
Abstract
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia encountered in clinical practice. Its prevalence increases with age and is estimated at around 5% in those aged 65 years, rising to 10% in the over 80 population. AF usually arises from the left atrium and is commonly referred to as a ‘supraventricular arrhythmia’. It is characterized by rapid, irregular and chaotic electrical atrial activity that results in an irregular ventricular response. AF is no longer considered a benign condition as it is associated with significant morbidity and mortality, most notably from its 5-fold increased risk of stroke. With an ever-increasing elderly population, it is unsurprising that AF poses a significant public and health burden and already accounts for about 1% of the National Health Service (NHS) expenditure.
The GP curriculum and atrial fibrillation
RCGP
be able to elicit appropriate signs and symptoms have knowledge of subsequent investigation and/or referral of people presenting with palpitations and silent arrhythmias have knowledge of the acute treatment of people presenting with cardiovascular problems or symptoms thought to be due to cardiovascular problems
Specific relevant problem-solving skills that GPs should have are to be able to:
urgently intervene when patients present with a cardiovascular emergency demonstrate an understanding of the importance of risk factors in the diagnosis and management of cardiovascular problems and demonstrate a reasoned approach to the diagnosis of cardiovascular symptoms using history, examination, incremental investigations and referral
Aetiology of AF
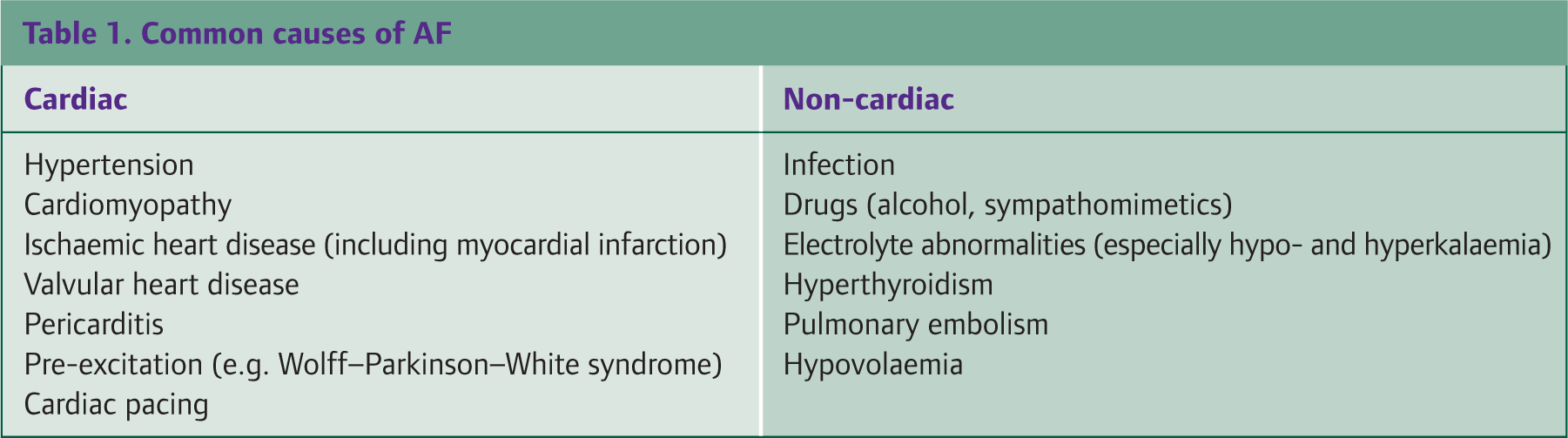
AF is associated with a number of cardiac and non-cardiac causes (Table 1). It is more common with advancing age and causes frequently encountered in general practice include hypertension, ischaemic heart disease, cardiomyopathy, valvular heart disease, drugs (particularly alcohol), thyrotoxicosis, infection and electrolyte disturbance. In approximately 12% of patients an underlying cause is not found and such cases are referred to as ‘lone AF’.
Common causes of AF
Classification
Various systems have historically been used to classify AF. It is now common practice to describe AF in relation to its pattern of occurrence: paroxysmal, persistent or permanent. AF may also be referred to as being acute in patients presenting with the sudden onset of symptoms or non-acute depending on the duration of symptoms (Table 2). Paroxysmal AF describes recurring episodes with a tendency to spontaneously revert to sinus rhythm and patients often experience repeated symptoms in conjunction with this. Persistent AF is of longer duration and requires treatment to terminate the arrhythmia. These patients present with symptoms of variable duration and severity. Permanent AF is longstanding AF in which attempts to restore sinus rhythm have failed or have not been attempted for clinical reasons.
Classification of AF

The burden of AF
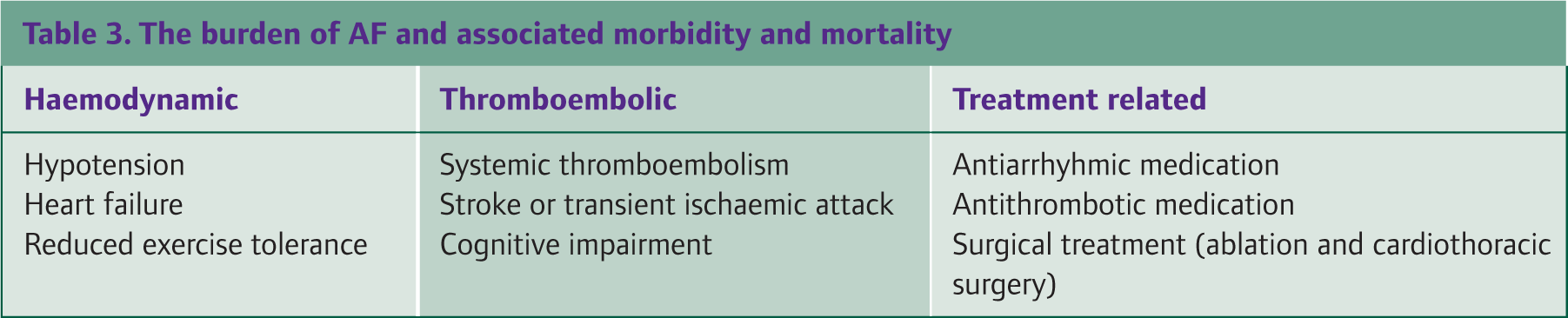
AF is associated with significant morbidity and mortality. This results from a combination of its immediate haemodynamic effects, its thromboembolic risk and the burden of treatment (Table 3). The symptoms of AF can be debilitating for some patients with an associated reduction in quality of life and increased hospitalization. The management of AF is also not without risk. Some patients experience problems from the treatments used and their monitoring (particularly warfarin), which will be discussed later in this article. The potential difficulties of pharmacotherapy are usually justified, however, by the greater benefits of treatment in reducing long-term complications such as peripheral thromboembolism (notably stroke), cardiac failure and the perpetuation of AF. Of note, it is estimated that AF is present in up to 15% of patients presenting with acute stroke.
The burden of AF and associated morbidity and mortality
Clinical features
Symptoms
The symptoms of AF are highly variable and are influenced by the rapidity of the heart rate and the patient's underlying cardiac function. Often patients present with vague complaints and it can be very difficult to ascertain the onset of AF. Recognized symptoms (in order of decreasing frequency) include: palpitations, breathlessness, fatigue, syncope/dizziness and chest pain. It is estimated that around 11% of patients with AF are asymptomatic and are identified incidentally during clinical review for other reasons.
Signs
The hallmark and sometimes only clinical finding on examination in AF is that of an ‘irregularly irregular pulse’. This description refers to irregularity of the rate, rhythm and volume that results from the conduction of chaotic atrial activity into the ventricles. The heart rate can be fast, normal or slow in AF and it is well recognized that the radial pulse may underestimate the rate due to an apical-radial delay. Therefore, the clinical finding of an irregular radial pulse should be confirmed by the palpation of a central pulse, such as the carotid or subclavian pulse.
Sometimes an otherwise asymptomatic patient may present with erratic home blood pressure and heart rate recordings. This often reflects the presence of AF and not a fault of machinery. Due to the difficulties in identifying AF on symptoms alone, it has been suggested that routine opportunistic pulse checks should be performed in general practice to improve the identification of this highly prevalent condition.
Once AF is suspected clinically, further assessment should be made to identify coexisting risk factors, underlying aetiology and complications (Table 4). In the context of AF presenting acutely, in addition, it is prudent to assess for signs of haemodynamic compromise as such patients should be referred to secondary care for emergency treatment.
possible clinical findings in association with AF

JVP = jugular venous pressure, BMI = body mass index, DVT = deep vein thrombosis.
Investigations
Every patient with suspected AF should have a 12-lead electrocardiogram (ECG) to confirm the diagnosis. However, patients with paroxysmal AF may require 24 hour ambulatory ECG or 7 day Holter monitoring if their initial ECG is normal.
Figure 1 shows an ECG with characteristic features of AF. There is an absence of P waves (indicating the absence of organized atrial activity) and irregularly occurring QRS complexes (reflecting a subsequent irregular ventricular response). Common coexisting features on the ECG suggesting other conditions associated with AF include conduction abnormalities (such as bundle branch blocks), changes from previous myocardial infarction (such as Q waves) and changes suggestive of underlying hypertension such as ventricular hypertrophy.
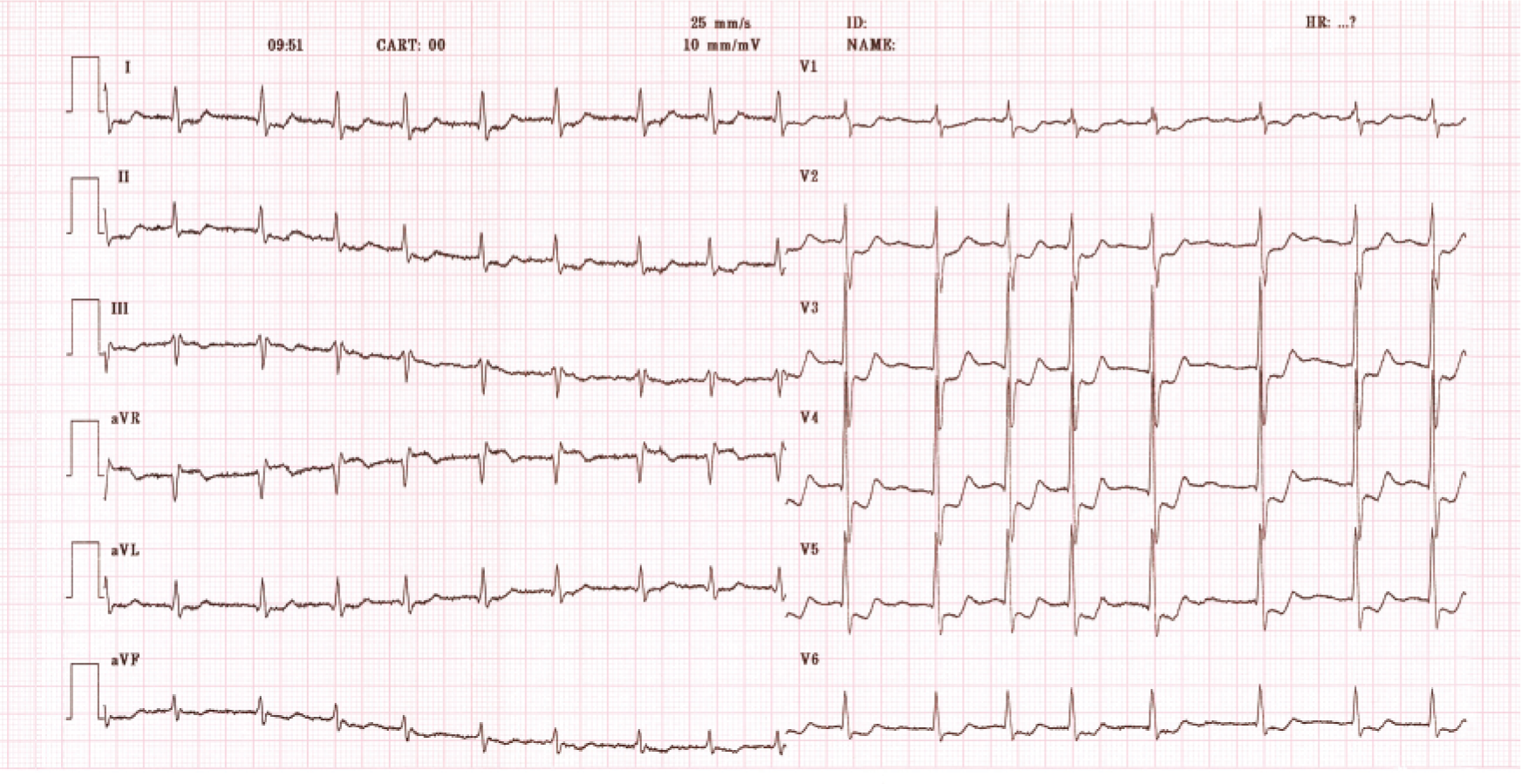
ECG features of AF (absence of atrial activity or ‘P’ waves and irregularly occurring QRS complexes)
All patients should then have a series of baseline tests (Table 5). Additional investigations may be warranted but vary according to the individual's presentation, aetiology and complications.
Baseline investigations for AF

Principles of treatment
The management of AF is often perceived as complex and confusing. Much of this confusion arises from the differences in the management of acute AF and non-acute AF. Those with acute AF may be at significant risk of rapid deterioration and therefore this group must be differentiated early on to enable prompt safe emergency treatment. For both groups, the management strategy used should be in conjunction with assessment and modification of risk factors for AF.
Acute AF
Patients with acute AF will usually have a clear onset of symptoms. The first priority is to decide whether the patient requires emergency treatment in hospital. This is achieved by identifying those patients who are unwell (or haemodynamically unstable) from those who are well (or haemodynamically stable). The former group requires emergency treatment and consideration for direct current cardioversion (DCCV). The role of immediate DCCV in acute unstable AF is to restore a normal cardiac rhythm and haemodynamic function, thereby preventing further clinical deterioration.
Unless they require emergency admission for immediate assessment of the arrhythmia and underlying precipitating cause (such as myocardial infarction), haemodynamically stable patients without complications from the AF can be managed as outpatients, either pharmacologically or with DCCV as a day-case procedure. Treatment of reversible underlying causes, such as infection or electrolyte disturbance, should be managed accordingly in conjunction with antiarrhythmic medication (Fig. 2).
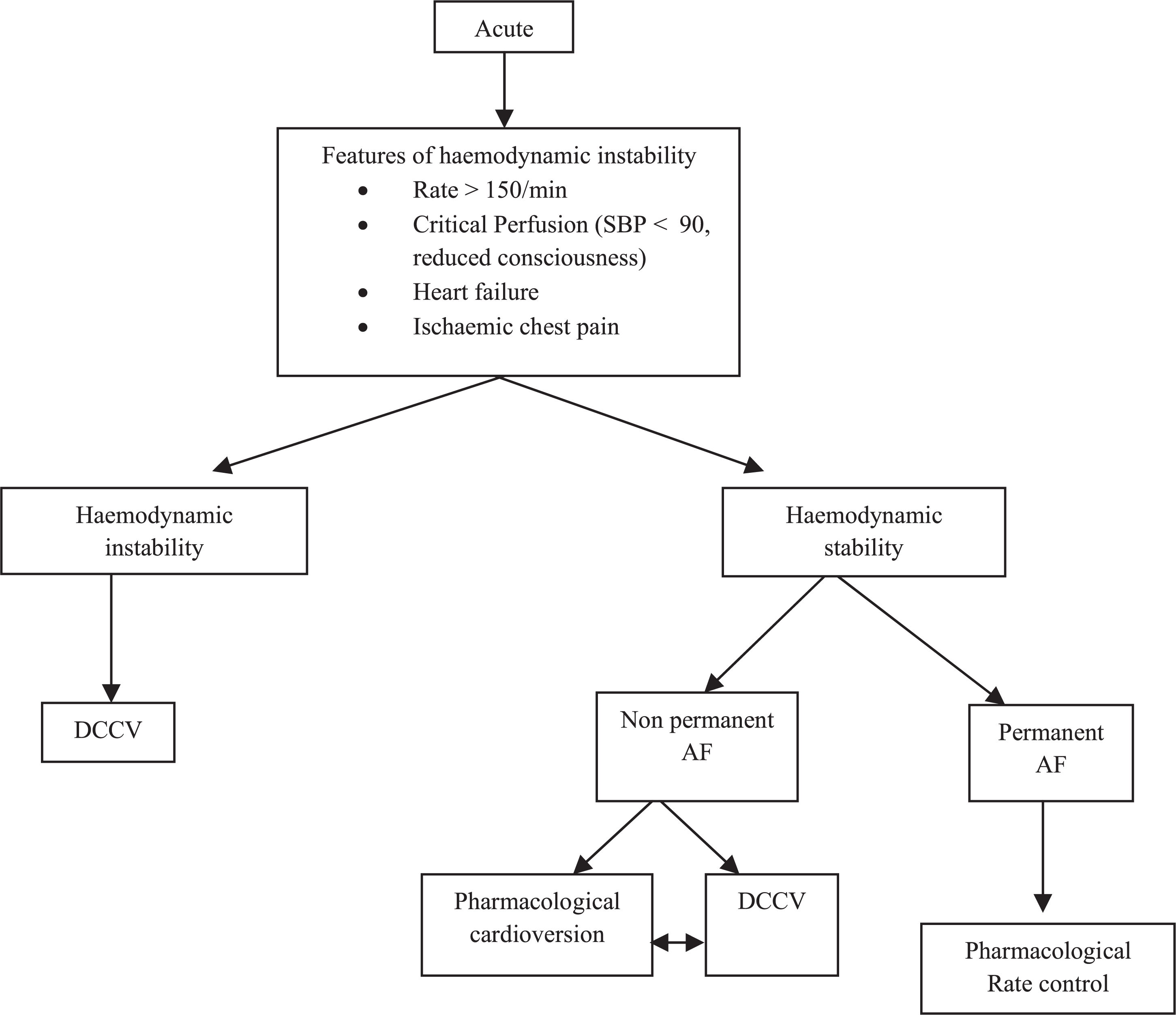
Emergency management of AF
Non-acute AF
The aims of managing non-acute AF are as follows:
treatment of the arrhythmia to provide symptomatic relief treatment of risk factors and underlying causes for AF the prevention of complications (in particular stroke)
Arrhythmia management
The control of non-acute AF may involve pharmacological or surgical therapy, the latter falling into the domains of secondary and tertiary care. Pharmacological strategies usually involve the prescription of antiarrhythmic drugs (AADs) and emphasis is placed upon a rhythm-or rate-control strategy.
Antiarrhythmic strategies
In recent years, there has been much debate regarding the optimal way to treat AF: the rate-versus rhythm-control dilemma. With the publication of large multicentre randomized control trials (RCT) and national guidelines it has become more widely accepted to adopt a rate-controlling strategy first. This is because rate-controlling drugs tend to be better tolerated by patients and have safer side effect profiles. Indeed, there is increasing evidence that long-term mortality is the same whichever strategy is used, further supporting the rate-controlling approach. However, the National Institute for Health and Clinical Excellence (NICE) guidelines recognize the importance of rhythm control as a first-line measure in certain subgroups of patient:
the young or those with lone AF—to prevent the development of lifelong AF those with structural heart disease or cardiac failure—to maintain cardiac function those with recurrent paroxysms of AF—to prevent recurring debilitating symptoms
It is therefore important to decide treatment on an individual basis, still considering those who may benefit from rhythm control over rate control (Fig. 3). It is also worth noting that some patients (particularly the elderly) who are both asymptomatic and have AF with a normal rate can be managed without antiarrhythmic medication and emphasis is then placed upon preventing complications, such as stroke.

Treatment strategy decision tree for AF (National Collaborating Centre for Chronic Conditions, 2006).
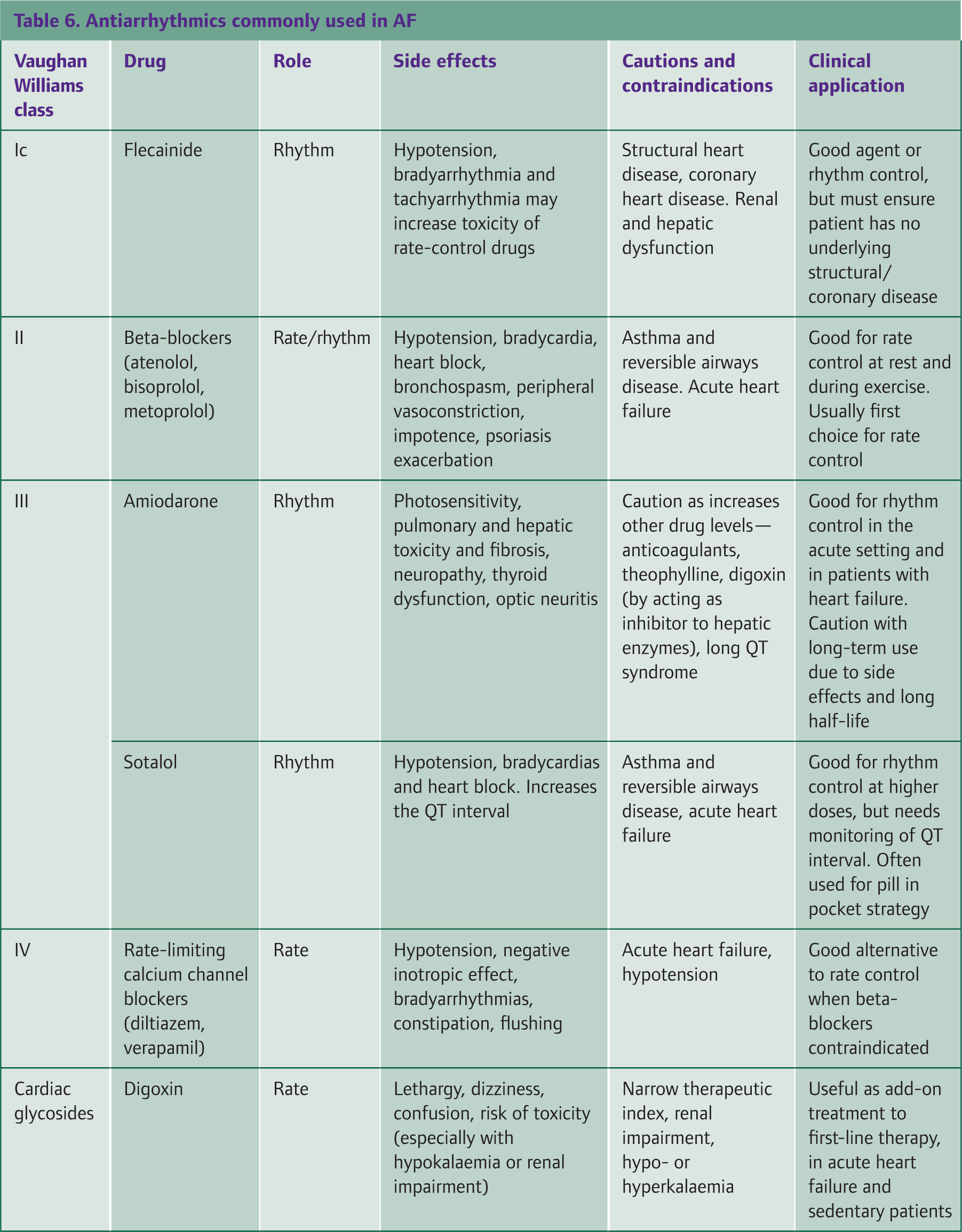
Once the clinician has decided whether to initiate a rate-or rhythm-control strategy, it is then necessary to decide which therapy to prescribe and in doing so, carefully consider each patient individually, balancing the benefits with the possibility of side effects from the chosen medications (Table 6).
Antiarrhythmics commonly used in AF
Rate-control therapies
There are three commonly used groups of drugs for rate-control therapy:
beta-blockers calcium channel blockers digoxin
The choice of drug used is dependent on a number of factors including co-morbidity, tolerability and personal preference. Optimal rate control is considered to be 60–80 beats per minute at rest and 90–115 beats per minute during exercise. Beta-blockers or calcium channel blockers are generally first-line treatments and digoxin should be used as an adjunct if first-line therapy is insufficient. Digoxin monotherapy should be reserved for those patients who have contraindications to first-line drugs, those presenting with acute heart failure and those with a sedentary lifestyle (e.g. immobile elderly patients). This is because digoxin has poor rate-controlling properties in states of high sympathetic output (i.e. exercise).
Rhythm-control therapies
Rhythm-control is a strategy aimed at restoring sinus rhythm. This can be achieved by pharmacological treatment, elective DCCV or surgical therapies. Patients requiring elective DCCV or surgical management should be under the long-term care of a cardiologist.
Patients with paroxysmal AF may be managed using long-term prophylactic antiarrhythmics but some individuals prefer a ‘pill in the pocket’ approach where they self-medicate with an AAD. The latter strategy is acceptable should the paroxysms be of a short or infrequent duration and providing there is no underlying structural or valvular heart disease. As for rate-controlling therapies, the choice of drug depends upon the presence of structural cardiac abnormalities, co-morbidity and patient factors such as tolerability.
Commonly used drugs to achieve rhythm control include flecainide, sotalol and amiodarone although beta-blockers are often used as first-line agents as they also share rhythm-stabilizing properties. Despite many of these medications being initiated by secondary care physicians, a GP may encounter these therapies during long-term follow-up and should have an awareness of their management.
Patients who are managed by elective DCCV are often managed with coexisting drug treatment, as this controls symptoms prior to DCCV and maintains sinus rhythm afterwards. It is also worth noting that these patients require anticoagulation to have been therapeutic for at least 3 weeks prior to DCCV (to prevent procedural thromboembolism).
Over recent years there have been new developments in the surgical approach to managing AF refractory to conventional treatment. Electrophysiological mapping and ablation of the arrhythmia is one such available therapy provided by cardiologists, with pulmonary vein isolation (PVI) being one of the more common techniques used. Cardiothoracic surgery also has a role using techniques such as the ‘maze procedure’ although this is reserved for patients who require open-heart surgery for other reasons (such as valve replacement).
Prevention of complications
Antithrombotic management
The increased atrial thrombus formation associated with AF is one of the main pathophysiological mechanisms behind its thromboembolic complications. It is well established that thromboprophylaxis in patients with AF is beneficial but the risk of stroke is not homogeneous for all patients and therefore patients need to be ‘risk stratified’ and managed accordingly. Various risk stratification models have previously been described and incorporate conditions associated with a greater probability (or risk) of stroke. Only after this risk is estimated can decisions regarding the appropriate treatment be made. The NICE risk stratification scheme has become widely adopted in the UK and categorizes patients into low-, moderate-and high-risk groups (Fig. 4). The following conditions are recognized by NICE as significant predictors of risk:

Stroke risk stratification algorithm (National Collaborating Centre for Chronic Conditions, 2006). *Coronary or peripheral artery disease. **An echocardiogram is not mandatory for stroke risk stratification, but does refine risk in cases of moderate and severe left ventricular impairment and valve disease.
Increasing age (particularly those over 75 years) Previous ischaemic stroke, transient ischaemic attack (TIA) or thromboembolic event Hypertension Diabetes Vascular disease Cardiac failure (either clinical or echocardiographic) or significant valve disease
The management of AF presenting acutely with haemodynamic compromise requires prompt treatment of the arrhythmia and this takes precedence over thromboprophylaxis. NICE recommends risk stratifying all other patients in the same way despite the pattern of AF occurrence (paroxysmal, persistent or permanent).
Antithrombotic therapy involves the use of antiplatelet agents (aspirin or clopidogrel) or anticoagulants (warfarin). It is recommended that patients who are in the low-risk group are treated with aspirin (75–300 mg daily) as the first-line antiplatelet. Should aspirin be contraindicated, clopidogrel (75 mg daily) should be used instead. Patients in the high-risk group should be started on warfarin therapy [to achieve a target international normalized ratio (INR) of 2.5 with a range of 2.0–3.0] providing there are no contraindications. If warfarin therapy is deemed inappropriate, then antiplatelet therapy should be considered as an alternative. Patients in the moderate risk group can be treated with either warfarin or aspirin, with careful consideration to the risks and benefits of each option. In recent years, there has been a trend towards the greater use of warfarin in patients at moderate risk of stroke. There is no benefit from using dual antiplatelet therapy as evidence shows that combining antiplatelets is inferior to warfarin by increasing the risk of harmful outcomes, in particular bleeding.
Certainly warfarin is not without its own risks. In addition to the difficulties of monitoring and interaction with food and drugs, warfarin is associated with an increased risk of bleeding. Despite the majority of bleeding events being classed as minor (bruising or longer bleeding times), particular attention is drawn to life-threatening events (gastro-intestinal and intracranial haemorrhage), the risk of which in appropriately selected patients is small.
Much of this concern relates to the risk associated from falls, but evidence also suggests that a patient would need to fall daily before the risk of bleeding from warfarin outweighs its benefits. Factors that have been shown to convey a greater risk of bleeding include:
Age over 75 years Concomitant treatment with antiplatelets or non-steroidal anti-inflammatory drugs On multiple other drug treatments Poorly controlled hypertension Past history of bleeding problems (such as peptic ulcer disease or cerebral haemorrhage) Previous history of poorly controlled anticoagulation therapy
Therefore, it is essential to assess bleeding risk as part of clinical assessment before starting a patient on anticoagulation therapy taking into consideration the factors listed above. Once initiated, patients need to have good compliance with treatment and tolerate regular monitoring to achieve stable INRs. Consequently, it is not surprising that the time immediately after starting warfarin is the most dangerous time and good clinical governance should be in place.
New and novel therapies that overcome the problems with anticoagulation monitoring are under development, such as the direct thrombin inhibitor dabigatran. With initial promising results in clinical trials (which show dabigatran to be as effective as warfarin in stroke prevention but having fewer bleeding events), this therapy remains under investigation.
When to refer
Some patients with AF require the involvement of a wider multidisciplinary team and are often referred to a cardiovascular specialist in secondary care. It is important to recognize certain groups that would benefit from shared care and refer promptly.
Patients who are acutely unwell require immediate admission and are usually referred to the relevant team via the emergency department Patients with coexisting causes for AF that need further investigation and treatment should be referred to the appropriate subspecialist. Examples of such patients include those with coronary heart disease, significant valvular heart disease, cardiomyopathy or thyrotoxicosis. Additionally, patients who have poor control of their AF require shared care as such patients may require multiple AADs, elective DCCV or even a surgical approach to their treatment
Key points
AF is the most commonly encountered arrhythmia and with an increasingly aged population its prevalence is expected to rise AF is associated with significant morbidity and mortality most notably from its 5-fold increased risk of stroke Although patients with AF can present with multiple and varying symptoms, a significant proportion of patients are asymptomatic. A GP must therefore have a low threshold for performing a routine opportunistic pulse check to improve the identification of this highly prevalent condition. Treatment of AF involves three important domains: controlling the arrhythmia, managing risk factors and causes of AF and preventing complications (especially stroke) Arrhythmia treatment involves control of the rate or the rhythm. However, it is important to remember that some patients may not require treatment. Stroke risk stratification models should be used to assess the risk of stroke. After assessment of bleeding risk, antithrombotic treatment (either aspirin or warfarin) should be initiated safely.