
Abstract
Bowel obstruction is a common surgical emergency. It can affect the small or large bowel and there are a number of possible aetiologies. Management requires prompt identification and referral to secondary care for further investigation and possible surgical intervention. Early diagnosis and management planning are the key to reducing morbidity and mortality associated with bowel obstruction from any cause.
The GP curriculum and bowel obstruction
Three GP curriculum statements cover bowel obstruction.
Primary care management to include the ability to recognize and evaluate acutely ill patients
GPs to be able to describe the increased risk of acute events in patients with chronic or co-morbid disease (e.g. increased risk of bowel obstruction in patients with bowel malignancy or previous history of intra-abdominal operations)
The knowledge base of
Able to recognize the significance of symptoms such as abdominal pain, nausea and vomiting
Aware of secondary care management of digestive problems, including surgical options
Able to intervene urgently when patients present with an acute abdomen
Relevant gross anatomy
Small intestine
The small intestine consists of the duodenum, jejunum and ileum. It extends from the pylorus of the stomach to the ileocaecal valve, where at the caecum the ileum joins the first part of the large intestine. The length of the small intestine varies from 3 to 10 m, with the average being around 6.5 m. Resection of up to one-third or even half of the small intestine is compatible with a perfectly normal life but outcome does depend on whether other parts of the gut are involved, particularly the ileocaecal valve. Loss of the ileocaecal valve allows colonization of the small bowel by bacteria from the colon and is associated with increased long-term morbidity.
The duodenum is the widest and most fixed part of the small intestine. It curves in a C around the head of the pancreas and is 25 cm long.
The duodenum joins with the jejunum at duodenojejunal flexure. There is no sharp distinction between the jejunum and ileum but the bowel does change it's character from above downwards. The jejunum has a thicker wall with larger circular folds of mucosa (valvulae conniventes) and greater diameter lumen. This can be distinguished on plain radiography but the main distinction to make is between the small and large intestine. Small bowel has mucosal folds (valvulae conniventes), which project across the entire width of the bowel wall and the bowel tends to lie in the centre of the abdomen. On a plain radiograph of distended colon, the haustrations (sacculations) appear as incomplete lines across the lumen of the colonic wall.
Large intestine
The large intestine is subdivided into the caecum with the appendix, ascending colon, transverse colon, descending colon and sigmoid colon. These sections are followed by the rectum and anal canal.
The caecum is the first part of the large intestine. It is a blind intestinal pouch in the right lower quadrant. The vermiform appendix extends from the caecum. The caecum is almost entirely covered with peritoneum, has no mesentery and can be lifted freely. An embryonic deficiency in the peritoneum allows increased mobility of the caecum and may predispose to caecal volvulus.
The ascending colon is retroperitoneal and adheres directly to the posterior abdominal wall. It passes superiorly from the caecum to the right lobe of liver where it turns as the hepatic flexure to become the transverse colon. The transverse colon is the largest and most mobile part of the large intestine due to its long mesentery, the transverse mesocolon. It crosses from the hepatic flexure on the right to the splenic flexure on the left, where it blends inferiorly to become the descending colon. The descending colon is also retroperitoneal and like the ascending colon adheres to the posterior abdominal wall. It is linked to the rectum by the sigmoid colon, which is an S-shaped loop of variable length. The sigmoid colon usually has a long mesentery (sigmoid mesocolon) giving it considerable mobility, potentially allowing it to twist around its axis leading to volvulus.
Epidemiology
In the developed world approximately 20% of patients admitted to hospital with an acute abdomen have intestinal obstruction. Of these 20%, approximately 80% will have small bowel obstruction. The leading cause of small bowel obstruction is post-operative adhesions reflecting the increasing number of abdominal procedures performed. In the developing world, obstructed hernias are the most common cause of obstruction.
Pathophysiology
Obstruction of the intestinal lumen causes the bowel proximal to the blockage to dilate. This distension is produced by gas (from the overgrowth of aerobic and anaerobic bacteria and swallowed air) and fluid, which is secreted from the bowel wall while absorption from the gut is reduced. This causes multiple physiological events:
The increase in luminal content leads to increased peristalsis to aid transit along the bowel both proximal and distal to the obstruction. The peristalsis above the obstruction leads to severe colicky abdominal pain. Below the obstruction, peristalsis often causes diarrhoea in the initial stages of obstruction.
Dehydration and electrolyte loss
The overgrowth of bacteria within the gut proximal to the obstruction and microvascular changes in the bowel wall lead to dramatically increased bacterial translocation with significant bacteraemia and subsequent systemic inflammatory response
Ischaemia of the bowel and subsequent necrosis leading to perforation may occur. This is caused by vascular occlusion either by strangulation where the bowel twists on its own mesentery or is trapped in a hernial sac, or secondary to bowel wall distension and oedema, which impair local venous and subsequent arterial flow.
Below the obstruction peristalsis and absorption continue until the bowel becomes empty, when it contracts and becomes immobile.
Intestinal physiology and dehydration
In total, the gastrointestinal tract secretes around 6 l of fluid/day. This includes fluid from the
Stomach—2 to 3 l/day. Includes mucus, hydrochloric acid and pepsinogen.
Gallbladder—500 ml/day. Secretes bile.
Pancreas—1.5 l. Secretions from the exocrine pancreas include proteolytic enzymes (trypsin and chymotrypsin), amylase and lipase. These are secreted in inactive forms, being activated in the intestine. The pancreas also secretes large amounts of bicarbonate.
Small bowel—1.5 l/day. Brunner's glands in the duodenum secrete mucus rich in bicarbonate. The small intestine also secretes numerous digestive enzymes including disaccharidases (maltase and sucrase), peptidases, phosphatases and enteropeptidases.
This fluid secretion also involves ion exchange and can lead to large amounts of sodium and potassium moving between the cells of the gastrointestinal tract and the intra-luminal fluid. During normal health much of this fluid is reabsorbed in the small intestine, with some also absorbed in the large intestine. However, when there is obstruction of the intestine, this fluid cannot be reabsorbed. Large amounts of fluid and electrolytes are lost due to repeated vomiting, and there is fluid sequestration in the bowel lumen (third space loss). Hypovolaemia may also be exacerbated by reduced oral intake.
Classification
Intestinal obstruction may be classified as dynamic or adynamic.
Dynamic obstruction
Dynamic obstruction is where peristalsis is acting against a mechanical obstruction blocking the bowel lumen. This can be
Intra-luminal (e.g. impacted faeces and gallstones)
Intramural (e.g. malignant and inflammatory strictures)
Extramural (e.g. adhesions, hernias and volvulus)
Adynamic obstruction
There are two forms of adynamic obstruction. Peristalsis may be absent (e.g. paralytic ileus) or it may be present, but in a non-propulsive form (e.g. mesenteric vascular occlusion or pseudo-obstruction).
Pseudo-obstruction is a term for the syndrome in which patients present with symptoms and signs consistent with large bowel obstruction, but have no mechanical cause demonstrated on contrast radiology. In around 80% of cases, an underlying precipitating condition exists, the most common being metabolic disorders, trauma, cardiorespiratory disorders or medications (Box 1).
Common medications that may cause colonic pseudo-obstruction include anticholinergics, tricyclic antidepressants and anti-Parkinsonian medications. The GP should consider the potential risk of these medications in patients with previous episodes of pseudo-obstruction and also be aware that these medications may be stopped in hospital. Alternative choice or cautious reintroduction may be necessary.
Predisposing conditions in acute colonic pseudo-obstruction
Chest infection
Myocardial infarction
Cerbrovascular event
Iatrogenic (medications)
Renal failure
Puerperium
Retroperitoneal malignancy
Orthopaedic trauma
Myxoedema
Electrolyte disturbance
Aetiology of dynamic bowel obstruction
Adhesional small bowel obstruction is by far the most common cause of bowel obstruction (Fig. 1). The common causes of small bowel obstruction differ from the causes of large bowel obstruction. Intra-abdominal adhesions are the most common cause of small bowel obstruction, and malignancy is the leading cause of large bowel obstruction.
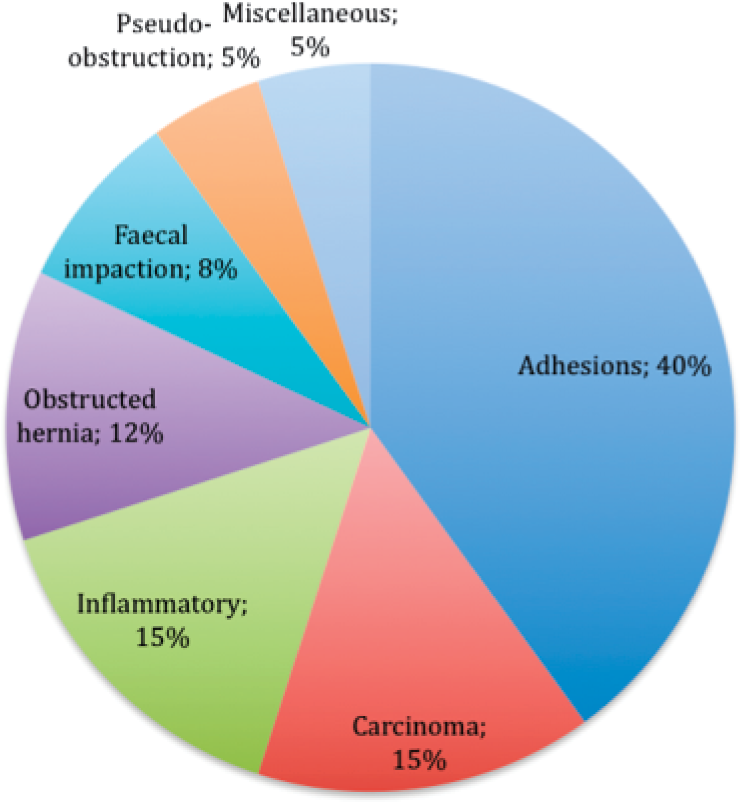
Causes of intestinal obstruction.
Small bowel obstruction
There are numerous causes of small bowel obstruction (Box 2) and treatment differs depending on aetiology.
Causes of small bowel obstruction
Within the lumen
Gallstones
Food bolus
Bezoars
Parasites
Enterolith
Foreign body
Within the wall
Tumour
Inflammation
Crohn's disease
Radiation enteritis
Post-operative stricture
Vasculitides
Outside the wall
Adhesions
Congenital
Acquired
Hernia
Primary
Secondary
Adhesions
Intra-abdominal adhesions are the most common cause of intestinal obstruction in Western countries accounting for approximately 40% of all cases. Adhesions develop following abdominal surgery (but may also be present without abdominal scars, following previous infections or as a developmental abnormality) as part of the normal healing process following disruption of the peritoneum. The exact mechanism for their development is a complex process involving several different cell types, cytokines, coagulation factors and proteases, which act together to restore tissue integrity.
The risk of developing post-operative adhesions is dependent on the type of surgical procedure, intra-operative complications and individual patient response. In general, there is a higher risk with procedures in the lower abdomen and pelvis. It is estimated that the risk of small bowel obstruction is 1–10% post-appendicectomy, 6% following open cholecystectomy, 10–25% after intestinal surgery and 17–25% following restorative proctocolectomy. It is therefore important for the GP to be aware of the increased risk of intestinal obstruction for patients who have had previous abdominal surgery.
Herniae
Herniae are the second most common cause of small bowel obstruction. It is important in all cases of suspected intestinal obstruction to examine all hernial orifices (both natural and incisional), and signs of possible obstruction include the hernia being tense, tender or irreducible and absence of the cough impulse. A special consideration is a Richter's hernia, which involves herniation of only part of the bowel wall without obstructing the lumen. In this case, there can be infarction of the trapped bowel segment and the patient will have exquisite localized tenderness over a potential hernia site. These patients may well not suffer from any absolute or partial constipation so it is important to be aware of this condition and the potentially misleading clinical signs.
Large bowel obstruction
Malignancy accounts for approximately 60% of all cases of dynamic large bowel obstruction. Other causes include diverticular disease (20%) and volvulus.
Malignancy
Intestinal obstruction secondary to carcinoma usually affects the large bowel. Patients may have noticed preceding symptoms suggesting colorectal malignancy, which would be dependent on the site of the tumour. Right colonic tumours may present with weight loss, altered bowel habit and malaise. Left colonic tumours generally present with overt rectal bleeding or the passage of mucus in addition to above symptoms.
Diverticular disease
Recurrent attacks of diverticulitis may cause narrowing of the bowel lumen. Patients will often present with distal colonic obstruction as diverticular are most common in the sigmoid colon and generally have a long history.
Volvulus
Colonic volvulus is another important cause of large bowel obstruction and is defined as an axial rotation of the colon around its mesentery. As the sigmoid colon is very mobile with a long mesentery, it is involved in 76% of cases, the caecum in 22% and transverse colon in 2%. Sigmoid volvulus usually occurs in the elderly, whereas caecal volvulus can be seen more commonly in younger patients as it results from a congenital malformation.
Intussusception
Intussusception is thought of as a paediatric condition but approximately 10% of cases of intussusception occur in adults. The majority of cases seen in adults are caused by tumours.
Mortality and morbidity
The mortality and morbidity rates of intestinal obstruction are dependent upon the aetiology and the patient's age at presentation. Strangulation with ischaemia of the bowel poses a greater risk to patients if unrecognized, with mortality as high as 25% if the delay in surgical intervention exceeds 36 hours.
Colonic pseudo-obstruction is thought to account for around 200 deaths in the United Kingdom per annum.
Clinical assessment in primary care
Intestinal obstruction presents with four key clinical features (Box 3), which are pain, vomiting, abdominal distension and constipation. These features vary according to the location, period of obstruction, the underlying pathology and the presence or absence of intestinal ischaemia.
Cardinal features of bowel obstruction
Vomiting
Pain
Constipation
Abdominal distension
In proximal small bowel obstruction vomiting occurs early and may be associated with rapid dehydration. There is minimal abdominal distension. This contrasts to low small bowel obstruction where pain predominates, there is central distension and vomiting is delayed.
In large bowel obstruction, the main presenting symptom is abdominal distension. Pain is mild, and vomiting and dehydration occur late.
Late manifestations of all forms of intestinal obstruction include dehydration, oliguria, hypovolaemic shock, pyrexia, septicaemia, respiratory distress and peritonism.
Pain
Pain is usually the first symptom in small intestinal obstruction. It occurs suddenly and is usually severe. The pain is usually colicky in nature and coincides with increased peristaltic activity. The development of severe pain is indicative of the presence of strangulation.
Vomiting
With more proximal obstruction, there will be a shorter interval before the onset of symptoms, including nausea/vomiting. Therefore, these symptoms are seen earlier in small bowel obstruction compared with pathologies that affect the large bowel. As obstruction progresses the character of vomited material changes from digested food to faeculent material.
Distension
In small bowel obstruction, abdominal distension is dependent on the site of blockage and is greater in more distal lesions. Peristalsis may be visible on inspection of the abdominal wall. Distension is a common finding in large bowel obstruction.
Constipation
Constipation can be classified as absolute (i.e. neither faeces nor flatus is passed) or relative (where flatus only is passed). Absolute constipation is a feature of complete intestinal obstruction. It is important to be aware that some patients may pass flatus and/or faeces in the early period following the onset of obstruction due to the evacuation of bowel contents distal to the obstruction.
Dehydration
Patients with small bowel obstruction will often appear significantly dehydrated. This is commonly multifactoral, related to reduced oral intake, defective intestinal absorption, vomiting and sequestration in the bowel lumen (third space loss). This commonly leads to severe hypovolaemia and electrolyte loss.
Clinical examination
Features of intestinal obstruction on clinical examination include features of hypovolaemia, including tachycardia, dehydration (with reduced skin turgor and dry mucous membranes) and hypotension. Hypotension and tachycardia may be secondary to hypovolaemia in simple obstruction but can also be caused by ischaemia and sepsis in strangulated obstruction, in which case these features will be resistant to fluid resuscitation.
Pyrexia in the presence of obstruction may indicate the onset of ischaemia, intestinal perforation or inflammation associated with obstructing disease. Hypothermia can also be present and may be an indication of septicaemic shock.
As mentioned previously, the abdomen may appear distended. The degree of distension is often dependent upon the site of the lesion and is more pronounced with large bowel obstruction than with proximal obstruction.
Simple obstruction causes poorly localized tenderness, which may not be severe. Localized abdominal tenderness is indicative of intestinal ischaemia. The development of peritonism or peritonitis indicates overt infarction and/or perforation. Right iliac fossa tenderness in large bowel obstruction may be a sign of closed loop obstruction with imminent caecal perforation.
In all cases of suspected intestinal obstruction, it is vital to examine all hernial orifices. In the case of a strangulated external hernia, the lump will appear tense, tender and irreducible, and there will be no expansile cough impulse.
On auscultation, bowel sounds may be high pitched and described as ‘tinkling’. Reduced bowel sounds are suggestive of bowel ischaemia.
Rectal examination is very helpful to differentiate between mechanical and functional obstruction. In mechanical obstruction, the rectum is often empty and collapsed, but it may be possible to feel rectal tumours or diverticular masses. In pseudo-obstruction, a cavernous, ballooned gas-filled rectum may be identified.
Features of strangulation
It is important to distinguish between strangulating and non-strangulating intestinal obstruction. In non-strangulating bowel obstruction, the blood supply is intact, whereas when strangulated there is direct compromise of blood flow to the intestine. Strangulating bowel obstruction is a surgical emergency and prompt referral is essential to improve patient outcome.
The presence of shock indicates underlying ischaemia. In impending strangulation, symptoms usually commence suddenly and recur regularly, and pain is never completely absent. Generalized tenderness and the presence of rigidity indicate a need for emergency referral, and these patients usually require prompt laparotomy.
Management in primary care
Patients in whom the GP suspects intestinal obstruction will require prompt referral to secondary care as a surgical emergency.
Patients should be made nil by mouth. If available, a large-bore nasogastric tube should be passed to decompress the gastrointestinal tract and intravenous fluids commenced if available. Analgesia is appropriate and is unlikely to mask vital diagnostic signs in the acute abdomen. Centrally acting anti-emetics (such as cyclizine) will help relieve nausea. However, medications that increase gastric emptying (such as metoclopramide) should be avoided.
Haemodynamic instability or signs of strangulation and peritonism require emergency referral to the nearest Emergency Department for assessment by the surgical team. This group of patients often requires stabilization in the emergency department and early intensive care input followed by an emergency laparotomy.
Investigation and management in secondary care
Investigation
Initial investigations will include full blood count, urea and electrolytes, amylase and group and save so that blood can quickly be crossmatched if operative intervention is necessary. Other important blood tests include trace elements, as deficiency of these may be a cause of pseudo-obstruction. Some hospitals may also check C-reactive protein (CRP) as part of the initial investigations.
Plain abdominal x-rays can confirm around 60% of cases of intestinal obstruction, with abnormally dilated gas-filled bowel loops being visible. In small bowel obstruction, bowel loops with bands (valvulae conniventes) can be seen to traverse the whole diameter of the gut (Fig. 2). Small bowel loops tend to be central, and pathological dilatation is considered to be present if the small bowel diameter exceeds 5 cm.

Supine radiograph from a patient with complete small bowel obstruction shows distended small bowel loops in the central abdomen with prominent valvulae conniventes. Miriam Maslo/SPL.
In large bowel obstruction, x-ray will show bowel with bands (haustra) that do not cross the gut. Dilated loops tend to be peripheral and not central. Pathological dilatation is present when bowel diameter is greater than 8 cm, or the caecum is dilated to above 10 cm. There is increased concern when large bowel obstruction is accompanied by a competent ileocaecal valve preventing any decompression.
In cases where the patient is stable, and urgent operative intervention is not required, computerized tomography (CT) scanning can be used in order to provide further information about the possible aetiology. CT will identify 95% of cases of obstruction. CT can show the cause as well as the level of intestinal obstruction, viability of involved bowel and any metastases in the case of malignant obstruction.
Management of dynamic obstruction
There are three main measures in the management of acute intestinal obstruction:
Gastrointestinal drainage
Fluid and electrolyte replacement
Relief of obstruction, usually surgical
Gastrointestinal drainage is usually facilitated by the passage of a large-bore nasogastric tube such as a Ryle's tube. These will be placed on free drainage, with aspiration at appropriate intervals. Other than decompressing the gastrointestinal tract these techniques also reduce the risk of aspiration from vomiting or during subsequent induction of anaesthesia.
Intravenous fluid replacement is necessary to rehydrate patients and correct any biochemical abnormality. The most common abnormality is sodium and water loss. There may also be significant loss of potassium causing hypokalaemia. Appropriate fluid therapy is with Hartmann's solution or normal saline with potassium replacement. Recent studies suggest that Hartmann's is preferable.
The use of intravenous fluids and nasogastric decompression in the management of intestinal obstruction can easily be remembered as the ‘drip and suck’ method. Patients without indications for surgery are routinely treated with a trial of conservative management. In a proportion of cases, particularly adhesive obstruction, these management techniques may be successful in relieving intestinal obstruction without the need for surgical intervention.
Some clinicians advocate the use of broad-spectrum antibiotics at an early stage due to bacterial overgrowth, but this remains controversial.
The timing of surgical intervention depends upon the clinical picture. In some cases, such as adhesional obstruction where there is no pain or tenderness, conservative management may be continued for up to 72 hours in the anticipation of a spontaneous resolution. However, indications for early operative intervention include obstructed or strangulated external hernia, internal intestinal strangulation and any evidence of peritonitis or perforation.
The type of surgical procedure necessary depends on the nature and position of the obstruction. This can take the form of division of adhesions (enterolysis), small or large bowel resection with or without formation of a stoma, a bypass procedure or proximal decompression with the formation of a defunctioning stoma.
Post-operative care
Depending on the patient's condition and nature of the procedure undertaken, patients will commonly spend a period of time on the intensive care unit post-operatively. Nasogastric tubes will be left on free drainage until there is minimal gastric aspirate, and intravenous fluids will be continued. Patients will remain nil by mouth until their surgical team feel it is appropriate for them to gradually reintroduce fluids and subsequently progress to a normal diet. If the patient has had a stoma formed during the operation, they will need to learn how to care for this and change the bag, usually being taught by specialist nurses. In the case where patients are unable to care for the stoma adequately themselves (e.g. elderly patients), then on discharge appropriate arrangements will be made with district nurses.
One retrospective study in Norway (Fevang et al., 2000) showed that average length of post-operative hospital stay for small bowel obstruction was 7 days. However, old age, non-viable strangulation and a treatment delay of more than 24 hours were found to be significantly associated with a longer post-operative period in hospital.
Management of adynamic obstruction
If no obvious cause for mechanical large bowel obstruction is found on contrast radiology, then it is important to identify any underlying cause for a pseudo-obstruction and treat these as appropriate. This includes discontinuing/changing any medications that may cause gut stasis and includes anticholinergics, tricyclic antidepressants and anti-Parkinsonian drugs.
A nasogastric tube is inserted to decompress the stomach and upper small bowel. Enemas and flatus tubes can also be used in an effort to decompress the large intestine. In most post-patients the condition will resolve without the need for further intervention, and one study by Bachulius and Smith (1978) found that it took an average of 6.5 days for complete resolution in a group of 26 patients treated medically. Patient improvement can be judged by regular abdominal examination and radiographs.
More active intervention may become necessary if the risk of perforation increases significantly (Box 4). One method to decompress the colon is via colonoscopy, and this is effective in 73–90% of patients. Although this procedure can be difficult, the risk of perforation during colonoscopy for this procedure is thought to be around 3%.
Indications for surgery in pseudo-obstruction include
Caecal distension
Continuing caecal distension beyond 48–72 hours despite maximum medical therapy
Pain over the right iliac fossa, i.e. the caecum
Perforation and pneumoperitoneum
Primary care management post-hospital discharge
Following discharge from hospital, patients who have undergone operative intervention may well have required the formation of a stoma. Stomas are often precautionary and it is often possible to reverse them at a subsequent operation. Having a stoma formed may be a psychological and social burden and they are often particularly difficult for younger patients to cope with. Patients may need support from their GP and other community services. Patients with ileostomies are at risk of high effluent output, which can lead to fluid and electrolyte disturbances. This must be recognized and appropriate advice and treatment sought. Many departments have community stoma nurses who are invaluable in this situation.
Other patients may have been diagnosed with colonic malignancy, and in some cases where this was inoperable the stoma will have been performed as a palliative procedure for the relief of obstruction. Again, these patients will require support in the community from appropriate services in order to optimize their quality of life.
Future developments
At present much work is being undertaken to fully understand the pathophysiology of adhesion formation. By furthering this knowledge it may be possible in the future to develop effective methods of preventing adhesional formation following intra-abdominal surgery. Currently, the most promising groups of agents are barriers, which exist as a membrane or gel and act to separate damaged or injured peritoneal surfaces that may be at risk for adhesions. The ideal barrier does not yet exist but the necessary characteristics are a substance that is antiadhesive, biocompatible, resorbable, adherent to the traumatised surface, effective on an oozing surface, applicable through a laparoscope and inexpensive. In addition adhesion formation is a highly preserved gene and despite known drawbacks has many advantages such as localizing infection and neo-vascularization. At least one study to date that examined a product, which inhibited adhesion formation, had to be abandoned because of an increased incidence of anastomotic leaks.
Key points
Bowel obstruction is a common presentation with various aetiologies
Patients who have had previous abdominal surgery are at increased risk of intestinal obstruction due to adhesions
It is important to examine all hernial orifices in cases of suspected bowel obstruction
By maintaining an awareness of this condition GPs can ensure prompt referral to secondary care, therefore reducing mortality and morbidity