
Abstract
The differing status of men and women in a society affects their experience both as patients and as providers of health care. This article examines the influence gender issues have upon the role of doctors and the running of health care services in an increasingly feminized workforce. It aims to raise awareness of the medicolegal aspects involved, including opportunities for GPs to improve gender equity in the workplace.
The GP curriculum and the gender of GPs
Treat colleagues equitably and with respect
Act in ways that recognize that people are different and do not discriminate against people because of those differences
Challenge behaviour that infringes the rights of others
Recognize and take action to address discrimination and oppression in self and others
Act in ways compliant with employer law, disability discrimination legislation and best practice in recruitment: encourage others to do so
Interpret people's rights in a way consistent with employer's policies and relevant professional standards
The changing face of general practice
Over the past four decades in the UK, the proportion of women in employment has grown markedly. At the start of 1971, the employment rate for women was 56% compared with 70% in 2008. By contrast, there has been a similarsized decrease in the employment rate for men, with the male employment rate falling from 92 to 78%.
Paralleling national employment trends, the last four decades have seen a significant shift in the gender composition of entrants to medical training. In 1960, only 24% of medical students were female; today this figure is 57% (Department of Health, 2009). As a result of the increased number of medical student places, twice as many men are entering medical school as did in 1960, but 10 times the number of women (Fig. 1).
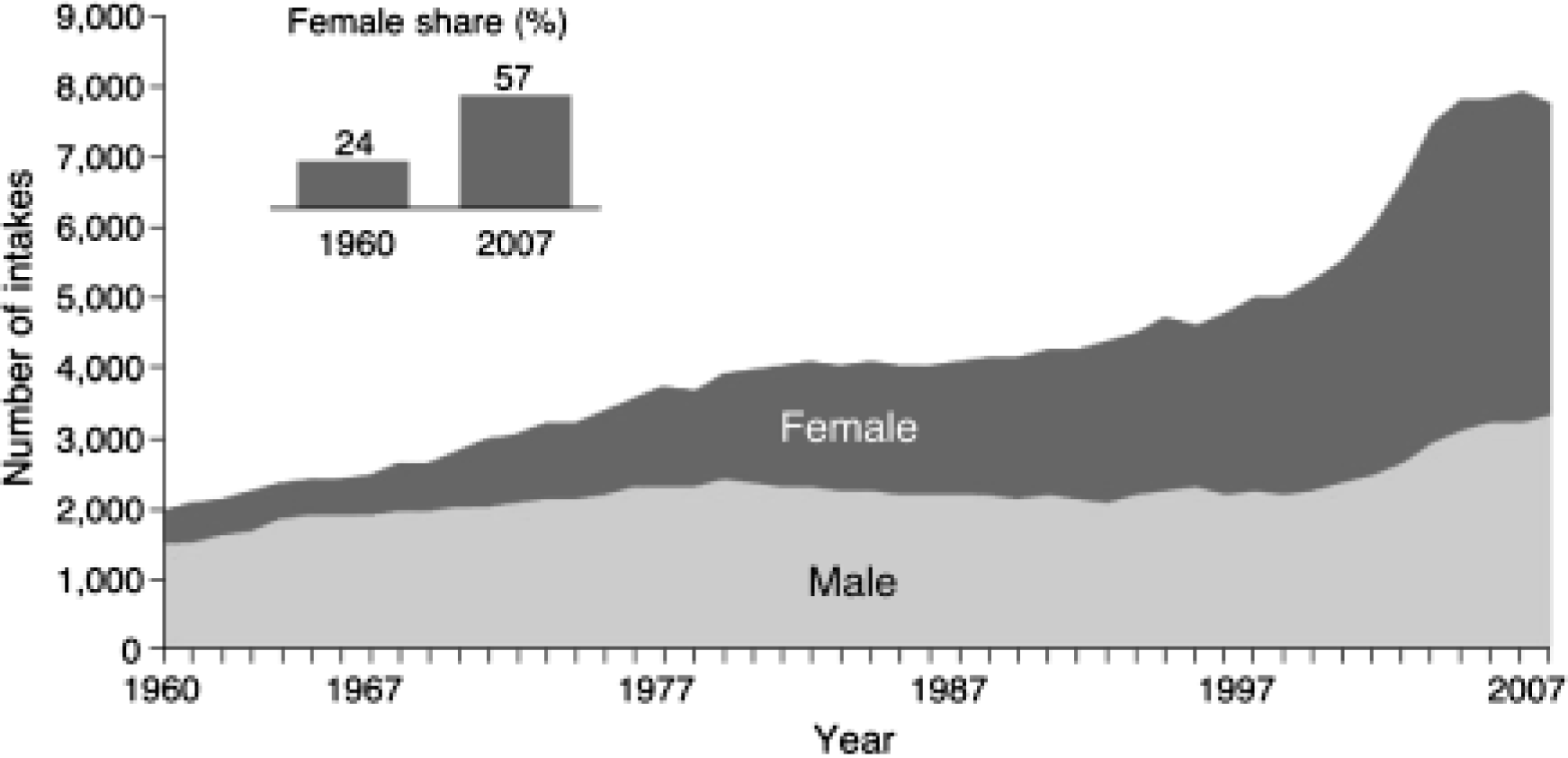
Male and female intake into UK medical schools (1960-2007).
The increasingly large numbers of women entering medical training in the UK are beginning to be reflected in the composition of the medical workforce. However, in the past, this has been moderated by the influx of significant numbers of international medical graduates who were more often male. Women now make up 40% of all doctors and 28% of all consultants, but only 9% of surgeons (NHS Information Centre for Health and Social Care, 2009a).
General practice is the most popular specialty for female doctors. Female GPs comprised 32% of practitioners in 1998 and 43% in 2008 (Fig. 2). On present trends, female GPs will form the majority as soon as 2013, and more than half of all doctors will be female by 2017.
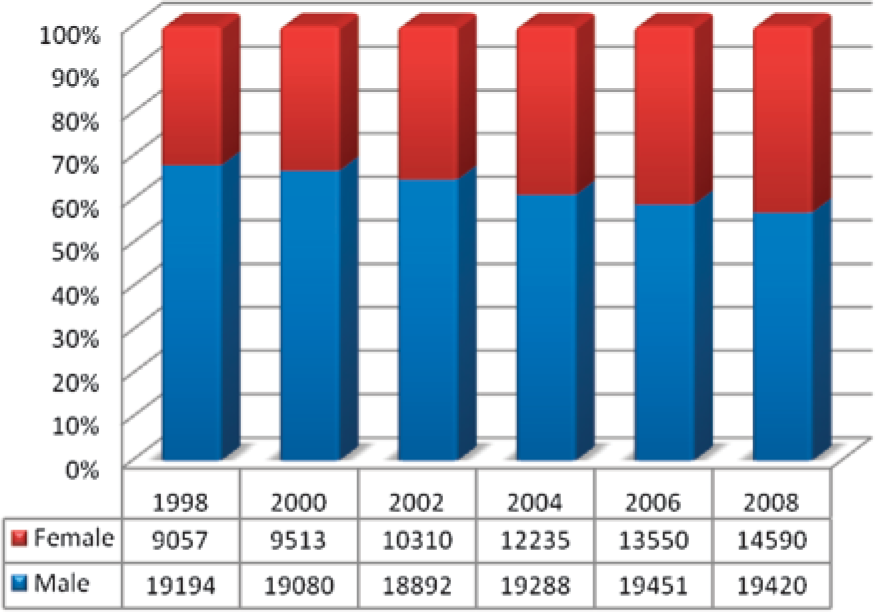
GPs by gender 1998–2008.
The popularity of general practice as a career choice for women doctors is not fully understood. Possible explanations include
A gendered expectation that general practice is a specialty in which women's relational and empathic skills are valued
Junior doctors' experiences while learning
Positive female career role models from general practice
A view among female junior doctors that general practice is a specialty with more flexible working hours that are perhaps easier to plan and in which there are job opportunities for women.
Hours of work
Although there are more women workers, women do not necessarily do a larger share of the workload. The high numbers of female part-time workers mean that work is not shared proportionately. In 2008, over half of women's jobs were part-time compared with one in six men's jobs.
In primary care too, women account for almost three-quarters of those doctors who practice on a part-time basis. Nearly half (49%) of all women GPs—as opposed to 12% of male GPs—have part-time working arrangements (RCGP, 2006). Therefore, male GPs carry a higher proportion of the workload than their numbers might suggest.
Reasons for part-time working
It is oversimplistic to make broad assumptions about parttime workers. Within this group, there is a great deal of heterogeneity in numbers of hours worked: some GPs may only work two or three sessions a week, others may work eight sessions a week and still be labelled part-time. Many GPs also have portfolio careers. They work a limited number of sessions each week in general practice, and thus are classed as part-time, but perform other jobs the rest of their working week. Examples include GPs who work as clinical assistants, GPs with special interest or those with industrial, academic or managerial responsibilities.
One likely reason behind women's preferences to work part-time is the disproportionate responsibility that they have for childcare. A self-report survey of English GPs (Gravelle and Hole, 2007) found that on average both full- and part-time female GPs worked fewer hours than their male colleagues. This differential was entirely accounted for by family circumstances: the negative impact of having children on hours worked was twice as large for female GPs. Once this effect was allowed for there was no significant difference between genders in hours worked.
It might be expected that female GPs who stop working or reduce their hours when child rearing will later return to longer working hours. However, this is often not the case. Many women never return to full-time working, as the partnership structure of general practice does not lend itself to easy changes in working hours. The opportunity to go back to full-time working may not be available in the GP's practice at the time that she is ready to increase her hours. Furthermore, other responsibilities, such as care for elderly relatives and care for the home, compete for the time of women GPs who work part-time and take over prominence once childcare is no longer an issue.
It is also a fallacy to suggest that just women GPs wish to work part-time. A recent longitudinal study of doctors' careers (Jones and Fisher, 2006) found that significant numbers of both male and female GPs choose to work reduced hours. Doctors of both genders who move to general practice from other career preferences do so because of better hours and working conditions, and many either work part-time or are considering doing so. This challenges the assumption that the preference for part-time working is driven by the childcare responsibilities of women. Men as well as women may demand greater flexibility in working hours in future to allow time for both family commitments and for them to pursue other activities.
Partner or salaried?
Over the past decade, an increasing number of women have joined practices as partners, altering the gender composition of practices (Fig. 3). In 2006, 63% of GP partners were male, 37% were female (Elston, 2009). However, this figure is not as high as might be expected given the significantly greater proportion of GPs who are now female.
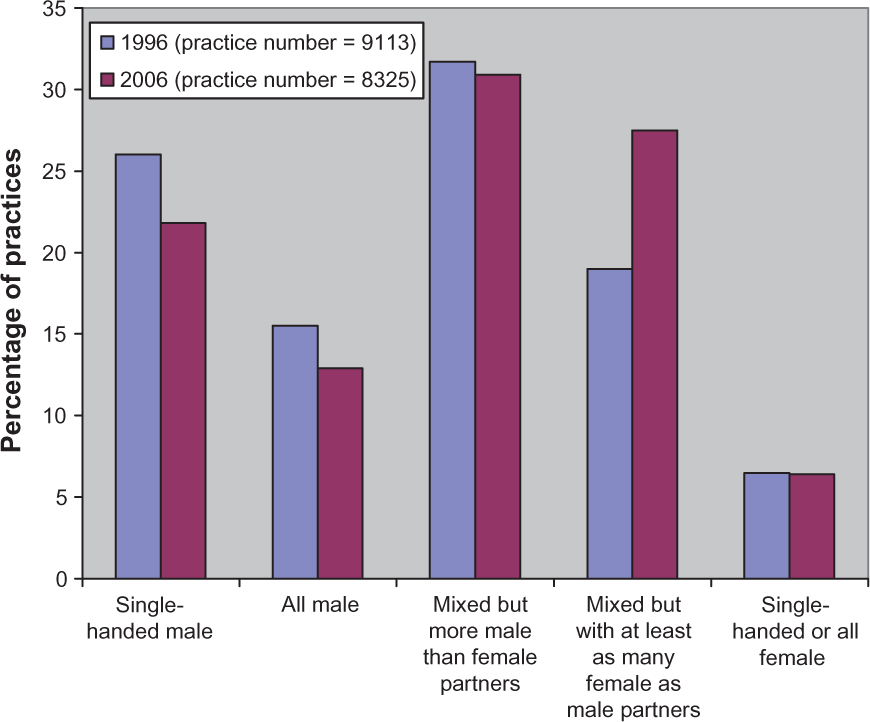
NHS practices in England, by gender composition of partnership in 1996 and 2006.
In a 2008 study of salaried GPs, women were almost twice as likely to be salaried as men (Ding et al., 2008). There is a strong association between salaried status and working part-time: 64% of salaried GPs work part-time.
It may be that the advantages of salaried and part-time work appeal more to female GPs, particularly younger women who are new entrants to general practice and who may be more likely to have young children. Such advantages include a more stable income, more ease in relocating, paid maternity and sick leave, fewer management responsibilities, fewer practice-related commitments outside usual working hours and no financial stake or risk in practice ownership. However, many of these factors could also be attractive for younger men embarking on their general practice careers, and the larger numbers of women GPs in salaried posts may simply reflect the difficulties that women face obtaining partnerships.
There are also disadvantages in salaried working for GPs— lower income, perceived lower status, less job security and lack of career development opportunities. These may create inequity between male and female GPs. For example, the average annual net profit for a GP partner in a non-dispensing practice in 2006 was £106 681, but the average pretax earnings from all sources of income of a salaried GP was £46 905 (NHS Information Centre for Health and Social Care, 2008).
Workflow and consultation styles
The workflow of GPs varies according to gender. Women doctors' duties more often involve caring for women's health, contraception and antenatal care. Despite the greater psychosocial focus that women GPs generally have, women doctors are no more likely to see patients with psychiatric diagnoses (Franks and Bertakis, 2003).
In general, woman GPs tend to have longer consultations with their patients. Despite this, there is no evidence that they see fewer patients than their male counterparts working the same hours. Instead, they tend to put in more of their own time to compensate. This difference may be partly because female GPs are more likely to perform time-consuming examinations such as antenatal checks, breast and pelvic examinations. However, even adjusting for case mix, women GPs still have a slower consultation rate, probably resulting from different consultation style (Roter et al., 2002).
Although there is no strong quantitative evidence for claims that women doctors have better communication skills, a large body of qualitative literature has identified that, in general, women doctors:
Are more patient centred
Are more empathic
Show more partnership behaviours
Engage in more positive talk and emotionally focused talk
Ask more psychosocial questions and counsel more psychosocially
Are more prevention oriented in their behaviour
Are more likely to refer or follow-up their patients
Female GPs derive more satisfaction than their male counterparts from relationships with patients (Chambers and Campbell, 1996). However, they may be less good than men at skills such as saying no, keeping tight boundaries and being clear on lines of professional responsibility (Howe, 2007).
Although there are very many notable exceptions, in general male doctors are more distant, authoritative, give more commands to patients, interrupt more and are more presumptuous (Kilminster et al., 2007). Their consultations, perhaps as a consequence, tend to be shorter. Male GPs are considered to be more efficient than female GPs (Bloor et al., 2008) and tend to prefer organizational aspects of care (Chambers and Campbell, 1996).
Some authors argue that female GPs need to be more efficient and develop a stronger ability to live with risk. However, effective communication and patient-centred care tends to result in better outcomes and qualitative benefits, which might offset any alleged inefficiencies from longer consultations. Moreover, longer consultations result in fewer missed diagnoses and less litigation. Significantly, more male doctors are referred to the National Clinical Assessment Service, and satisfaction surveys show that patients in general are more satisfied with women doctors.
Leadership roles
Across the National Health Service (NHS), and indeed internationally, women fill fewer leadership positions than men. For example, they are underrepresented on NHS Trust Boards and professional executive committees for Primary Care Trusts. In 2007, only 12% of all university clinical professors, and in the preceding year, only two of 34 medical school deans, were women. One exception to this is the Royal College of General Practitioners (RCGP) which has good representation of women among its officers, including the current president of the RCGP who is female.
There is no evidence to suggest that this underrepresentation in leadership roles is due to lower academic ability of women: if anything, females tend to outperform males in academic examinations right up to MRCGP level. Studies have also shown that women are good at empowering others and are good team leaders (Eagly and Johnson, 1990), so their lack of advancement is not due to poor leadership skills.
It is likely that the current situation is influenced by the experiences of female GPs at practice level, where they are more likely to be working part-time and as salaried employees, and they are less likely to be involved in leadership and management roles. A survey of Scottish GPs (McKinstry et al., 2006) found that male GP principals claimed to spend an average of 18% more time providing patient services activities and 50% more time on professional activities such as training and practice management than women. Lack of leadership experience at practice level may constrain women's ability to become involved in leadership beyond the practice. The increased proportion of female medical students, associates in training and younger GPs may mean that women GPs will assume more leadership roles as time goes on, but systemic factors limiting the progression of women into these roles must be addressed for this to happen.
Career constraints
There are a number of reasons why both female and male doctors may feel that their career is constrained by gender. Beginning at medical school, gender may directly constrain experience. For example, male medical students describe having fewer opportunities to learn gynecological examination (Higham and Steer, 2004).
However, often the influence of gender is much more subtle with gender stereotypes and gendered values being passed on in the course of everyday teaching and practice. The predominance of men in senior educational, academic and hospital consultant posts may be partly to blame for this. Specialties in which there are more female leaders attract more female trainees who go on to move into higher positions. Lack of career advice, poor mentoring and paucity of female gendered role models are all recognized as institutional barriers for women in medicine.
It may be that when women are in a minority they are less well integrated and less able to alter the organizational structure to favour female trainees coming through behind them. For example, in general practice, even now, most practices have a majority of male partners. Within a practice, a majority male view can influence practice decision making and the way in which practices plan for the future. This in turn can lead to active discrimination to ensure the appointment of new male partners, with positions holding lesser status being offered to women, thereby perpetuating gender career constraints for women.
Finally, in all areas of medicine, women are disproportionately constrained by family ties. They remain the traditional child caregivers, even in families in which both partners have a career. They are forced to choose between career and family, often opting for flexible working patterns with lower status and fewer opportunities to progress in order to accommodate family commitments. This constraint is exacerbated by institutional limitations such as lack of flexibility in rotas, low acceptance of career breaks, paucity of part-time working opportunities and a lack of childcare facilities which are acceptable and accessible—ideally in the workplace. All these factors combine to produce a glass-ceiling effect for many female doctors.
Discrimination: the legal position
Discrimination is defined as unfair treatment of a person or group of persons on the basis of prejudice. In 1975, the Sex Discrimination Act was passed, the Equal Pay Act came into force and the Equal Opportunities Commission (subsequently replaced by the Equality and Human Rights Commission) was set up as the organization to promote, monitor and enforce these two pieces of legislation and promote equality on the basis of gender in the UK. Under the terms of this legislation, discrimination (both direct and indirect), victimization and harassment on the basis of gender are all illegal.
Since then, men and women have become more alike in the way that they balance work and home, increasingly sharing earning and caring responsibilities. But the gender divide has not gone away and issues of gender discrimination are commonplace.
Discrimination law is complex and constantly changing. The major pieces of legislation that you should be aware of are summarized in Table 1. Specialist legal advice is always advisable.
Current equality legislation in the UK

Direct discrimination
Direct discrimination occurs when a person is treated less favourably on the grounds of a particular characteristic, such as gender. Direct discrimination is usually fairly easy to spot.
Example 1
In the Bankwood practice, six candidates are short-listed for a GP Partner post. One of the female candidates, Dr A, clearly meets the requirements of the job specification better than any of the other candidates but is rejected in favour of one of the male applicants on the basis that she has just got married and thus would be likely to take maternity leave in the near future.
Indirect discrimination
Indirect discrimination occurs when an unjustifiable rule or requirement is applied to everyone but has a disproportionately adverse impact on a group with a particular characteristic such as gender. This is often harder to detect than direct discrimination.
Example 2
The Chestnut practice has just one female partner. Dr B came to the practice straight from GP training and until now has worked full-time. After the birth of her first child, she asks the partnership if she might drop her hours to part-time. Even though she is prepared to share her office with another GP, and happy to be flexible about the way in which she works part-time, her request is denied on the basis that no one else works in the practice part-time and she was appointed to a full-time post.
This is indirect discrimination as no justifiable reason has been given for Dr B's request to be denied. Lack of opportunity to work part-time is more likely to adversely affect women GPs than men as women have traditionally shouldered the role of childcare within the home.
Victimization
Victimization occurs when a person is treated less favourably because they have asserted their rights under equality legislation.
Example 3
Dr B was forced to leave the Chestnut practice after her request for part-time working was turned down. After taking legal advice, she took a successful discrimination case against the practice to an industrial tribunal. However, when she came to apply for other GP posts in the area, she was told repeatedly that she was unappointable because of the actions that she had taken.
Harassment
Harassment arises when the conduct of one person has the effect of violating another person's dignity or creating an environment which is intimidating, hostile, degrading or humiliating.
Example 4
Dr C is a male GP who has dropped his hours to parttime to share the childcaring responsibilities with his wife, who is also a GP and works in another local practice. His colleagues within the practice continuously tease and joke about his part-time status and role as house-husband and are hostile toward him because he does not take on as many of the managerial duties within the practice as his full-time male colleagues.
Discrimination and the duties of a doctor
The General Medical Council (GMC) guidance Good medical practice (2006) includes a requirement for doctors never to discriminate unfairly against either their patients or their colleagues, including for reasons of gender. It is also advised that doctors should challenge any colleagues whose behaviour does not comply with this guidance. This advice is reiterated in the RCGP guidance Good medical practice for general practitioners (2008), which also sets out some examples of good practice, for example, facilitating patient preference to see a doctor or nurse of a particular gender.
Implications for practices and workforce planning
‘We should make our goal a profession where every woman and man goes as far as they wish and as far as their talents permit.’ Baroness Deech, 2009.
In 2009, Baroness Deech published her report: Women doctors: making a difference. This report looked at the obstacles to the full exercise of every doctor's potential — from the decision at school to study medicine, through training, work, maternity leave, childcare, progress through the profession to leadership, retirement and pensions—with special emphasis on the choices and problems that women face. Her recommendations fall into three main areas:
improving the existing structures so that there is better advancement to crucial career turning points as well as different ways of working
ensuring that new processes such as revalidation have the flexibility and capacity to accommodate doctors who may not be conforming to the usual working patterns and
providing additional support for the practical realities of caring for a child or a dependent relative
GPs as partners
GP partners responsible for the day-to-day running of practices must ensure that they do not discriminate on the basis of gender against their own partners, their employees or their patients. Appointments to GP partnerships are in short supply at the moment in the UK. Recent evidence suggests that, despite more women than men completing GP training, and most practices having more male than female partners, women applying for partnership positions are less likely than men to be appointed as partners. This suggests implicit discrimination.
When advertising GP partnership posts, it is important that practices formulate clear job descriptions with transparent criteria for selection. Those applicants that meet the criteria best—whether male or female—should be invited for interview. During the interview process, female candidates must not be asked gender-specific questions that might disadvantage their application. For example, it is not acceptable to ask either male or female candidates about future plans for parenthood. The successful candidate should be selected on the basis of aptitude and best suitability for the post, and practices must be able to justify those reasons for selection.
Within partnerships, it is also important to ensure that female partners are offered the same opportunities as male partners. For example, it is not acceptable to allow a male partner to have a period of sabbatical leave but exclude a female partner from having sabbatical leave because she has had time-out for maternity leave.
GP partners are also employers. They employ salaried GPs and practice staff. It is the partners' responsibility to ensure that each practice has a written equality and diversity policy in place. This policy should apply to all employed staff whatever their roles. The Arbitration and Conciliation Advisory Service (ACAS) produces a booklet (‘Delivering equality and diversity’) giving step-by-step guidance on how to do this which can be downloaded from their website (www.acas.org.uk). Further advice can also be obtained from the British Medical Association (BMA).
Finally, in provision of primary care services, it is important that partners ensure that services are equally accessible to both male and female patients. As health service needs are not the same for these groups, gender equity should be the aim. The service should cater in equal measures for the specific needs of both male and female patients. For example, this might include providing late appointments for full-time workers (who tend to be male) or home visiting services for full-time informal carers (who tend to be female) who cannot get to the surgery to attend to their own health needs.
GPs as employees
Salaried GPs are an increasingly large group of doctors; the majority are women. In recent months, there have been reports of a ‘split’ in general practice with some salaried GPs wanting their own representation (Sands, 2009). Salaried GPs suffer from perceived lower status than their GP partner colleagues despite an equal level of training and very similar working roles and responsibilities. They also have significantly lower hourly pay together with fewer opportunities to pursue extended roles. Contracts vary greatly from practice to practice in terms of both conditions of employment and pay. Many salaried GPs earn considerably lower amounts than the BMA recommended rate and do not get the recommended uplifts for seniority (Middlemiss, 2009) and very few primary care organizations enforce the General Medical Services (GMS) contract stipulation that GMS practices must employ salaried GPs under terms that are no less favourable than those of the BMA model contract (Praites, 2008a).
Lack of career development opportunities, and perceived inequalities with their colleagues who are partners, cause dissatisfaction and reduce motivation. This in turn may result in poorer performance and patient care and even ill-health. Career limitation is a frequently quoted reason for salaried GPs to leave the profession (Praites, 2008b) and may be seen as an indirect form of discrimination.
As with all jobs, it is important to have a defined job description. Salaried GPs may relish the opportunity to take on additional roles. However, unlike partners who receive a share of practice income whatever they do, making an assumption that they will be performing equal administrative and leadership roles within the practice, salaried GPs tend to be paid less money with the assumption that they will not be taking on any of these roles. Therefore, it is important to ensure that any additional work or responsibilities are reflected in alterations to both the salaried GP's job description and pay.
Workforce planning
In general practice, we are currently facing the prospect of an increasingly feminized workforce as a large influx of female medical students progress through their medical careers. At the same time, traditional models of provision of primary care services are being challenged from all sides. Workforce redesign will be required to enable women doctors to be utilized in an effective and productive manner and male doctors to have equitable access to flexible career opportunities. This should consider the following factors:
Higher proportions of part-time workers—as full-time male GPs retire, there may be a shortfall in primary care provision. Planning a workforce that consists of a larger number of part-time workers brings both organizational and economic challenges. For example, maintaining continuity of care may become more difficult as may access to any particular doctor.
Gender-specific constraints—within the general practice, workforce men often express unmet desires to reduce their working hours but find it difficult to do so because of institutional and peer expectations, while women feel unable to fulfill their potential both as clinicians and as leaders due to professional constraints.
Patient choice—preferably patients should have a choice about whether they see a male or female doctor, particularly when consulting about gender-specific issues.
Different consultation patterns—women doctors may require longer consultation times and be less efficient. On the other hand, costs of poor performance and litigation are less.
Public authorities, practices and employers have a duty to avoid discrimination on the grounds of gender. Alongside making plans for the future workforce, additional opportunities for role extension should be made equitable for both genders. These opportunities give doctors role satisfaction, career advancement and often are recognized outside their own practices. For example, evening meetings of Commissioning Groups may save practice time but are unlikely to be attended by female GPs with childcare responsibilities. Failure to address the issues that constrain female GPs from pursuing leadership and other extended roles not only demotivates the female workforce but is also a form of indirect discrimination.
With electronic communication and increased use of teleconferencing and e-communication, administrative roles may become easier. Electronic communication also makes some academic opportunities more accessible to women. For example, anyone can write an article for InnovAiT or author an e-GP module. The task can be broken down to fit around both general practice and home commitments. However, major academic funding bodies still have very limited options on part-time funding for research.
Finally, as women GPs become the majority, it is important that we face the issues of discrimination against women that are still inherent in the profession. Some GPs advocate addressing this by positively discriminating against women entering medical school thereby restoring the traditional balance (McKinstry, 2008). However, this view makes the assumption that male-dominated medicine is somehow ‘better’. There is absolutely no evidence for that. Nursing is a female-dominated profession, and many nurses successfully juggle fulfilling careers with their traditional family commitments. The arguments about poor continuity and lack of application that are often levelled at female doctors have been overcome in the nursing profession, and there is no reason why the same should not become true in medicine.
An alternative approach is to embrace the change and build systems into every practice and primary care organization to ensure that both men and women GPs are supported to work to their maximum potential as clinicians, administrators and leaders. This will ensure that general practice benefits fully from the gender-specific skills that both men and women have and will lead the way for other specialties to follow.
Key points
An increasing proportion of medical trainees and new entrants to general practice are female
The burden of childcare responsibilities falls disproportionately upon women doctors and this is a significant factor that guides women's career pathways and desired working patterns
General practice is a popular choice for female doctors, but women are still underrepresented as GP partners and in leadership and academic roles
Female and male GPs work different hours, see different caseloads and have different consultation styles, which may all affect service delivery
Discrimination is unfair treatment on the basis of prejudice: GPs have an ethical and legal duty to avoid gender discrimination in their roles as partners, employers and policy-makers
For an effective general practice workforce, it is important to support both male and female GPs to work to their maximum potential as clinicians, administrators and leaders