
Abstract
In many ways, lives of men and women have become more similar over recent years, as more and more women have entered the labour market. Despite this, differences remain. These, in turn, affect both patients' experiences of health and disease and the health services required.
“The task of medicine is to promote health, to prevent disease and to treat the sick … These are highly social functions”
H. E. Sigirist, Civilization and Disease, 1943.
The GP curriculum and gender issues
This article directly relates to Royal College of General Practitioners (RCGP)
Treat patients, carers and others equitably and with respect
Act in ways that recognize that people are different and do not discriminate against people because of those differences
Recognize and take action to address discrimination and oppression in self and others
There are also some more specific statements about health related to gender in section 10 of the curriculum:
Recognize the issues of gender and power, and the patient-doctor relationship, and know how to prevent these issues adversely affecting health care
Describe the impact of gender on individual cognition and lifestyle and formulate strategies for responding to this
Understand the issues of equity and access to health information and services for women and men
Evaluate the effectiveness of the primary care service you provide from a gendered perspective
Describe the impact of culture and ethnicity on the perceived role of men and women in society and their attendant health beliefs, and tailor health care accordingly.
Biological differences between males and females are responsible for a differential experience of health and disease. A woman will not experience prostate cancer for instance. However, the differences between males and females go beyond the physical characteristics, which describe a person's sex, to include a vast array of social roles, behaviours and attributes. The term ‘gender’ is used for the social construct ascribed to someone because of their sex (Box 1), and it is the differences between genders that result in many variations in health experiences for males and females. This article is concerned with the impact of gender on primary care, recognizing that the differing status of men and women in a society affects their experience both as patients and as providers of health care.
Defining sex and gender
Demographic differences
Overall, there are more women than men in the UK population (30.3 × 106 women and 28.9 × 106 men). More boys than girls are born each year and there are roughly 20 000 more boys than girls at every age until 22 years, when the number of women overtakes the number of men. This difference increases with age. At 90 years of age, there are three and a half times as many women as men (Fig. 1).
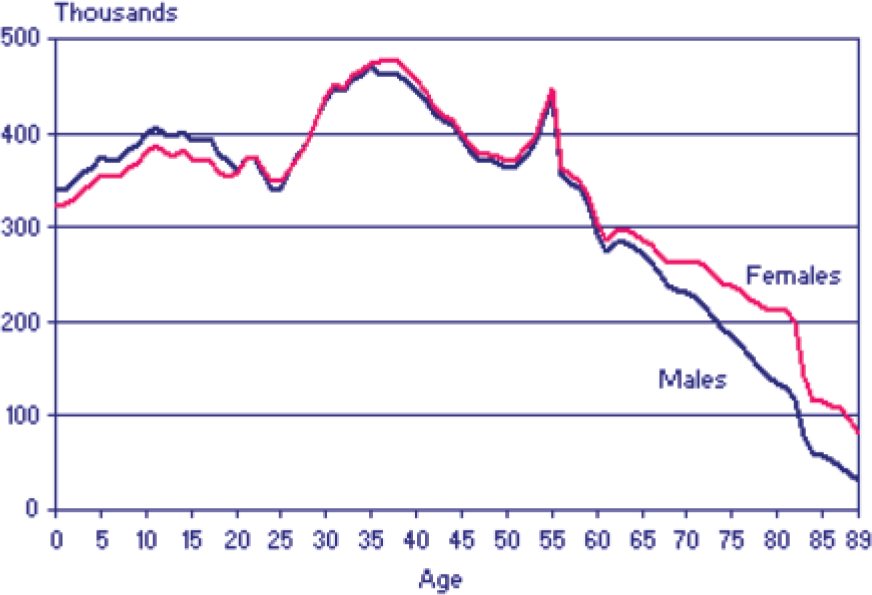
Male and female distribution of the UK population.
Gender and societal risk
In the UK, 60% of men and women live as a couple and 81% of couples live in owner-occupied accommodation. Over the past 30 years, the proportion of single or divorced people has increased. A quarter of families with dependent children in the UK are headed by a single parent: 22% by lone mothers and 3% by lone fathers (National Statistics Online, 2008). Of lone mothers, half have never been married but lone fathers tend to be divorced. Around a half of lone mothers with dependent children live in social sector housing.
Divorcees of all ages are at greater risk of premature death than married people. Death rate is doubled for divorced men aged 35–42 years—mainly as a result of cardio- and cerebrovascular disease, cancer, suicide and accidental death. There is also a similar increase in morbidity.
Among older people, there are more than three times as many widows as widowers in the population as women tend to live longer than men. Women are more likely to become informal carers than men as they are often still fit enough to perform caregiving duties when their spouses fall ill. As women tend to live longer than men, when an elderly woman becomes ill, she is two times more likely to go into residential care.
Homelessness
Homelessness is not defined by having a roof over your head. If a person does not have the right to stay in the home, or if the home is not fit to live in, that person is also technically homeless.
Roughly 90% of rough sleepers are male (peak age 26–49 years). Risk factors for homelessness include
Institutionalization—time in local authority care; contact with the criminal justice system; previous service in armed forces
Health—alcohol and/or drug misuse; mental health problems; past history of physical/sexual abuse
Relationship problems—disputes with parents/step-parents; marital/relationship breakdown; domestic violence
Education and work—learning difficulties and literacy problems; exclusion from school; lack of qualifications; unemployment
Others—housing shortage; previous homelessness; debt; benefit problems; refugees/asylum seekers
The homeless are more at risk of death, physical illness and contracting infectious diseases. In addition, half suffer from a mental illness of some sort, and up to 80% misuse drugs or alcohol. Multiple morbidity is high but a quarter to a half of homeless people report a medical problem for which they have not sought help and the homeless are 40 times more likely not to be registered with a GP.
Domestic violence
There is strong evidence that GPs under-detect people who are at risk of mental and physical abuse (Department of Health, 2005). Almost one in three women suffer domestic abuse in their lifetime. Risk factors include pregnancy (when incidence of abuse increases), addiction in the partner and a history of abuse in childhood in either partner.
Women who suffer domestic violence are often unwilling or unable to talk to anyone about their problems as a result of fear of further violence, embarrassment or fear of losing their home, family and means of financial support. They become socially isolated as a result. Warning signs may include psychological distress, unexplained injuries, missing appointments or booking late in pregnancy. Health care workers may perceive such behaviours as problematic, potentially hindering access to the support these women need.
Men may also experience domestic violence. This is more often emotional than physical. Less is known about this phenomenon as, due to gendered expectations and norms, men may be less likely to seek help when they are being abused.
Gender, work and income
Educationally, girls generally perform better than boys at all levels:
58% of girls achieve five or more GCSE grades A*—C compared to 47% of boys
At degree level, 58% of women gain a first or upper second class degree compared to 50% of men
Eighty-four percent of men and 73% of women of employment age are working or available to work. The proportion of women working depends on the age of the woman's youngest child (Table 1). Almost half of female jobs are part-time, and 40% of women with dependent children work part-time compared with 23% of those without children and 5% of men. Roughly, a quarter of female employees do administrative or secretarial work. Men are twice as likely as women to be managers and senior officials and far more likely to be in skilled trades (Fig. 2). Since 1999, women's hourly pay has remained at around 80% of men's pay.
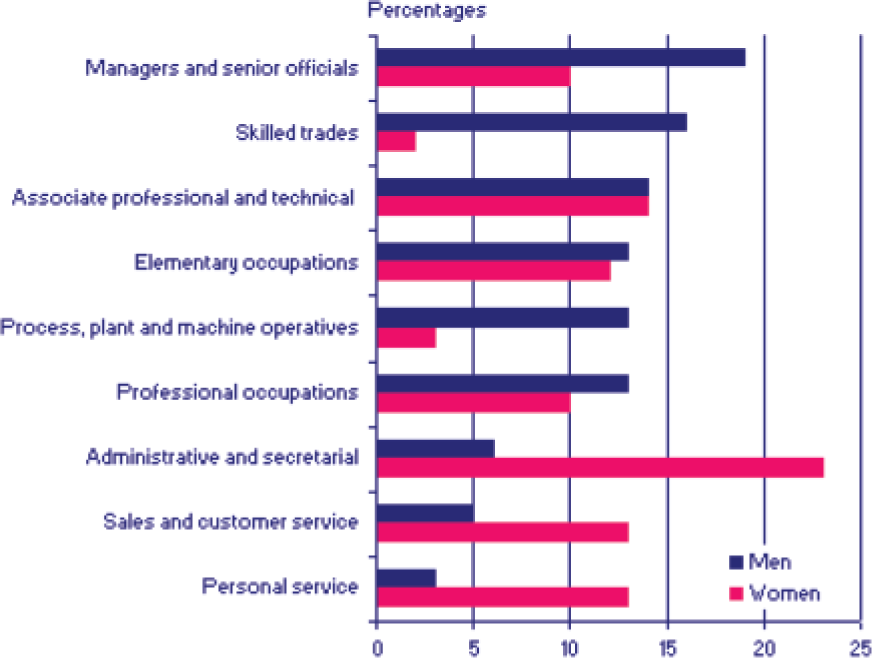
Employees by occupation in the UK in 2003.
Impact of children on employment of women

Deprivation
Social deprivation is related to income and is linearly associated with death and ill health from all causes with no threshold and no upper limit. Patients with low income levels have higher incidence of illness leading to an increased requirement for primary health care services and increased use of out-of-hours and emergency services. The most pronounced effect is with circulatory and other smoking-related disease. A similar trend is seen with infant mortality, morbidity from chronic illness (particularly musculoskeletal, cardiovascular and respiratory conditions) and teenage pregnancy.
This increase in morbidity with increasing social deprivation is not a new problem nor one unique to the UK. Suggestions that it is due to smoking and eating habits may be partly correct but this social disparity was still apparent in evidence collected more than 80 years ago, when those of social classes I and II were more likely to smoke, eat foods high in saturated fats and take less exercise. Gender is relevant when discussing health disparity as a result of income. Women, and particularly unmarried mothers, are overrepresented in the lowest income groups and suffer disproportionate health consequences as a result.
Gender and health
Life expectancy
Girls born in 1901 could expect to live to just 49 years and boys just 44 years. Over recent years, the increase in life expectancy among older adults has been particularly dramatic. By 2004, women aged 65 years could expect to live to the age of 85 years, and projections suggest that this will increase by another 3 years by 2021 (Fig. 3). On average, girls can expect to live 4 years longer than boys, but in recent years this gender disparity in life expectancy has been reducing (Fig. 4).

Life expectancy in England and Wales.

Average life expectancy for males and females, by time period.
The cause of the gender gap in life expectancy between men and women is multifactorial. Genetic factors, endogenous oestrogen (which affords protection against cardiovascular disease and other ageing effects) and different lifestyle and environmental influences all play a role. The reasons for the decreasing gender gap in life expectancy are not entirely clear and may relate to changes in working and lifestyle patterns for both men and women. For example, with increasing mechanization and decline in mining and manufacturing industry, men are less likely to suffer serious accidents or illnesses related to their occupations.
Healthy life expectancy
At all ages, a higher proportion of men than women in the UK report their health to be good. Among both sexes the proportion of people reporting good health declines with age; 41% of men and 38% women aged 60–74 years have an ongoing disability. However, many people in the older age groups still consider themselves to be in good health, even if they have a limiting long-term illness or disability that restricts their daily activity.
There has also been an increase in the number of years that men and women can expect to live free from a disability or limiting long-term illness (up to 69 years for females and 67 years for males). However, these numbers of disability-free years are not proportionate to the life expectancy of men and women and therefore while women on average live longer than men, they also have more years of poor health. Disorders such as arthritis and rheumatism are the most common types of chronic disease in the UK and their prevalence increases with age; women are more likely to suffer these disorders than men.
Causes of death
Circulatory disease (including ischaemic heart disease and stroke) was the most common cause of death in the UK for both males and females until 2006. However, deaths due to circulatory disease have begun to decline and although it remains the most common cause of death in males, in 2006 cancer took over as the most common cause of death in females. Figure 5 illustrates the gender differences in different cancers in the UK. The greater prevalence of circulatory disease and lung, bladder and stomach cancer among men is due in part to biological differences but also results from the historic gender difference in cigarette smoking (which is rapidly changing among younger generations).

Gender differences in common cancers in the UK.
Young men (aged 16–34 years) are more than twice as likely to die as women of the same cohort. The most common causes of death in this age group are suicide and accidents. This may be partly related to greater risk-taking behaviours among men, who are also more often involved in criminal activities, both as victims and as perpetrators. It may also be related to lack of social support for young men.
Lifestyle and health
Both men and women are increasingly exceeding the recommended daily alcohol limit. This is likely to be the cause of the simultaneous increase in the death rate from alcohol-related causes for both sexes. The greatest rate increase has been among men (Fig. 6), which may reflect that men are more likely than women to exceed the recommended daily limits for consumption of alcohol and are also more likely to drink heavily. Binge drinking rates are greatest in the 16–24 year age group for both men and women.
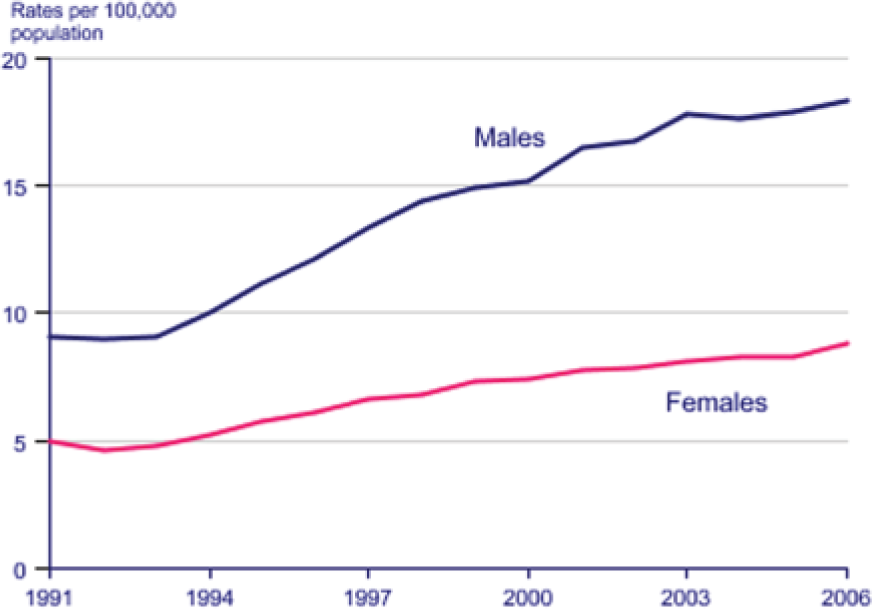
Death rates from alcohol-related causes.
Since the 1970s, the proportion of all people who smoke in Great Britain has fallen. Overall, there remains a higher prevalence of smoking among men than women, but among young adults (aged 16–19 years), more women (26%) smoke than men (23%). Rates of lung cancer deaths reflect smoking behaviour (Fig. 7).
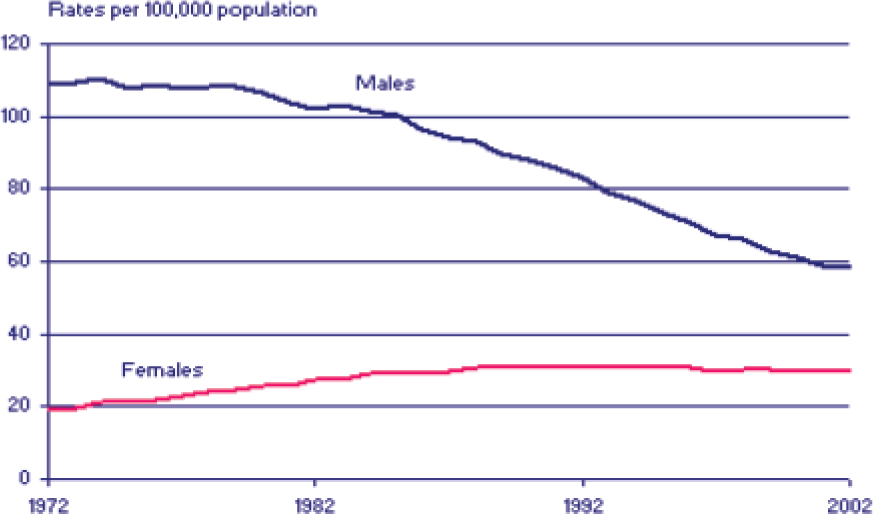
Lung cancer rates in the UK.
Men also have higher rates of substance abuse than women with 13% of men and 7% of women reporting use in 2006/07. Of the individuals reporting drug usage, roughly a third report the use of Class A drugs for both sexes.
Obesity is a significant public health concern. Traditionally, women have been more prone to obesity than men (Fig. 8). However, recently this trend has evened out and in 2005, similar proportions of men and women (23% of men and 25% of women) aged 16 years and over in England were obese with a body mass index (BMI) of 30 or greater. Furthermore, more men than women were classified as overweight having a BMI in the range 25–29 (43% of men and 32% of women).

Prevalence of obesity in adults by gender 1993–2005.
Diet and an increasingly sedentary lifestyle are likely to be causal factors in this changing trend. As a rule, young men eat less healthily than women or older men. In 2006/07 watching television was the most common leisure activity for over 8 of 10 men and women in England. Although men were more likely to perform physical activities, including sport and exercise (58% men compared with 43% of women), this was not at a high enough level to prevent obesity.
Diseases
As well as conditions unique to women such as gynaecological problems and pregnancy, women are more likely to consult than men with autoimmune disease, mental health problems, musculoskeletal symptoms and non-specific symptoms.
Diseases unique to men include prostate disease, testicular disease and problems of erectile dysfunction. However, men are also more likely than women to consult GPs with back problems, personality disorder, drug and alcohol dependence and diabetes.
Inequality within gender groups
Women and men are clearly not homogeneous groups, and inequality in health status exists within subsets of each gender. Some of this may be related to the status and behaviours accorded to a particular gender within a cultural or social group. For instance, within some ethnic minority groups the lower status of women may lead to reluctance to invest time and effort in preventive health measures. Sometimes a combination of biological and gender-related behavioural factors can contribute to health inequality, such as the higher rates of smoking in Bangladeshi males leading to a much greater prevalence of cardiovascular disease in this group.
There are geographical differences too. Women in Scotland suffer extremely poor health, much of which appears to be related to the changing behaviour patterns among young females and social class differences. Scotland has one of the highest levels of smoking and obesity in Western Europe and alcohol consumption in Scotland is increasing. Consequently, rates of oesophageal cancer, lung cancer, ischaemic heart disease and alcoholic cirrhosis among women are all rising.
Gender and the GP consultation
Except among the very young and very elderly, females are more likely than males to consult a GP (Fig. 9) with a ratio of number of National Health Service (NHS) GP consultations each year of 5:3. Some of this increased usage is predictable. In one study, 60% of the sex difference in consultation rates was accounted for by the increased number of appointments women made for screening (e.g. cervical smear testing), obstetric or genitourinary problems such as contraception (Stoverinck et al., 1996).

Overall consultation rates by age and sex in England in 1995 and 2008 using QResearch.
Other more subtle and complex factors may explain the remaining disparity. Familiarity with health care services as a result of contact for routine screening, contraceptive services or pregnancy may increase access. For example, it is common for a woman to mention another health problem in passing when she comes for a smear test or routine pill check. Women are also less likely to work and more likely to work part- rather than full-time. Routine health care services have traditionally been provided within routine working hours, and this may have made them more accessible to women than men.
Men are often reluctant to seek help until they are convinced that they have a significant problem as they do not want to waste the doctor's time, or they feel it is not very masculine to discuss health problems (McVittie and Willock, 2006). Male consultation rates appear to be associated with marital status, and self-reported health status with widowed and divorced men having the lowest self-reported health and highest consultation rates.
Gender and patient behaviour
GP receptionists often receive requests from patients to see a GP of a particular gender. This may be because the patient thinks the consultation may require an intimate examination but is not always so. Preferences may also be linked to patient expectations of the response that they will receive from the doctor. The expectation is that female GPs are more supportive and empathetic, while male GPs are more authoritative (Roter et al., 2002). Supporting this hypothesis, primary care studies have shown that women GPs tend to have very different caseloads from male GPs because female patients chose to see female GPs and expect a different communication style (WONCA Working Party on Women and Family Medicine (WWPWFM), 2008).
Additionally, the behaviour of patients during consultations differs according to gender. This may also relate to patient expectations. If patients expect a female GP to be more supportive and empathic, they may disclose more personal information; if patients do not regard a female GP with such authority, they may be more likely to challenge the GP's opinion. There is evidence that patients are more assertive with female GPs and interrupt them more (Kilminster et al., 2007). Additionally, a gendered difference in patient communication styles is also well documented. Men are generally less articulate about their health than women.
Finally, the construct of gender is different in different cultures: what is acceptable for a man or woman in one culture will differ for that of another. For example, in some cultures it may not be acceptable for a man to admit that he feels depressed and this will affect the way that he articulates his problems to his GP. GPs must be aware of potential hidden agendas.
Discrimination, equality and equity
Discrimination
Discrimination is defined as unfair treatment of a person or group of persons on the basis of prejudice. In 1975, the Sex Discrimination Act was passed and discrimination in the provision of facilities and services on the basis of gender became unlawful. This includes discrimination in the provision of primary health care services.
Equity or equality?
The equal provision of services for groups of people does not necessarily equate to the equitable provision of services to these people. Equity requires service provision in accordance with need.
To take the example of gender equity and public toilets:
Equality is the provision of equal numbers of toilet cubicles in public toilets for men and for women.
Equity is the recognition that due to aspects of their gender women require more time than men in the bathroom (having to disrobe and managing menstrual periods for example), and therefore the provision of more cubicles in public toilets for women than for men.
In addition to not discriminating on the basis of gender, a successful health service should also be gender equitable or cater in equal measures for the specific needs of both male and female populations.
Providing a gender-equitable service
To tackle rising levels of teenage referrals to specialist mental health services, the Primary Care Trust (PCT) has started a counselling service for teenagers. To test this out, a pilot scheme is started in three GP practices with health visitor support to provide general health information and health promotion advice. The service is advertised with leaflets placed in practices, local youth groups and schools.
Three months into operation, the new service is audited. Of note, three times more girls have been seen than boys. Although a gender disparity had been expected, the number of boys seen is disappointing, particularly as national statistics suggest that many boys suffer mental ill health and young men have a high suicide rate.
At a meeting to discuss the results, reasons for this disparity are sought. Several possible reasons are proposed:
Venue—Girls tend to visit GP practices more often for reasons such as family planning, so are more likely be familiar with the practice environment, and thus find it less intimidating
Marketing—The leaflet advertising the service has a picture of a girl chatting to a female counsellor on the front. Girls may identify with this image more than boys.
Gender of the counsellor—A single female counsellor had been employed to provide the counselling service, and the health visitor is also female. This leaves boys no option but to see a counsellor of a different gender.
After some juggling of staff, the service is made more gender equitable. Weekly sessions are alternated between a male and female counsellor, and additional sessions are provided in the local youth centre. Promotional leaflets are altered so that there is a picture of a happy looking boy and girl on the front cover. The information inside is updated to include information about choice of gender of counsellor.
A further audit 3 months later showed that more boys were using the service, to the extent that overall more boys than girls were seen at the youth centre sessions. By making the counselling more gender equitable, the PCT had been able to provide a more effective service.
What can we do as GPs?
Recognizing the role played by gender in health, health-seeking behaviour and the consultation is important as it influences the manner in which GPs and NHS organizations should provide their services.
At practice level
Some of the key implications for practice if a service is to be provided in an equitable fashion include providing access to appointments with a same-sex GP if this is preferred by the patient. For example, practices may wish to provide patients with information about the gender of GPs or nurses, with receptionists offering a choice of who the patient wishes to see. This is also likely to provide a more effective consultation.
Within the consultation itself GPs should maintain awareness of the gendered differences in patient communication styles. For example, men are less able to articulate health problems than women. GPs may wish to adopt communication strategies to allow for this.
It is also helpful for GPs to be aware of the gendered pattern of health and disease as this assists in the diagnostic process. For example, if a man presents with chronic breathlessness, ask what his occupation was. Has he been exposed to asbestos in the course of his work? If a man presents with erectile dysfunction, does he have cardiovascular disease or diabetes? If a young woman presents with obesity and further questioning reveals period problems or hirsutism, does she have polycystic ovarian syndrome?
Gender-specific consultation patterns are important for health promotion as well as diagnosis of disease. As men consult less often, it is important to make the most of each consultation, and particularly not to forget health promotion, for instance by opportunistically checking blood pressure or provision of leaflets on testicular self-examination or prostate-specific antigen testing. Consultations with women are useful platforms for promotion of women's health initiatives such as the UK breast screening or cervical cancer screening programmes.
It is also important to ensure that services provided do not discriminate against one gender. One example is informal carers. More informal carers are female than male. Carers tend to neglect their own health for a variety of reasons, including difficulties with access to health care services for their own health problems. If a patient is a carer, consider providing home visits, appointments at times when substitute care is available or appointments to coincide with appointments for the cared for. Another example is that of full-time workers. More full-time workers are male than female. Consider offering early morning, later evening or weekend appointments for workers unable to get the surgery during normal working hours.
At an organizational level
GPs have influence beyond their own practices. This can be at local level (e.g. through commissioning groups, Primary Care or Hospital Trusts, Local Medical Committees, University Departments or Deaneries), at national level (e.g. via the Royal College of GPs, General Practitioner Committee or Department of Health) or internationally (e.g. through representation on World Health Organization or European Union bodies or the World Organization of Family Doctors). In these positions, GPs have important roles as advocates for gender equity.
One such example is the World Organization of Family Doctors (WONCA) Working Party on Women and Family Medicine (WWPWFM). The WWPWFM is a group of primary care practitioners who seek to promote recognition of the significant impact that gender has on health. In 2006, the WWPWFM were successful in developing recommendations on how to achieve and maintain gender equity within their own organization and more widely (Box 2). These steps to gender equity in health provide a useful framework for GPs to work from when influencing policy decisions and service development.
Ten steps to gender equity in health
Strive for gender equity in access to health services
Work in all initiatives toward the elimination of gender-based violence
Uphold the right of women to reproductive choice and safe motherhood
Assert the right of women to safe sex and sexual choice
Advocate for women's active participation in decision making and equitable distribution of resources (health services, income, education, housing, etc.)
Integrate gender perspectives into medical curricula and education, residency training, professional development and patient care throughout the life cycle
Promote the integration and understanding of healthy human sexuality in medical curricula and education, residency training, professional development and patient care throughout the life cycle
Promote and support research on the impact of gender on health
Encourage those individuals and groups with special interests in issues, such as tobacco cessation and alcohol and drug misuse, to incorporate a gender perspective
Recognize that women's empowerment is a key factor in human immunodeficiency virus (HIV)/acquired immune deficiency syndrome (AIDS) and take concrete action toward addressing this worldwide catastrophe
Finally, GPs who also work as researchers, educators or academics can act to improve gender equity through increasing gender awareness in their field of work. Historically, medical research has been gender biased: most medical knowledge is based on research into male health and illness. As a result, erroneous assumptions have been made about the similarities and differences between men and women and gender stereotypes have been accepted. Such institutional bias is passed on to junior researchers and medical students. However, by explicitly acknowledging the role of gender inequalities in health and disease and aiming for gender equity, researchers and academics can start to change this systematic perspective. Through mainstreaming gender into the medical curriculum, educators can help to shape a more gender-equitable future.
Key points
There is an important distinction between biological sex and the social construction of gender: this influences experience of health and disease
Gender is a strong determinant of experience within society, for example, a woman is more likely to be a lone parent than a man
Biological sex affects the likelihood of an individual experiencing some illnesses that are sex specific and also contributes to physical differences which mean women tend to live longer than men. However, gender (including lifestyle factors) has a larger role to play in differential prevalence of illnesses among men and women.
Gender affects health-seeking behaviours and also the behaviour of individuals within the consultation. Women may be more likely to use health care services and are more articulate regarding their health problems.
GPs have a duty to avoid gender discrimination when providing services and therefore must be sensitive to the health needs and behaviours of individuals according to gender
To achieve the goal of gender equity in health care, GPs should strive to mainstream gender issues into their workplace and more widely, particularly as policymakers and educators