
Abstract
In the UK, 15% of consultations in primary care relate to problems with the skin. Bacterial skin infections are common and range widely in their size, severity and variety of skin changes produced. This article aims to provide information on the clinical presentation and management of bacterial skin infections including folliculitis, furunculosis, impetigo, ecythma, staphylococcal scalded skin syndrome, cellulitis, erysipelas and necrotizing fasciitis.
The GP curriculum and bacterial skin infections
Elicit the appropriate signs and symptoms and subsequent investigation/referral of people presenting with signs of infection of the skin
Have knowledge of commonly used treatment in primary care (including an awareness of appropriate quantities to be prescribed and how to prescribe them)
Recognize and intervene urgently in severe/life-threatening skin infection
Have knowledge of preventative strategies in skin infection
Appreciate the importance of the social and psychological impact of skin problems on a patient's quality of life.
Skin as a barrier
The skin provides an excellent barrier function against infection. Although many bacteria come into contact or reside on the skin, they are normally unable to establish an infection. Furthermore, the skin's normal bacterial flora helps prevent colonization by pathogenic organisms. It follows that any breach in epidermal integrity of the skin can allow penetration of bacteria and subsequent infection to develop. The protective barrier is naturally breached at sweat glands and hair ducts and organisms may use these as portals of entry.
Risk factors for skin infection
Some individuals are at greater risk of developing and having more extensive bacterial skin infections (see Box 1). Recognizing patient risk is important as it may impact on treatment choice, length of treatment, follow up and awareness of potential complications.
Risk factors for developing skin infection
Recent skin trauma
Conditions compromising the immune system
Diabetes
Human immunodeficiency virus (HIV)/acquired immune deficiency syndrome (AIDS)
Patients receiving chemotherapy
Steroid therapy
Poor health, nutrition and hygiene (plus alcoholism and intravenous drug users)
Conditions impacting on venous and lymphatic circulation
Obesity
Pregnancy
Chronic venous insufficiency
Chronic skin conditions (e.g. eczema and psoriasis)
Many bacteria can infect the skin, the most common being Staphylococcus and Streptococcus (see Table 1). This article presents the different clinical presentations caused by these organisms and the subsequent management of each condition.
Bacterial skin infections and their most common causative agent

Folliculitis
Folliculitis is a primary inflammation of the hair follicle that occurs usually as a result of infection. The infection can be superficial or deep. Folliculitis can also develop secondary to follicular trauma (i.e. shaving) or occlusion and specific skin diseases.
Superficial folliculitis is a relatively common self-limiting condition and patients rarely present to their GP. Those who are seen often have deep folliculitis or recurrent or persistent superficial folliculitis. The condition can affect all ages and any hair-bearing site. The sites most commonly involved are the face, scalp, thighs, axilla and inguinal area.
The patient presents with an acute onset of papules and pustules on an erythematous base associated with discomfort and pruritis (see Fig. 1). Deeper lesions present as erythematous, often fluctuant, nodules. When involvement of a follicle is more extensive, folliculitis can develop into cellulitis and furunculosis. Persistent or recurrent lesions may result in scarring and permanent hair loss.

Folliculitis.
Stye
A stye is folliculitis associated with the eyelash. The patient presents with pain, redness and swelling over the eyelid. Initially, the whole of the lid may be affected; however, the swelling soon becomes localized and a pus-filled lesion may be seen near the lid margin (see Fig. 2).

Stye.
Barber's itch
Barber's itch is a type of folliculitis in which lesions are seen in the bearded area and are often caused by Staphylococcus aureus or a dermatophytic infection. Barber's itch is referred to as sycosis barbae if caused by S. aureus or tinea barbae if due to a fungal infection. It presents with a rash over the bearded area with itching and papules or pustules associated with the hair follicle (see Fig. 3). It occurs more commonly in frequent shavers and those with nasal carriage of S. aureus.

Barber's itch.
Gram-negative folliculitis
Antibiotic-related folliculitis occurs on the face in patients taking long-term antibiotics. It usually follows oral tetracycline treatment of acne and is quite rare. The skin's normal flora is altered in favour of gram-negative organisms (such as Pseudomonas, Enterobacter, Klebsiella, Escherichia, Serratia and Proteus species) causing multiple small pustules to develop.
Hot tub folliculitis is another gram-negative folliculitis (usually caused by Pseudomonas) also known as spa or wet-suit folliculitis. Follicular-based papules and pustules develop within 48 hours of exposure to contaminated water or wet suits, usually in areas occluded by swimwear (see Fig. 4 that demonstrates the development of lesions after wearing a bikini). It may cause systemic symptoms such as fever, headache, malaise, gastrointestinal upset and sore throat but is a self-limiting condition that does not usually require treatment and resolves in 1–2 weeks. Showering after exposure to pool water does not seem to have an impact on the condition but maintenance and chlorination of pools can help decrease the population of Pseudomonas.

Hot tub folliculitis.
Non-infectious folliculitis
Irritant folliculitis may arise due to irritation from regrowing hairs after shaving or waxing. Swabs taken from the pustules are sterile. In the beard area, a type of folliculitis known as pseudofolliculitis barbae can occur. This primarily occurs in racial groups with thick, coarse curly hair. It is described as a perifolliculitis due to the hair re-entering the skin adjacent to its exit point from the follicle, thus acting as a foreign body inciting an inflammatory response. Advise the patient to allow the beard to grow for a few weeks to eliminate ingrown hairs. When resuming shaving, advise the patient to use a single-blade razor (more blades cut the hair shorter, increasing the risk of ingrown hairs) and to shave in the direction of the follicle without stretching the skin.
Acne represents a non-infectious form of folliculitis. The follicular inflammation seen in acne occurs as a secondary event as a result of follicular obstruction from abnormal keratinization. The hair follicle becomes obstructed by a keratin plug and the normally commensal bacteria (Propionibacterium acnes) trigger follicular inflammation. Papulopustular follicular drug eruptions can occur secondary to various medications such as anticonvulsants and chemotherapy. Finally, eosinophilic folliculitis can occur in patients who are immunocompromised. Its cause is not yet understood.
Management of folliculitis
Discussion of hygiene and the use of antibacterial washes (e.g. chlorhexidine) may be all that is required in uncomplicated superficial folliculitis. Topical antibacterials/antibiotics can be used as first-line treatment for recurrent superficial folliculitis. Swabs should be taken from the pustules for culture prior to commencing therapy. As the infection is usually due to S. aureus, topical choices include fusidic acid, mupirocin or neomycin for 7–10 days. If local treatment is ineffective, or the infection is severe or widespread, systemic antibiotics may be indicated. First-line antibiotic choice is flucloxacillin or erythromycin for 7 days.
If a patient does not improve with a standard course of antibiotics, therapy should be guided by culture sensitivity and other causes of folliculitis must be investigated. In recurrent or chronic cases treat carrier sites with mupirocin ointment twice a day for 5 days.
In Gram-negative folliculitis, high-dose trimethoprim (300 mg bd in adults) is the antibiotic of choice. In hot tub folliculitis, usually a benign self-limiting infection, antibiotic treatment with ciprofloxacin should be considered in patients with fever and constitutional symptoms or those with resistant infection.
Referral to a dermatologist may be indicated if lesions are not improving, there are recurrent disease episodes and/or lesions are causing scarring. Complications of folliculitis are uncommon but include cellulitis, scarring, permanent hair loss and furunculosis. Furuncles or boils are a deep infection of the hair follicle (see Fig. 5). They can cluster together and form carbuncles (a deep infection of a number of hair follicles). Large boils form abscesses that may require incision and drainage in addition to antibiotic therapy.

Furuncle.
Impetigo
Impetigo is a highly contagious condition caused by infection of the superficial layers of the epidermis by S. aureus, Streptococcus pyogenes or both. It may arise after contact with another sufferer, start after a minor skin injury or appear unexpectedly, seemingly without cause.
Impetigo is characterized by thin-walled vesicles, rupturing easily to leave an extending area of exudation and honey-coloured crusts (see Fig. 6). Multiple lesions often occur, particularly around the face. Usually the infection is asymptomatic but occasionally the patient may complain of a slight burning or itching at the site of the lesion.

Impetigo.
While impetigo can manifest as a primary skin infection, it may also occur as secondary infection of pre-existing skin disease, such as eczema or herpes simplex, a process called impetiginization. Impetigo rarely progresses to systemic infection although streptococcal impetigo can very infrequently cause a post-streptococcal glomerulonephritis.

Ecthyma.
Management of impetigo
Advise patients on the prevention of spread to others by avoiding close contact and using separate towels; stress the importance of not touching the lesions. Some schools advise that children must stay at home until the lesions have healed. The Health Protection Agency (2006) recommends exclusion from school or nursery until lesions are crusted or healed; however, due to lack of evidence, new Dutch Guidelines for general practitioners (2008) on bacterial skin infection no longer recommend exclusion from school.
Gentle debridement of crusted lesions using an antibacterial wash (e.g. chlorhexidine) and a washcloth is generally recommended; however, there is little evidence that using disinfectant solutions improves impetigo. Topical antibiotics such as fusidic acid [or mupirocin if methicillin-resistant Staphylococcus aureus (MRSA)] are recommended as first-line treatment. They can be applied two to three times daily with a 7 day course usually being adequate. A recent Cochrane review found no superiority between fusidic acid or mupirocin. The review also details that topical treatment can be considered as effective as, or more effective than, oral antibiotics for limited disease, with topical agents having fewer side effects. This finding is in contrast to the commonly held view that oral treatment is superior to topical treatment. From a practical perspective, oral antibiotics may be preferable for people with very extensive disease. Oral erythromycin can be used if infection is widespread; a 7 day course should be supplied. Studies have shown oral penicillins to be inferior to erythromycin in treating impetigo.
Ecthyma
Ecthyma is a skin infection characterized by ulcers forming under a crusted surface infection. The infection extends into the dermis and is often referred to as a deeper form of impetigo as the same bacterial pathogens are involved.
Management of ecthyma
The treatment of ecthyma is the same as impetigo by soaking and debriding the crusted areas, together with topical and possibly oral antibiotics if the lesions are extensive. The duration of treatment varies with several weeks of therapy sometimes necessary to completely resolve lesions. Improving hygiene is an important factor in the treatment—advise patients on washing daily with antiseptic soap, changing and laundering clothes and bed linen frequently and of the importance of using separate towels to prevent infection spreading.
Staphylococcal scalded skin syndrome
Staphylococcal scalded skin syndrome (SSSS) is a toxin-mediated type of exfoliative dermatitis caused by S. aureus. Exotoxins are released by some strains of S. aureus and cause detachment within the epidermal layer. SSSS is a syndrome of erythematous cellulitis followed by acute exfoliation of the skin. It can vary in severity from a few blisters to a severe exfoliation affecting the entire body.
SSSS mostly occurs in children less than 5 years old. Adults are usually protected by the antibodies against staphylococcal exotoxins acquired during childhood with very few cases being reported among adults in the literature. Neonates are most at risk due to their lack of specific immunity and their immature renal system being unable to excrete the toxins. Adults who are immunocompromised or individuals with renal failure may also be at risk of developing SSSS. Outbreaks of SSSS often occur in childcare facilities as asymptomatic adult carriers introduce the infection.
SSSS presents as a red rash followed by diffuse epidermal exfoliation. Fluid-filled blisters form, rupturing easily, leaving an area that looks like a burn (see Fig. 8). The area is tender and warm to palpate and the patient may have a fever and experience general malaise.

Staphylococcal scalded skin syndrome.
Management of SSSS
Treatment of SSSS requires hospitalization for intravenous antibiotics and fluid replacement. Flucloxacillin is usually the antimicrobial of choice. Dependent on treatment response, oral antibiotics can be substituted in several days. Other supportive treatment includes paracetamol for pyrexia and pain, the maintenance of fluid and electrolyte balance and skin care. SSSS usually follows a benign course and generally healing is complete within 5–7 days of commencing treatment.
The mortality in adults is high at 50-60% but much lower in children (1–5%). Differentiating SSSS from toxic epidermal necrolysis (TEN) that carries a much higher mortality is important. In SSSS, the mucous membranes are spared. In TEN, mucous membranes (mouth, oesophagus, anus and vagina) are almost always affected.
Cellulitis
Cellulitis is a common bacterial infection causing inflammation of the dermis and hypodermis of the skin. It usually develops secondary to a break in the skin where organisms gain entry to the dermis and multiply. Facial cellulitis of odontogenic origin may also occur. The most common bacterial pathogens involved are Streptococcus pyogenes and S. aureus.
The patient usually presents complaining of pain and swelling at the site of infection. Cellulitis most commonly affects a limb but anywhere on the body can be affected. Involved sites are erythematous, hot, swollen and tender (see Fig. 9). Lymphangitis, regional lymphadenopathy or both may be present. Symptoms and signs are usually localized to the affected area but bacteraemia can occur causing the patient to become systemically unwell with malaise, chills and fever. Severe or rapidly progressive cellulitis may cause blistering, abscess formation and necrotizing fasciitis. Cellulitis must be differentiated from lower leg eczema and acute venous problems including deep vein thrombosis, thrombophlebitis and vasculitis.

Cellulitis.
Management of cellulitis
Most cases of cellulitis are mild and can be treated in the outpatient setting with oral antibiotics. Flucloxacillin (500 mg to 1 g four times a day) will adequately cover the most common causes of cellulitis: S. aureus and streptococci. For patients with penicillin allergy, clarithromycin 500 mg bd is a second-line alternative. Consider patients with a large area of cellulitis and those with systemic upset or risk factors for poor outcome for hospital admission for intravenous antibiotic therapy.
Treatment length has not been extensively studied but most cases of uncomplicated cellulitis can be successfully treated with 1–2 weeks of therapy. With regards to prognosis, following a cellulitis episode of the leg, approximately 7% of patients develop chronic oedema and up to one in three patients develop a recurrent episode within 3 years. This is usually attributable to chronic venous insufficiency.
Erysipelas
Erysipelas is an acute bacterial infection of the skin and subcutaneous tissue that characteristically extends into the cutaneous lymphatics. It is a superficial form of cellulitis, almost always caused by Streptococcus pyogenes, but occasionally other beta haemolytic streptococci or, rarely, staphylococci are implicated.
Erysipelas begins as a small erythematous area on the skin that progresses to an indurated, fiery-red tense and shiny plaque that may blister (see Fig. 10). Fever, malaise and chills are usually present and often begin before the onset of skin changes. The lesion has well demarcated advancing margins, displaying local signs of inflammation being warm, oedematous and tender. Affected skin is differentiated from cellulitis by this well defined raised border, reflecting its more superficial nature. Cellulitis has no lymphatic component and exhibits indiscreet margins. However, in many cases it is difficult to make a distinction between cellulitis and erysipelas and the two processes often coexist. Current thought tends to regard erysipelas as a form of cellulitis rather than a distinct entity.

Erysipelas.
Management of erysipelas
Treatment of erysipelas is usually for 10–14 days with antibiotic therapy, either orally or intravenously dependent on how unwell the patient is. Most streptococcal bacteria causing erysipelas are sensitive to penicillin with erythromycin being used as a second choice in those with penicillin allergy. Signs of systemic illness usually resolve within a few days; however, the skin changes may take a number of weeks to settle. Usually no scarring occurs. Antimicrobial coverage for S. aureus is not generally required but it should be considered in those who do not improve with penicillin. Erysipelas can recur in up to one-third of patients due to ongoing risk factors and impaired drainage of toxins due to lymphatic damage caused by the initial infection.
Necrotizing fasciitis
Necrotizing fasciitis is a serious soft tissue infection of the deeper layers of the skin and subcutaneous tissues, spreading across the fascial plan and destroying the soft tissues. It is an important infection with a high mortality, with the bacteria gaining entry through a break in the skin's integrity. The most common causes are Group A Streptococci (Streptococcus pyogenes) and S. aureus.
‘Type 1’ necrotizing fasciitis is a polymicrobial infection usually including both Gram-positive and Gram-negative organisms together with anaerobes. This type usually occurs in areas where the body is colonized by faecal flora, affects the abdominal wall or affects patients with leg ulcers and poor general health. It may initially be mistaken for a simple wound cellulitis. Severe pain and systemic toxicity demonstrate widespread tissue necrosis underlying what appears to be viable skin.
‘Type II’ necrotizing fasciitis describes a monomicrobial infection usually with Group A Streptococci. In recent years, MRSA is increasingly being seen.
‘Type III’ necrotizing fasciitis or gas gangrene is caused by Clostridium perfringens. It usually follows significant trauma or surgery and results in crepitus under the skin. Initially, the patient presents with pain over the area of injury, worsening over time. Patients may have flu-like symptoms that develop into septicaemia. Later, the affected area begins to swell and show a purplish rash, with blisters developing. The skin then starts to turn black due to necrosis. Crepitus may be evident (see Fig. 11).
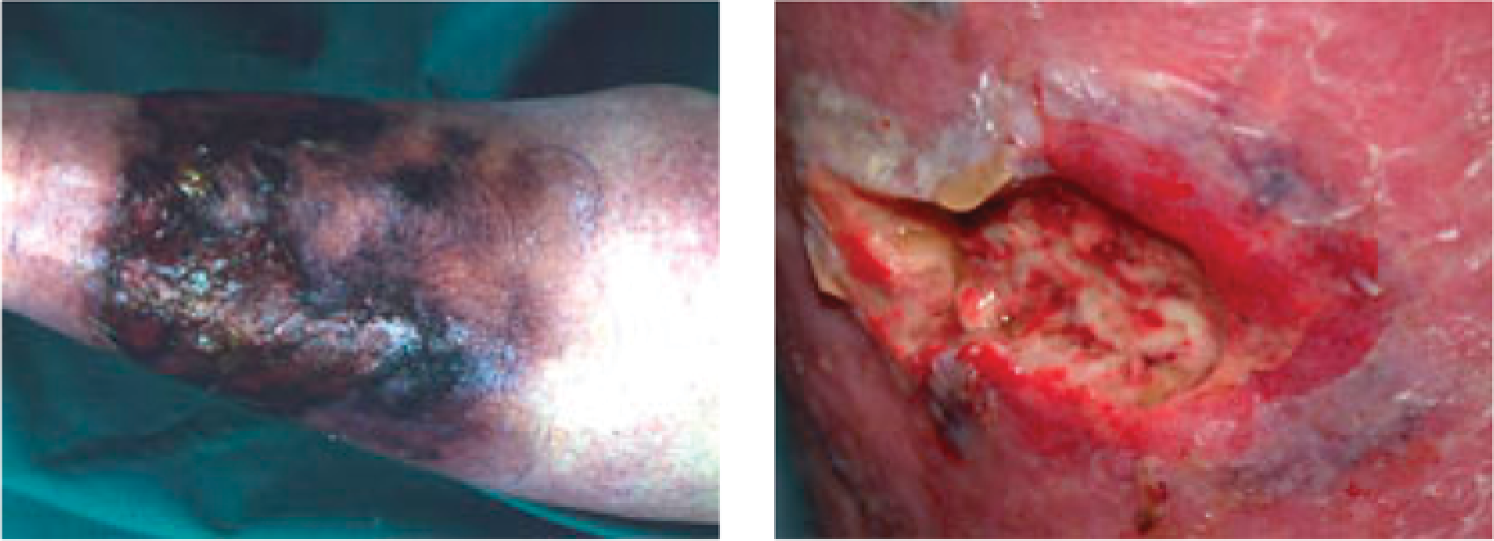
Necrotizing fasciitis.
Determining necrotizing fasciitis from cellulitis is essential. Features such as severe pain, rapid progression, poor therapeutic response, blistering necrosis and signs of systemic toxicity suggest a diagnosis of necrotizing fasciitis.
Management of necrotizing fasciitis
Prompt diagnosis and treatment are essential to reduce the risk of death and disfigurement from necrotizing fasciitis. Admission to hospital for early surgery and debridement of necrotic tissue are vital for survival. Necrotizing fasciitis has a high mortality with up to 25% of patients dying as a result of the condition or its complications.
Methicillin-resistant S. aureus
Staphylococcus aureus colonizes approximately one-third of the healthy population, causing no harm. MRSA are varieties of S. aureus that have developed multiple antibiotic resistances, including resistance to the antibiotic methicillin. MRSA is rarely acquired in the community. Usually, however, it is acquired in the hospital setting but may then be taken home by patients. The proportion of the general population colonized with MRSA is 3%; this increases in hospitalized patients as a result of greater exposure to the bacteria.
Infection with hospital-acquired MRSA tends to occur in the elderly, those who are chronically ill or those with open wounds, such as those undergoing surgery or patients with skin breakdown. Significant problems can occur if MRSA skin infections develop, as although MRSA is no more virulent than other forms of S. aureus, infections resulting from MRSA can be difficult to treat as there are a very limited range of effective antibiotics available.
If MRSA skin infection is suspected because a patient has been recently hospitalized or is known to be colonized with MRSA, it is important to obtain a swab from the infected skin lesion for microscopy, culture and sensitivity. For patients with minor skin infections (e.g. folliculitis), systemic antimicrobial therapy is not advised but consider skin antiseptics or topical fusidic acid cream.
If a patient has a large abscess (greater than 5 cm diameter), is systemically unwell or develops any surrounding cellulitis, systemic antibiotic treatment should be commenced. Empirical antibiotic treatment for suspected S. aureus infection is flucloxacillin 500 mg to 1 g four times daily for 5–7 days (or clindamycin in those with penicillin allergy). If MRSA is strongly suspected based on the patient's history or detected on swabs, then contact your local microbiology department for advice before commencing treatment.
Key points
Bacterial skin infections are a common presentation to primary care. Knowledge of their presentation and management is essential.
Individuals with a history of skin trauma, chronic skin conditions, obesity, poor general health and nutrition, pregnancy, diabetes, chronic venous insufficiency and those who are immunocompromised have an increased risk of developing bacterial skin infections
The most common pathogens implicated in bacterial skin infection are S. aureus and Steptococcus pyogenes
S. aureus is mainly implicated in the development of folliculitis, furunculosis, impetigo, ecythma and SSSS
Streptococcus pyogenes is the main causative agent in cellulitis, erysipelas, impetigo and necrotizing fasciitis
MRSA skin infections can be difficult to treat, contact your local microbiology department for advice
Footnotes
Acknowledgements
All photographs within this article are reproduced with permission from DermNet NZ, the website of the New Zealand Dermatological Society Incorporated.