-line treatment option in pregnancy, lactation and when patients decline chemical treatment. There may be a greater role for wet combing in future as resistance to pediculicides is a growing problem. Louse comb packs are available as ‘Bug-Buster’ kits on National Health Service (NHS) prescription.
Insecticides
Many patients prefer insecticides as first-line treatment. These have either an aqueous or an alcoholic base. Aqueous preparations are normally favoured as alcohol-based preparations can cause hypersensitivity reactions in those with atopy, as well as being flammable. There is no evidence of difference in efficacy between the two bases.
If the individual has not yet used an insecticide, malathion 0.5% aqueous liquid or phenothrin 0.5% aqueous liquid are usually recommended as first-line agents. Permethrin is not recommended for head lice treatment. The policy of rotating insecticides on a district-wide basis to prevent resistance is now thought to be ineffective.
Malathion is an organophosphate which acts by inhibiting the function of acetylcholinesterase leading to paralysis of the louse. Phenothrin is a pyrethroid which binds to sodium channels, again causing paralysis of the louse. Both these preparations can be bought over the counter. They both have pungent odours but are generally well tolerated.
Preparations are rubbed into dry hair and scalp and allowed to dry naturally and then washed off 12 hours later (usually the next morning). Repeat the treatment after 7 days aiming to kill any newly emerged nymphs.
The quantity of insecticide required depends on the length and thickness of hair, but generally 50–100 ml is sufficient for each application. Insecticides should not be used more often than once a week and for no longer than 3 consecutive weeks.
Dimeticone
Dimeticone (4%) lotion is an alternative to the traditional insecticide treatments for head lice infestation. It coats the lice and prevents the excretion of water. This interferes with water balance in the lice causing death. As it acts via a physical process rather than direct toxic effect on the lice, it is often effective in cases of insecticide resistance. It is safe to use in pregnancy and lactation.
Dimeticone lotion is rubbed into dry hair and scalp and allowed to dry naturally. After a minimum of 8 hours, it can be shampooed out. Treatment is repeated after 7 days. The average quantity required is 50–100 ml per single application.
Alternative therapies
Some patients prefer to use natural products such as tea tree, soya, sunflower and corn oils for treatment of head lice infestation. These probably act in much the same way as dimeticone, by coating and suffocating the lice. Aromatherapy has also been used. However, there is no robust evidence of efficacy of any of these treatments and so they are not recommended.
Assessing response to treatment
It is always necessary to check response to treatment by detection combing 2–3 days after completing a course of treatment. If no head lice or nymphs are found at this time, repeat the check 6–8 days later (8–10 days after completion of the treatment course). This will determine if any viable eggs have survived, if any live lice are still present or if reinfestation has occurred. Success is confirmed when both checks reveal no lice or nymphs. Persistence of infestation at this stage defines treatment failure.
Treatment failure
The most common causes of treatment failure are summarized in Table 2. If infestation persists following a full course of treatment, consider whether this may be secondary to:
inadequate materials — ineffective louse comb or insufficient supply of insecticide
incorrect technique
resistance to insecticide and/or
reinfestation
Likely causes of treatment failure and reinfestation

If inadequate materials or poor technique are thought to contribute, discuss repeating the treatment with the patient and/or parent. Re-educate and supply appropriate equipment. If the patient is unwilling to attempt the same treatment again, consider switching to a different treatment.
If treatment failure is thought to result from insecticide resistance, change the insecticide used and repeat the treatment. For example, use malathion if phenothrin was used initially or vice versa. If resistance to both agents is apparent, consider using carbaryl instead. Alternatively, switch to wet combing or dimeticone.
If the head lice were caught at a communal place, reinfestation is common. Treatment of reinfestation may be with the same treatment or using an alternative treatment strategy depending on patient/parent preference. However, it is important to ensure that all contacts of the affected individual are screened for head lice and affected individuals are treated simultaneously. This may require parents to liaise with their childrens' schools or organizers of other group activities that their children participate in.
Complications
The psychological effect of infestation
Head lice infestation historically has been linked in society to poor hygiene. Over decades, research has proven this association to be unsubstantiated and false. However, even today, there is a public perception that people who have head lice infestation are dirty. This stigma can result in failure to acknowledge infestation and also failure to ensure contact tracing. As well as the implications that this has for successful treatment, the stigma of head lice infestation can have long-lasting psychological effects.
This occurs in several ways. Social exclusion of individuals with head lice is common. It is not unusual for children with head lice to be sent home from school (although there is no need for this) or excluded from social activities with their peers such as birthday parties. This alone can result in loss of confidence and self-esteem. The stigma associated with head lice can also result in unkind comments or even bullying by peers, again affecting confidence and self-esteem. Furthermore, the perception that having head lice implies lack of cleanliness can cause feelings of guilt (e.g. parents often assume that it is their fault that they or their children have head lice), anxiety and in extreme cases fuel cleaning compulsions or social phobia.
As GPs, it is important that we address these issues with patients and parents. In all cases, emphasize that infestation is not linked to being dirty and is not anyone's fault. Provide written advice sheets where possible. Written information both reinforces the information that you have given and also provides the patient or parent with something to show others less well informed.
Medical complications
The medical complications of head lice infestation are fortunately rare and mild. They include excoriation, skin infection, dermatitis (Fig. 3) and loss of sleep secondary to continual itching.

Dermatitis secondary to pruritus.
Prevention of head lice infestation
Neither prophylactic insecticides nor wet combing are helpful in preventing infestation. However, wet combing has a role in early detection, and, if there is an outbreak at a school, weekly detection combing can lead to earlier treatment.
Key points
Head lice infestation is often asymptomatic, but may cause scalp pruritus. It is most common in 4- to 11-year-old children.
Diagnosis is with a louse comb and requires presence of live moving lice (not just an empty shell or ‘nit’)
Treatment options include wet combing, insecticides (malathion/phenothrin) or dimeticone — check for treatment response 2–3 days and 8–10 days after the end of the treatment course
Treatment is ineffective unless contacts are traced and those confirmed with infestation are treated simultaneously
Always consider the wider social and psychological effects of head lice infestation
Insecticides and regular wet combing are not effective as prophylaxis against infestation
Footnotes
Acknowledgement
We would like to thank Dr Paul Wainman for his help with mentoring us under the InnovAiT ‘buddy’ scheme during the preparation of this article.