
Abstract
Constipation affects about 15–20% of the population in the UK. It tends to cause problems at the extremes of age and women are more commonly affected than men. Constipation is associated with irritable bowel syndrome (IBS) in 59%, pelvic floor dysfunction in 29% and slow transit in 13%. Many people manage their constipation themselves with diet or over-the-counter medication. This article aims to provide a strategy for GPs to manage those with more severe symptoms who present to general practice.
The GP curriculum and constipation
GP
Manage primary contact with patients who have a digestive problem
Understand the principles of treatment for common conditions managed largely in primary care, such as constipation
Recognize that some patients may find digestive problems embarrassing to discuss openly and adopt a non-judgemental, caring and professional approach towards patients with digestive problems
Recognize the effects psychological stress can have on the gastrointestinal tract, especially with functional disorders
Recognize and respond urgently to red flag symptoms
Advise patients regarding lifestyle interventions that have an impact on gastrointestinal health, such as advice on diet and on stress reduction
Demonstrate an understanding of national guidelines that influence health care provision for digestive problems
Definition of constipation
The term constipation has different meanings to different people. When asked what constipation is, the most common responses from patients are:
Straining needed to pass stool (52%)
Hard stools (44%)
Inability to pass stool (34%)
In an effort to standardize the concept of constipation for clinical research purposes, the Rome criteria were developed by a panel of experts in 1992. Box 1 summarizes the revised version of these (the Rome II Criteria). It is important to note, however, that only a small proportion of patients presenting to primary care with constipation meet these criteria.
The Rome II Criteria
Two or more of the following symptoms for at least 3 months (which need not to be consecutive) in the past year:
Straining at more than one in four defecations
Lumpy or hard stools with more than one in four defecations
Sensation of incomplete evacuation with more than one in four defecations
Sensation of anorectal obstruction or blockage with more than one in four defecations
Manual manoeuvres to facilitate evacuation with more than one in four defecations (e.g. digital evacuation or support of the pelvic floor)
Less than three defecations per week
Pathophysiology and causes of constipation
In the colon, water and sodium is absorbed from the gut and, with the help of colonic bacteria, the stool is formed. The average person absorbs 1–1.5 l of fluid from the stool every day, leaving about 150 ml of stool water.
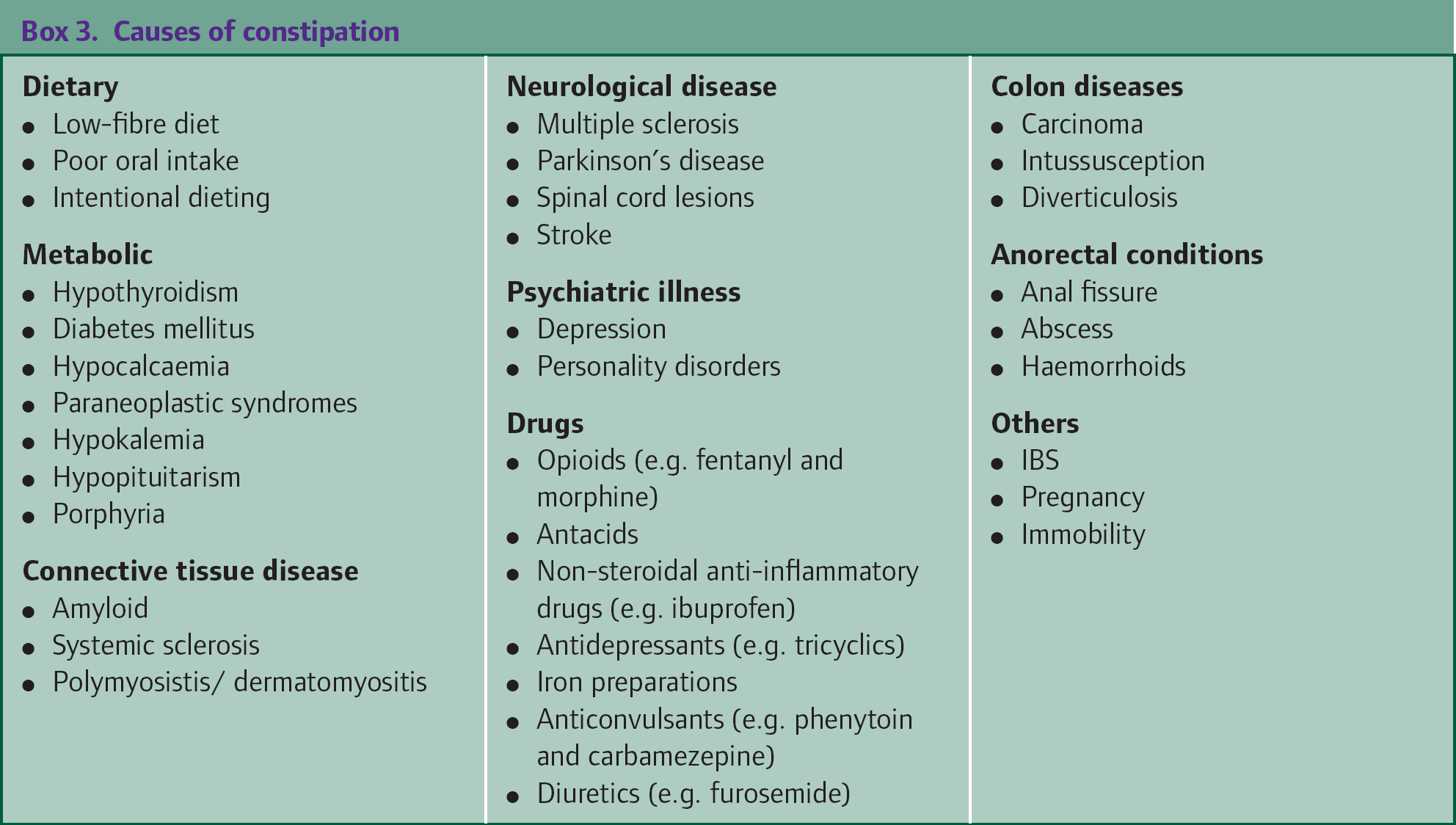
Box 2 lists some risk factors for constipation. Constipation can arise secondary to drugs or other disease processes (Box 3). However, constipation often results simply from the way that the individual's bowel functions, when it is termed primary or functional constipation. Patients with functional constipation can be divided into three distinct groups: those with normal transit times, those with slow transit through the gut and those with pelvic dyssynergia.
Risk factors for constipation
Age—more common in children and the elderly
Female gender
Low socio-economic status
History of chronic constipation
Low level of physical activity
Pregnancy
Poor dietary intake
Terminally ill patients
Normal transit constipation
In this form of constipation, the time taken for the stool to pass through the colon (the transit time) remains normal. Anxiety, psychosocial stress and emotions all seem to play an important role in development of this type of constipation. There may be sensory or psychomotor abnormalities of the anus or the rectum that contribute towards the pathogenesis. However, evidence for this is currently lacking.
Slow transit constipation
Impaired colonic motor function is the key problem in slow-transit constipation (Fig. 1). It is more common in females who usually present with feeling of general malaise, abdominal bloating and very infrequent bowel movements (sometimes less than once a week).

Abdominal x-ray showing faecal loading. The patient had a barium swallow 3 weeks before this x-ray was taken and barium can still be seen in the colon.
Pelvic floor dyssynergia
Pelvic floor dyssynergia arises from a lack of coordination between abdominal, anal, rectal and pelvic floor muscles. There is paradoxical contraction or failed relaxation of the puborectalis muscle and anal sphincter. It is thought to be due to learned behaviour acquired at the extremes of age (children or the elderly) to avoid discomfort and straining associated with defecation. Pelvic floor dyssynergia is difficult to treat medically and patients often report the need for manual evacuation.
Causes of constipation
Assessment of constipation in primary care
Constipation is the major reason for around 3 million GP consultations every year in the UK. It can be difficult to obtain an accurate history from patients presenting with constipation, partly because patient perceptions of what is normal can be extremely variable and partly because many people find it embarrassing and difficult to talk about bowel symptoms openly.
Establish the symptoms that the patient has. Ask about onset, duration, frequency and consistency of stools and any other associated symptoms, such as abdominal pain, urgency of passing stool, tenesmus or blood or mucus in the stool. Include a drug history, including over-the-counter medicines and illicit drugs. Check past medical history to exclude secondary causes of constipation.
The Bristol stool chart (Fig. 2) provides a good tool for the assessment of stool type, particularly in teenagers and young adults. It may also be used as a guide to monitor and tailor treatment.

Bristol stool chart.
Ask about lifestyle, including exercise, diet and alcohol intake. Explore health beliefs: around 80% of patients presenting with constipation to general practice believe that their bowels should open daily. Also enquire about any concerns about underlying disease. If symptoms are longstanding, ask why the patient is consulting now.
Examination
Perform a general physical examination with particular attention to the abdomen. Look for signs of anaemia, weight loss, abdominal masses, liver enlargement and palpable colon. With consent of the patient and appropriate chaperoning, consider performing a rectal examination to assess anal tone, any anal pathology such as fissures and for rectal masses and faecal impaction. This is particularly important in patients over the age of 40 years.
Investigations
Investigation in primary care should be kept to a minimum.
Consider:
a full blood count to exclude anaemia
erythrocyte sedimentation rate (ESR) and/or C-reactive protein (CRP) to exclude inflammatory bowel disease
thyroid function tests to exclude hypothyroidism
coeliac serology (and IgA levels) to exclude coeliac disease
Management in primary care
In all cases treat any underlying cause found. Treat symptomatically if no cause is found or if the underlying cause is untreatable.
Immediate referral
Refer immediately for secondary care assessment if there are any red flag symptoms suggestive of bowel cancer, such as unintentional and unexpected weight loss, persistent change in bowel habit for 6 weeks or more in anyone aged over 60 years, anaemia not related to menstrual loss or rectal bleeding that does not clearly originate from haemorrhoids or an anal fissure. Consider referral if the patient has a family history of bowel or ovarian cancer. Refer under the 2 week wait rule if National Institute for Health and Clinical Excellence (NICE) referral criteria are met (Box 4).
Lifestyle advice
In all cases give lifestyle advice. This can relieve symptoms and prevent recurrence in the future. Lifestyle advice includes: • Increasing fluid intake to more than 21/day (at least 8–10 cups)
Avoiding or cutting down on alcohol
Increase physical exercise if possible
Encourage patients to have regular meals and take time to eat; avoid missing meals and long gaps between meals
Add fibre to the diet by increasing fruit, vegetables and wholegrain foods and adding coarse bran to food
Advising patients to open their bowels when needed
Laxatives
If lifestyle advice alone fails and symptoms are causing distress, consider prescribing or advising the patient to buy a laxative over-the-counter. Table 1 lists some laxatives commonly used in primary care in the UK.
Commonly used laxatives

Tailor your choice of laxative to the patient's problem. For example, stool softeners are likely to be helpful for patients with hard lumpy stools and bulk-forming laxatives for people with poor dietary fibre intake. Similarly, stimulant laxatives should be reserved for patients with poor colonic motility. Titrate the dose to the response. Long-term use of stimulant laxatives (including co-danthrusate) is acceptable in the very elderly. Otherwise use as required or intermittently as long-term use is reported to cause colonic atony.
NICE referral guidelines for suspected lower gastrointestinal cancer
Refer urgently to be seen within 2 weeks by a team specializing in lower gastrointestinal malignancy if:
right lower abdominal mass consistent with involvement of large bowel
a palpable rectal mass (intraluminal, not pelvic; a pelvic mass outside the bowel would warrant an urgent referral to a urologist)
unexplained iron deficiency anaemia (haemoglobin of 110 g/dl or less for men or 100 g/dl or less for non-menstruating women)
rectal bleeding persisting for 6 weeks or longer without a change in bowel habit and without anal symptoms
change in bowel habit to looser stools and/or more frequent stools persisting for 6 weeks or longer without rectal bleeding
Routine referral for specialist assessment
If treatment with lifestyle measures and laxatives is unsuccessful, consider referral for specialist assessment. As well as the more usual investigations such as sigmoidoscopy, colonoscopy or barium enema, specialist investigations are available to identify the causes of functional constipation.
A colonic transit study can demonstrate slow transit as well as pelvic floor dyssynergia. In this test, the patient is asked to swallow a radio-opaque-labelled marker and daily x-rays are taken. Normal transit time is 3 days (72 hours). If transit through the colon takes 5 days or more, it is deemed ‘slow’. Similarly, if the labelled material passes through the colon normally but accumulates in the sigmoid colon or rectum, a diagnosis of pelvic floor dyssynergia is considered. Anorectal manometry is another useful test that evaluates the sphincter pressures and rectal sensations.
Treatment of pelvic floor dyssynergia or obstructed defecation can be particularly challenging, as these conditions do not respond to conventional dietary or laxative treatments. Behavioural treatment, such as biofeedback therapy, may be beneficial. This involves monitoring anal sphincter contractions during defecation and retraining patients to reduce these contractions and thus inhibiting their paradoxical response.
Constipation in specific situations
Elderly and terminally ill people
Occult presentations of constipation are common in the elderly and frail. These include:
Confusion
Urinary retention
Abdominal pain
Overflow diarrhoea and/or
Loss of appetite and nausea
Elderly people are five times more likely to develop constipation than young adults. Most of this is due to reduced mobility, chronic illness and polypharmacy.
Constipation is also a very common symptom among those with terminal illness. These patients may be elderly, are often relatively immobile and may eat and drink relatively little, all of which predispose them to constipation. They may have an underlying condition that causes constipation, such as Parkinson's disease, and may be on drugs such as opioids that make constipation more likely. It is important to remember that in patients with bony metastases from cancer, constipation may herald spinal cord compression. If suspected, a full neurological examination is essential.
Pre-empt constipation by putting all high-risk patients (such as those taking opioid analgesia) on regular aperients. Treat reversible causes, for example, by giving analgesia if there is pain on defecation, altering diet where possible, stopping non-essential drugs that might be causing constipation and increasing fluid intake.
Treat with regular stool softener (e.g. lactulose) either alone or in combination with a regular bowel stimulant (such as senna) or a combination drug (such as co-danthrusate). Titrate dose against the patient's response.
If oral medication is ineffective, consider adding rectal measures. If the patient has soft stools and a lax rectum, try bisacodyl suppositories. It is important that these come into direct contact with the rectum in order for them to work. If the patient has hard stools, try glycerol suppositories. Insert the suppository into the faeces and allow it to dissolve. If constipation still has not cleared, refer to the community nursing team for a lubricant and/or stimulant enema. Once constipation is cleared, leave the patient on a regular aperient with instructions to increase aperients if constipation recurs.
Pregnancy
Constipation is a common problem particularly in late pregnancy. Dietary changes and exercise are the mainstays of treatment in this situation and laxatives should be avoided if possible. Lactulose is safe and should be the first choice if drug treatment is needed.
Painful anorectal conditions
Patients with painful anorectal conditions such as anal fissure, haemorrhoids, fistula and abscess may develop constipation as a result of withholding stool to prevent pain. Treat with stool softeners to make passing stool less painful. Treat the underlying cause, for example, anal fissures may be treated initially with local anaesthetic gel. Local application of glyceryl trinitrate or calcium channel blocker ointment can also be tried. Haemorrhoids in the early stages respond well to application of local anaesthetic with, or without, steroid to improve the symptoms of pain and pruritis ani. If the patient continues to withhold stool despite stool softeners or the underlying condition does not respond to primary care treatment, consider secondary care referral.
Irritable bowel syndrome
Twenty percent develop symptoms of IBS in their lifetime. Constipation is the predominant symptom in 30% but other symptoms, such as abdominal pain or bloating, are also usually present.
IBS is a diagnosis of exclusion. How far to investigate is a clinical judgement weighing risks of investigation against possibility of serious disease. Factors to take into consideration include the age of the patient, family history, length of history and symptom cluster. In all patients, consider checking full blood count (to exclude anaemia), ESR or CRP to exclude inflammatory bowel disease and coeliac serology.
Education and reassurance form the basis of management of symptoms in these patients. Lifestyle and dietary measures must be tried before trying pharmacotherapy. It is important to note that some patients with IBS cannot tolerate high-fibre foods. Bran may also make some patients worse. For patients with constipation-dominant IBS, isphagula husk is better tolerated and may work well. If this is unsuccessful, try an osmotic laxative but avoid the use of lactulose as this may make bloating worse. Short cycles of stimulant laxatives can be tried as a second line.
If a patient fails to respond to treatment, consider another diagnosis. Review the history and examination and consider referral for further investigation.
Key points
Constipation is a common problem in UK general practice affecting about 15–20% of the population.
The GP is the first point of contact for patients presenting with symptoms of constipation and it is important for every GP to have a strategy to assess and manage such patients
Constipation may be functional or secondary to another cause, such as a chronic illness or drug treatment
It is important to treat any underlying causes of constipation and refer for specialist assessment if there are any red flags suggesting bowel cancer
For those with functional constipation, or if the cause cannot be treated, give lifestyle advice, and if this is not sufficient, start treatment with laxatives