
Abstract
Laryngeal cancer is a disease that usually presents with hoarseness. It is most common in older people and those of lower socio-economic classes. Understanding the warning signs and symptoms can help in making an early referral to the ear, nose and throat (ENT) specialist. This article aims to provide an overview of the ways in which laryngeal cancer can present, its treatment and problems that are sometimes encountered.
The GP curriculum and laryngeal cancer
UK health priorities—Early detection of head and neck cancer improves survival and evidence-based guidelines exist but are not widely used
Primary care management and contextual aspects—GPs should be aware of indications for appropriate referral to an ENT specialist. Training in ENT has been limited outside of specialist training programmes, so increasing the risk of inappropriate referrals and under-referral.
The knowledge base and specific problem-solving skills—Hoarseness, dysphagia, neck swellings and otalgia are all potential symptoms of benign and malignant ENT conditions. GPs should be able to recognize warning features of head and neck cancer and not delay referral with unnecessary investigations.
Epidemiology, risk factors and pathology
Laryngeal cancer is the most common head and neck cancer. It is mainly a disease of middle-aged men, with peak incidence in the seventh decade. Women affected tend to be younger, with peak incidence before the age of 60 years. The UK combined annual incidence is approximately 3 per 100 000 but as high as 8.2 per 100 000 in Scottish males.
Smoking is the main risk factor, and up to 98% of patients with laryngeal cancer are smokers. Smoking and high alcohol consumption in combination has a synergistic effect on risk. Other aetiological factors include occupational exposure to dust and gas compounds or polluted work environments. Those working with asbestos, wood dust, cement dust and tar seem to have an increased risk. Acute or chronic laryngeal inflammation caused by reflux may also be a carcinogenic cofactor and infection with human papilloma virus (HPV) has been implicated in some cases.
More than 90% of laryngeal cancers are squamous cell carcinomas. For descriptive purposes the larynx is divided into three regions:
The supraglottis comprises the laryngeal surface of the epiglottis, aryepiglottic folds, arytenoids, false cords and ventricles. Carcinoma arising in this region accounts for approximately 40% of all laryngeal carcinoma.
The glottis comprises the vocal cords (Fig. 1) and the anterior and posterior commissures. Tumours in this region account for about 59% of all laryngeal carcinoma.
Squamous cell carcinoma of the left vocal cord.
The subglottis extends from the lower border of the cricoid to the under surface of the vocal cords and is the least frequent site (1%) for laryngeal carcinoma to arise
Clinical features
Symptoms of laryngeal cancer are summarized in Box 1. The patient's symptoms will depend upon which site within the larynx is affected.
Symptoms and signs of laryngeal cancer
Hoarseness
Pain—often referred to the ear
Dysphagia
Breathing difficulties—beware the patient with chronic obstructive pulmonary disease and stridor
Stridor
Lymph node enlargement in the neck
Weight loss
Haemoptysis
Glottic tumours present early with hoarseness and metastasize late. This is because they have a very small space to grow in and there is a poor lymphatic supply to the area. For this reason glottic cancer has the most favourable prognosis of all forms of laryngeal cancer as people tend to seek medical advice early. Suspect laryngeal cancer in any patient with persistent hoarseness of the voice for 3 weeks or longer, until proven otherwise. Other possible causes of hoarseness are listed in Box 2.
Differential diagnosis of hoarseness
Acute laryngitis: associated with upper respiratory tract infection
Vocal cord polyp, cyst or nodule
Vocal cord granuloma
Laryngeal papilloma
Carcinoma
Muscle tension dysphonia: associated with voice abuse and gastro-oesophageal reflux. Hoarseness is variable, and comes and goes.
Vocal cord palsy: resulting from recurrent laryngeal nerve palsy
Motor neurone disease
Multiple sclerosis
Myaesthenia gravis
Muscular dystrophy
Drugs, e.g. steroid inhalers—can cause myopathic weakness of the adductor muscles of the vocal cords leading to dysphonia, this effect is reversible on cessation of inhaled steroid treatment. The use of a spacer does not appear to help with hoarseness associated with inhaled corticosteroid use
Hypothyroidism
Patients with subglottic tumours may present with hoarseness if the tumour extends superiorly to involve the glottis but, generally, dysphonia is a late feature with patients more commonly presenting in respiratory distress or with stridor (a high-pitched inspiratory noise indicative of upper airways obstruction). Throat pain and unilateral otalgia are also indicative of advanced disease.
Supraglottic tumours, on the other hand, present later and metastasize earlier. The bigger space available to grow conceals the primary for longer and greater lymphatic supply facilitates its spread to the local neck nodes. Symptoms on presentation are variable and may include hoarseness, neck swelling, dysphagia or respiratory problems.
Management in primary care
With the exception of a chest X-ray for patients with persistent hoarseness, investigations for head and neck cancer in primary care are not recommended as they can delay referral (National Institute for Health and Clinical Excellence (NICE), 2005). Patients with suspected head and neck cancer should be referred urgently for ENT assessment under the 2 week wait rule. Box 3 summarizes NICE criteria for urgent referral.
Criteria for urgent referral of patients with suspected head and neck cancer (2 week rule)—relating to laryngeal cancer
Unexplained persistent sore throat or painful throat or persistent dysphagia lasting more than 3 weeks
Unexplained unilateral pain in the head and neck area for more than 4 weeks, associated with otalgia but a normal otoscopy
Patients with persistent hoarseness for more than 3 weeks with negative chest X-ray (some local guidelines differ and recommend referral before the chest X-ray results are reported)
Unexplained lump in the neck of recent onset or previously undiagnosed lump that has changed over a period of 3–6 weeks
Specialist assessment
Throat and neck examination
When a patient is referred to an ENT department with any symptoms or signs suggestive of laryngeal cancer, a complete head and neck examination is performed. This includes a direct examination of the larynx using a flexible nasoendoscope (Fig. 2). This is a painless procedure done in the ENT clinic, with or without a nasal spray containing lidocaine and a nasal decongestant. It allows for the visualization of the hypopharynx and larynx down to the level of the vocal cords.

Nasoendoscopy being performed in the ENT clinic.
Abnormalities such as irregular lesions of the glottis or supraglottis, oedema and impaired vocal cord mobility are easily identified. Photographs and video recordings can be made to document and compare findings. Flexible endoscopy can also identify other benign laryngeal lesions such as polyps or Reinke's oedema that might be the cause of the patient's symptoms.
Attention is also paid to the airway status—advanced lesions can physically obstruct the airway and urgent intervention (such as tracheostomy, intubation and/or debulking surgery) rarely might be necessary. Other important parts of the examination include palpation of all parts of the neck to identify any cervical lymphadenopathy and assessment of the rest of the upper aero-digestive tract for second primaries.
General examination
A more general examination of the patient allows for a good estimate of nutritional status, which is often compromised in any patient with a head and neck malignancy. It is also important to identify any medical co-morbidity that the patient might have. Smoking and alcohol abuse are risk factors for laryngeal carcinoma as well as being risk factors for cardiac, pulmonary and liver disease and, if present, can significantly alter management and prognosis.
Biopsies
Direct microlaryngoscopy and biopsy are the investigation of choice. This is performed under general anaesthesia and it usually involves an overnight stay in hospital. A rigid laryngoscope is used to visualize in detail the larynx and hypopharynx, providing some of the information necessary to stage the disease. During this procedure, biopsies of the lesion are taken and sent for histopathological examination that will usually provide the definitive diagnosis including the histological subtype. This often takes at least seven working days.
Radiographic tests
The radiological investigation of choice is a computed tomography (CT) scan from skull base to diaphragm. Laryngeal cancer spreads first to the regional cervical lymph nodes, and the second most common site for metastasis is the lungs. Moreover, around 5% of patients presenting with laryngeal cancer also have a synchronous primary lung lesion. This is why the chest is included in the CT scan.
Staging
The stage of a malignant lesion refers to the extent of spread. The tumour, node and metastasis (TNM) system is commonly used and indicates the size and extent of local spread of the primary tumour or neoplasm (T), the presence, size and site of cervical lymph node metastases (N) and the presence or absence of distant metastases (M).
The stage of the disease is crucial to planning further management and is an indicator of the prognosis. For example, small primaries that have spread to the lymph nodes have half the 5 year survival rates that small nodenegative lesions have.
Treatment
Once a diagnosis of laryngeal cancer is made, each patient's case is discussed at a multidisciplinary team (MDT) meeting involving ENT surgeons, radiologists, oncologists, pathologists, head and neck cancer nurses, speech therapists and dieticians. A treatment plan is agreed upon, including decisions on the type of treatment modality to be used, where the treatment will take place and which health professionals are to be involved in the care. Following this, the patient is seen by the team and the diagnosis, prognosis and management plan are explained. Contact numbers are given to the patient for 24 hour help and advice.
The three modalities of treatment are surgery, radiotherapy and chemotherapy. Patients with early stage disease are managed with a single modality, whereas multiple (combined) modalities are used in advanced disease. Those with supraglottic disease require treatment of the neck (surgery or radiotherapy) because of the increased risk of metastasis with these tumours.
Surgery
Endoscopic laser resection is being increasingly used in the management of small laryngeal cancers (stage T1 and T2). It has the same outcome as radiotherapy and is less prolonged. The patient's voice may be impaired temporarily. Laser resection can be repeated and radiotherapy can still be used for salvage treatment, i.e. should the tumour recur and further laser resection not be possible.
Surgical treatment includes total laryngectomy or more rarely hemi-laryngectomy. Laryngeal transplantation is at a basic science research stage. Total laryngectomy is a major procedure and leaves the patient with a permanent tracheostomy. It involves removal of the larynx from (and including) the hyoid bone down to the upper tracheal rings. It has the effect of separating the respiratory tract from the gastrointestinal tract (Fig. 3).
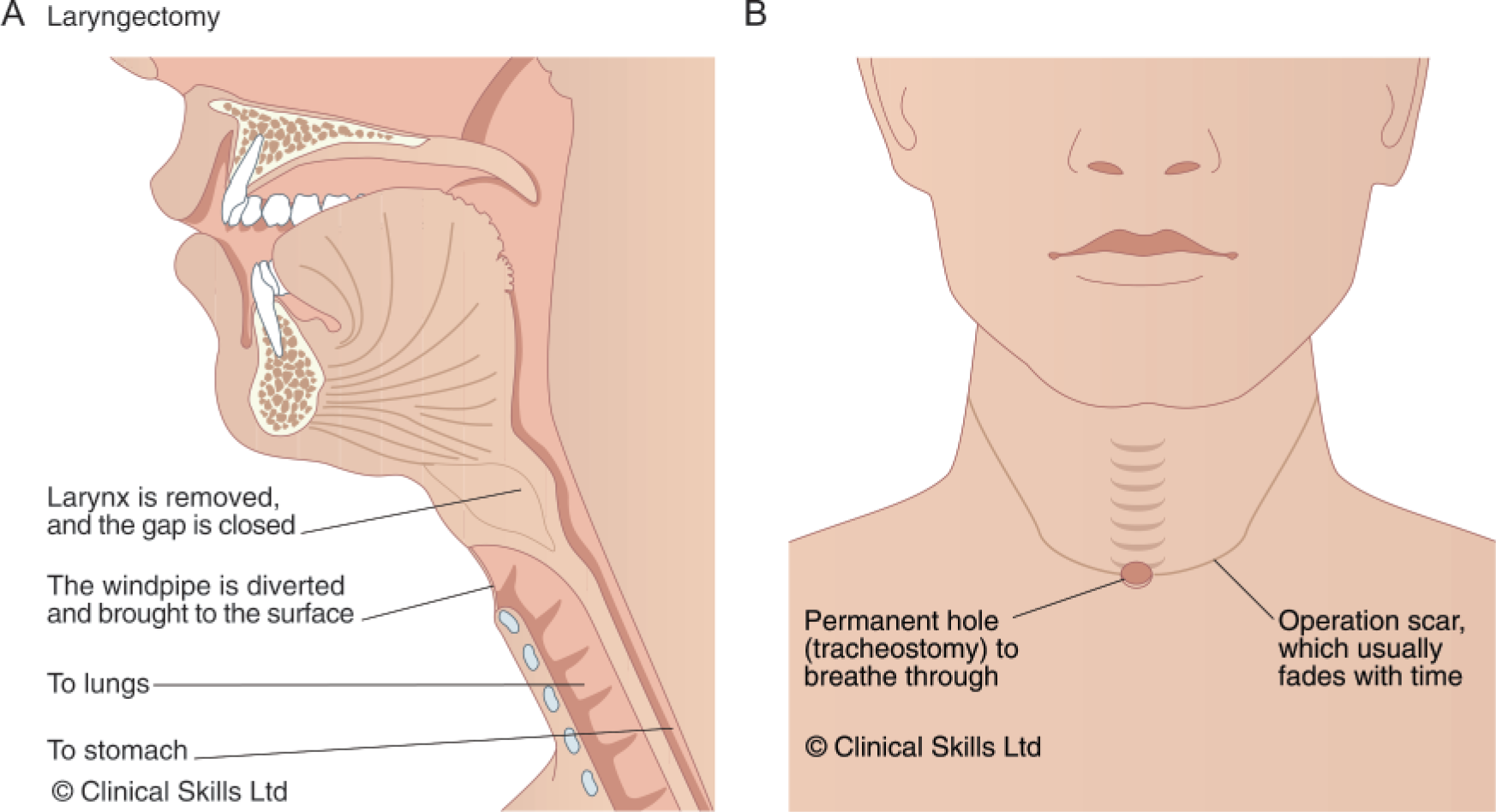
Cross section of the head and neck after laryngectomy.
A hemi-thyroidectomy is usually performed at the same time, depending on the side of the primary tumour. A selective neck dissection may be necessary if there are any cervical lymph node metastases. This involves removing the lymph nodes together with the primary tumour.
Since the laryngeal inlet is situated anterior to the pharynx, the anterior wall of the hypopharynx is opened as part of the procedure. This is closed primarily using sutures but for more extensive surgery, a skin flap may be used to reconstruct the defect.
During the procedure a communication between the posterior wall of the upper end of the trachea and the adjoining wall of the oesophagus is often made. This is known as a tracheo-oesophageal fistula. It forms the site for the insertion of a speaking valve, either during the procedure or at a later stage, which allows for phonation after this operation.
Patients should expect to stay in hospital for at least 10 days after surgery. During this time, special attention is paid to nutritional supplementation, which helps their recovery from the surgery. Patients are also visited by the head and neck cancer nurse specialist and taught how to manage the tracheostoma site.
Radiotherapy
Radiotherapy can be used as the only treatment in early cancers. If used in conjunction with surgery, it usually starts within 6 weeks of surgery, if complications allow. The whole treatment usually lasts 5–6 weeks and is administered daily, excluding weekends. It is important not to miss any treatments.
Early complications during treatment include skin erythema and tenderness, mucositis, dysphagia and odynophagia. Mucositis can be so severe as to necessitate hospital admission for nasogastric or percutaneous endoscopic gastrostomy (PEG) feeding and opioid pain relief. Many units now insert radiologically guided PEG tubes prior to treatment, especially if radiotherapy is combined with chemotherapy.
Long-term side effects of radiotherapy include xerostomia (dry mouth), oedema, induration, a degree of fibrosis of the neck tissues, dysphagia and malignant change in irradiated tissues. A dental examination is important in the workup prior to radiotherapy as carious or diseased teeth need to be removed before starting treatment. This is done to avoid the risk of osteoradionecrosis.
Chemotherapy
In the UK, chemotherapy is usually used in combination with radiotherapy. In some, chemotherapy is used as a ‘neoadjuvant’—to shrink the tumour prior to surgery and may also be used for the palliation of advanced disease. It is normally only considered in patients with more advanced disease. Those over the age of 65 years or with significant renal impairment tend to do badly and so are less likely to be offered chemotherapy.
Follow-up
Hospital follow-up for laryngeal cancer patients is normally for 5 years from the end of treatment. It is monthly for the first year, reducing to 6 monthly in the final year. Head and neck review clinics are staffed by ENT surgeons, oncologists, dieticians, the head and neck nurse and a speech and language specialist. It is an opportunity not only to conduct examinations to detect recurrence but also to screen for other post-operative problems and second primaries.
Specific post-operative problems
Swallowing
Swallowing may be affected by laryngectomy. Dietician input can help patients adapt to their new swallowing needs and optimize their dietary intake. Many laryngeal cancer sufferers have poor dietary habits even prior to their diagnosis.
Depending on the extent of surgery, the anastomosis of the hypopharynx can result in a stricture, which in turn may cause dysphagia post-operatively. Strictures are investigated and monitored with barium swallow tests. Stricture dilatation under general anaesthetic may be needed, sometimes recurrently, for patients with significant stenosis.
In some, dysphagia is not due to a physical constriction, but a functional one. Botulinum toxin can be injected to relax tight pharyngeal constrictors and may also be useful for patients who are having difficulty vocalizing.
Olfaction
Following laryngectomy, sense of smell and taste is altered due to the abolished airflow through the nose. Radiotherapy might also damage the taste buds.
Hypothyroidism
Hypothyroidism may be a cause for unexplained tiredness or even depressive symptoms. It results from the combined effects of a hemi-thyroidectomy, devascularization of the remaining part of the thyroid gland and irradiation of the neck. Life-long replacement therapy with levothyroxine is sometimes necessary.
Tracheostoma problems
Total laryngectomy patients can have their tracheostoma decannulated once the surgeon is satisfied that the wound is dry and healing well. A small removable sialastic ‘button’ or vent is often inserted to prevent late stenosis.
Patients are taught how to routinely look after their stoma on the ward and deal with crusting that could cause a blockage if left. Normally, air drawn into the trachea is humidified in the upper airways. After laryngectomy, air is drawn directly from the outside into the trachea. Crusting results from squamous metaplasia of the trachea and lack of humidification of inspired air. Secretions dry and accumulate around the stoma and potentially can cause acute respiratory compromise.
Wearing a specially designed bib helps to increase humidity levels, prevents rapid expulsion of tracheal excretions and may help with potential body image problems. More sophisticated devices, such as the humidity and moisture exchanger (HME), are now in common usage. These provide similar benefits to the bib and also improve gas exchange in the lungs by decreasing expiratory airflow.
Voice rehabilitation
Early laryngeal cancers managed with radiotherapy alone might result in persistent hoarseness due to the effect of radiation on the larynx. Surgery involving minor resections may also be accompanied by persistent hoarseness following treatment.
Loss of voice is one of the biggest concerns for patients contemplating total laryngectomy. This is a concern that should be explored and discussed prior to surgery by the surgical team and the unit's head and neck nurse and speech and language therapist. In the ideal situation, patients undergo surgical voice restoration with the insertion of a voice prosthesis prior to discharge from hospital (Fig. 4).
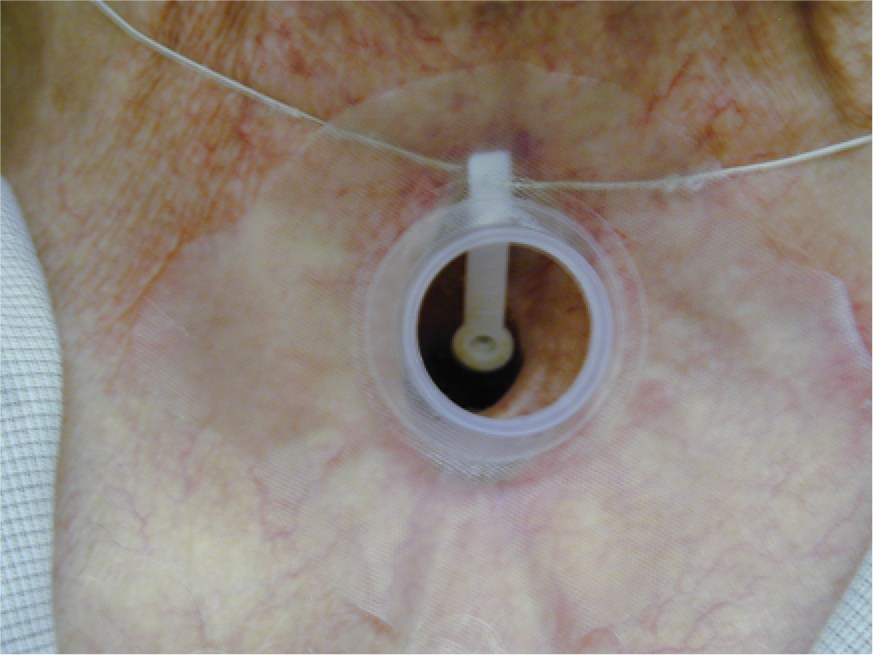
A voice prosthesis in place and transparent tracheostoma dressing.
Voice prostheses come in many varieties but all are essentially one-way valves inserted into the fistula created between the posterior tracheal wall and the oesophagus. Air passes from the lungs into the oesophagus. It escapes from the oesophagus via the oropharynx and oral cavity, which vibrate to provide a sound. The sound can be articulated into speech by movements of the mouth and tongue. Interestingly, patients keep their regional accents. Diversion of air into the neopharynx requires occlusion of the stoma usually with the patient's thumb, but in some, a ‘hands-free’ valve is taped over the stoma allowing air to enter into the lungs on inspiration but occluding on expiration, so forcing air through the speech valve.
Problems with voice prostheses
Some patients are not suitable for a voice prosthesis. A degree of manual dexterity is required to achieve voicing and look after the valve, severe chronic obstructive airways disease limits the airflow that can be achieved and dementia prevents sufficient learning of new techniques required.
Not all who are fitted with a prosthesis are able to voice well to begin with. If the patient is able to make some speech-like sounds when the prosthesis is briefly removed, then technical issues with the prosthesis and pharyngeal tone have to be explored. This is done in conjunction with the speech and language therapists. Overall though, about 80% of patients will have useful or good voice post-operatively.
An important complication is expulsion of a voice prosthesis that sometimes happens unnoticed or while attempting to cough. The fistula tends to close rapidly and, if allowed to, will disappear within a few hours. Some patients are competent enough to insert a stent by themselves prior to attending the ENT department, otherwise a doctor can insert a sialastic urinary catheter and secure it on the chest wall to prevent significant closure.
Another significant problem with voice prostheses is leakage. Eventually, saliva or other liquids imbibed will start to pass from the oesophagus into the trachea. This can cause aspiration and, if unnoticed, is a significant threat to the patient's health. Leakage is associated with a clogging of the valve by candidal overgrowth. This can be delayed by daily amphotericin lozenges, but all leaking valves eventually require replacement in the ENT clinic. This is a quick procedure performed with local anaesthetic spray.
For a few, especially those who have had radiotherapy prior to surgery, the fistula recurrently breaks down. The only option for these patients is for the fistula to be closed surgically. Depending on personal preference, the patient must then learn oesophageal speech, use an electro-larynx, silent articulation or simply pen and paper. Oesophageal speech was the closest to normal speech prior to surgical voice restoration and requires swallowed air to be expelled in short gulps to vibrate the pharynx as with a voice prosthesis. However, only a third of patients produce a good quality of voice in this way. Electro-larynx devices pick up muscle contractions in the pharynx when applied to the skin on the side of the neck to produce a modulated electronic-sounding noise. They require little dexterity, so are suitable, for example, in those with deformed arthritic hands.
Support
Although many patients with laryngeal cancer get back to a near-normal life, quality of life issues are increasingly recognized. Ongoing problems tend to result from job difficulties if previously required to lift heavy objects (laryngectomees are unable to perform the valsalva manoeuvre), body image problems, sexual dysfunction and issues relating to altered speech and smell.
Patients are vulnerable as those who smoke and drink tend to have done so as a way of life, often with informal support networks consisting of other smokers and drinkers or without any close relationships at all. Help with alcohol addiction may be required.
Various support groups exist for laryngectomees. The National Association of Laryngectomee Clubs, the Cancer Laryngectomee Trust (www.cancerlt.org) and the Head and Neck/Tracheostomy/Laryngectomy Support Group (www.macmillan.org.uk), run by Macmillan Cancer Support, are examples of associations that provide advice and support for people after laryngectomy. There are also many other smaller associations that offer support at a local level.
Prognosis
Overall, nearly two-thirds of all laryngeal cancer patients can be expected to be disease free at 5 years. Currently, treatment for early stage (T1 and T2) laryngeal cancer in the UK gives up to 80% 5 year survival. There has been less improvement in survival rates over recent years compared with many other cancers, possibly because most patients with laryngeal cancer are long-term smokers with coexistent cardiovascular disease and other health problems (NICE, 2004).
Key points
Laryngeal cancer is a disease that mostly affects people in their 60s and 70s who have been exposed to years of smoking and/or alcohol
Persistent hoarseness is frequently, but not exclusively, the presenting complaint
There are no investigations indicated in general practice for suspected head and neck cancer apart from a chest X-ray in the presence of persistent hoarseness for more than 3 weeks
Laryngeal disease that has spread to the neck lymph nodes represents advanced disease with a poorer prognosis
Treatment is with one or a combination of radiotherapy, surgery and chemotherapy: treatment decisions are made by an MDT
Voicing after laryngectomy can be achieved by several methods: choice depends on individual patient factors