
Abstract
This article aims to highlight the delivery of health care to people with learning disabilities (PWLD) in the context of new Department of Health guidance and implementation of the Mental Capacity Act (2005). We seek to identify a myriad of barriers to health care delivery in this population and look at strategies to tackle these barriers. We will also consider the issue of capacity, which is particularly important for PWLD. We will highlight the importance of recognizing this population's enhanced baseline medical morbidity and how a best interests team approach is optimal when targeting interventions.
The GP curriculum and learning disability
Demonstrate an awareness of the issues of capacity and consent and the mechanisms by which these can be determined
Demonstrate respect for the patient's autonomy, which may be limited, and an awareness of how communicating via carers may skew the doctor-patient relationship
Demonstrate an understanding of how health can be overlooked in PWLD
Describe the associated medical problems in commonly encountered conditions that make up learning disabilities
Describe the roles of paid carers, respite care opportunities, voluntary and statutory agencies and an ability to work in partnership with them so there is cooperation without duplication
Demonstrate an understanding that all citizens should have equal rights to health and equitable access to health and health information according to their needs
Demonstrate an understanding that PWLD are more prone to the effects of prejudice and unfair discrimination
Demonstrate an awareness of the evidence regarding the health needs of PWLD
Demonstrate an understanding of the importance of developing and maintaining continuing learning on physician-based issues that are barriers to health care for PWLD
Background
It is estimated that 2.5% of people in the UK have a learning disability, although wide variations of between 0.6 and 2.5% have been reported. In a typical general practice population of 12 000 patients, this equates to a total of 300 patients, the majority of whom have mild learning disability with only a minority formally diagnosed. The level of learning disability is based on a person's intelligence quotient (IQ) and broadly corresponds to his or her level of functioning (outlined in Table 1).
Level of learning disability

The provision of quality health care to PWLD is a national priority; the emphasis on this is highlighted by the government's recent good practice guidance on health facilitation and planning for PWLD (Department of Health, 2008) and the Royal College of General Practitioners curriculum dedicating an entire chapter to highlighting the health needs and concerns of PWLD.
The Department of Health white paper, Valuing people (2001), highlighted the significantly higher psychiatric and physical co-morbidities of PWLD; the paper also highlighted the inconsistent and suboptimal level of health care provision. A follow-up government white paper, Valuing people now (2009), recommended supporting Primary Care Trusts (PCTs) with a new primary care service framework to commission better primary care access for PWLD. It also recommended a national awareness and education programme for the National Health Service (NHS) regarding the Disability Equality Duty: a duty for public bodies to promote equality for disabled people in every area of their work.
A formal investigation into medical treatment of PWLD, Equal treatment (2006), has been reported by the Disability Rights Commission. It described the barriers to primary care and screening initiatives experienced by PWLD. Their findings suggested a need for targeted action and leadership to tackle the marked health inequalities experienced by PWLD. It was suggested that regular health checks would help address the significant health care needs of PWLD, particularly in relation to cerebrovascular disease and diabetes.
An independent enquiry into access to health care for PWLD, Healthcare for all (Department of Health, 2008), delivered a critical account of the unequal care received. The report highlighted how ‘reasonable adjustments’ such as an annual health check, assistance with visits to hospitals and better information and help with communication would all help to tackle the inequalities in access and outcomes from the health service. The report suggested that the expected ‘equality’ of care for all citizens did not necessarily mean the ‘same’ care, especially if giving the ‘same’ care to patients with learning disabilities would be unsatisfactory. However, the acceptance of suboptimal care for PWLD being endemic within the NHS is by no means universal with critical voices questioning these findings (Fitzpatrick, 2008).
In 2009, a nationally agreed Directed Enhanced Service was introduced nationally for GPs, which incentivized annual health checks for PWLD. An enhanced service for annual health checks had been operating in Wales since 2006 and the recipients had valued the opportunity and appreciated the importance of these checks (NPHS/WCLD Project Group, 2009).
Barriers to care and practical considerations
A variety of different reasons have been suggested as to why PWLD face challenges in receiving quality health care. It was noted by Healthcare for all (Department of Health, 2008) that a small minority of people are not registered with a GP, and while the number of people was small, the barrier to health care encountered due to this was large.
Communication difficulties, sensory impairment, reliance on others to voice health care needs and negative professional attitudes have all been highlighted. PWLD may see multiple health care professionals, including GPs and psychiatrists. Professionals may incorrectly assume that a particular medical concern is being dealt with by a colleague, when in fact that colleague is of the same belief, leading to a lack of responsibility (Mackin et al., 2007). PWLD also have a variety of medical health issues linked directly with the aetiology of their learning disability, such as epilepsy (Sivakumar, 2007). Autistic spectrum disorders (ASD) are also linked to learning disability although the relationship is not entirely clear. What is evident, however, is that PWLD with co-morbid ASD face even greater challenges given the lack of resources and facilities facing people with ASD and their carers.
Diagnostic overshadowing is an important concept in PWLD. It arises when potentially treatable physical and psychiatric conditions are falsely attributed to the underlying learning disability. This may deny patients the standard of health care they would receive if they did not have a learning disability.
Case study 1
Adam is a 34-year-old man with moderate learning disability. He lives in a private residential home with 24 hour carers. He is brought to surgery on a Monday morning because the residential home staff have noticed that Adam is more agitated than usual and that he has started hitting the side of his head during the weekend.
The carer who accompanies Adam to the surgery, who is new to the home, requests more as required diazepam medication to help ‘calm him’ and mentions ‘Adam gets like this sometimes’.
The GP, noting Adam's history of recurrent otitis media, shows Adam an otoscope and demonstrates its use on the carer. The GP performs an otoscopic examination on Adam and diagnoses a left-sided otitis media. As Adam has a history of recurrent otitis media and usually requires antibiotics to settle these infections, an antibiotic and analgesia are prescribed and a follow-up appointment is arranged.
At follow-up, the carer notes that Adam settled shortly after his first dose of regular analgesia and no further head banging was noted. The GP notes that the otitis media has resolved.
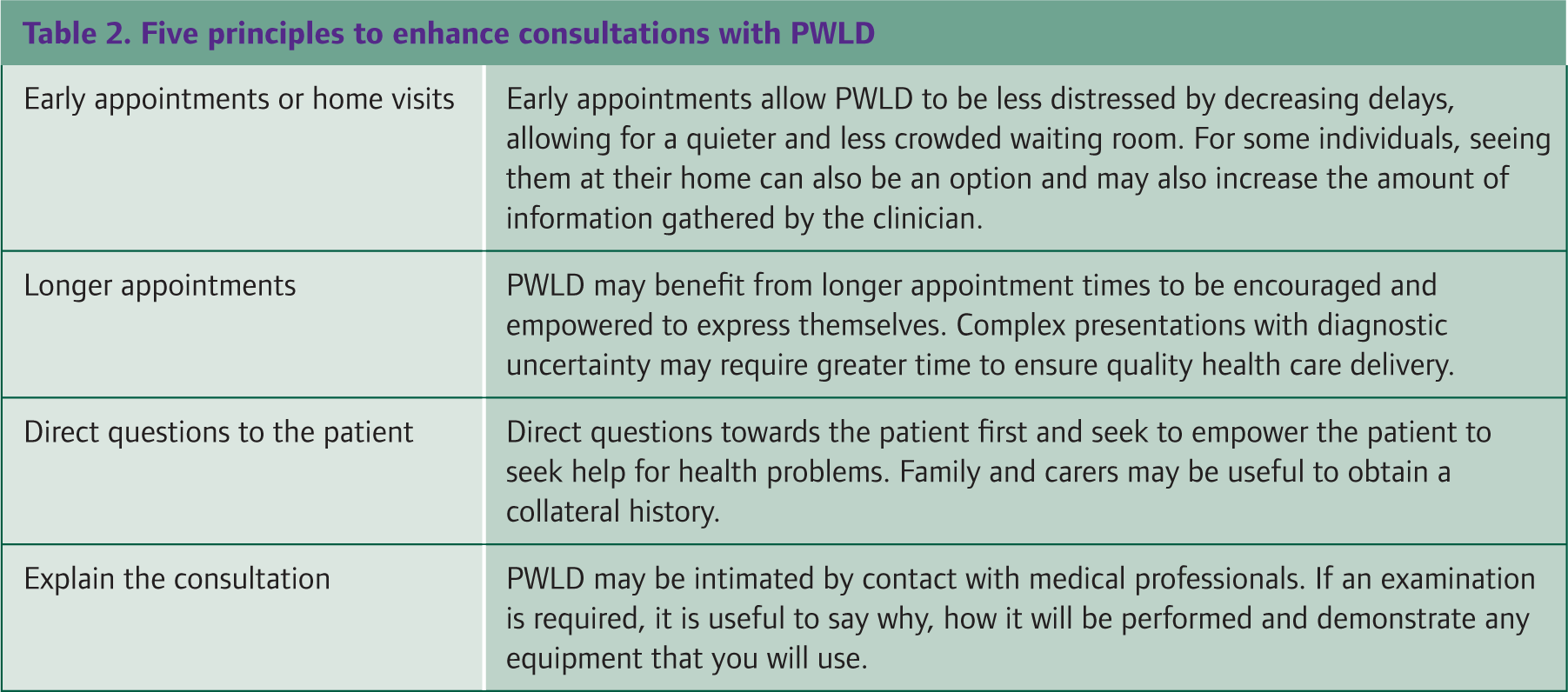
Despite the many potential barriers to obtaining health care, there are several principles that can be employed before and within a consultation to improve health care delivery in PWLD. These points are outlined in Table 2.
Five principles to enhance consultations with PWLD
Antipsychotic drug use
A challenge to the health and well-being of PWLD is the high rate of antipsychotic drug use, largely for challenging behaviour. Challenging behaviour is a broad term but may encompass physical aggression, self-injury, destructive behaviour, verbal aggression and sexually inappropriate behaviour.
It has been reported that up to 45% of PWLD in hospital and 20% in the community will be receiving antipsychotic drugs (Ashcroft et al., 2001). Unfortunately, these antipsychotic medications carry a variety of risks. Of particular concern are the associated metabolic disturbances that include weight gain, diabetes and impaired glucose tolerance and adverse lipid profile (Tschoner et al., 2007). PWLD have both increased baseline morbidity and decreased health care access.
Combined with adverse metabolic side effects as a result of a high prevalence of antipsychotic medication use, PWLD benefit greatly from close health monitoring. In particular, people using antipsychotic medication, regardless of intellectual function, should undergo metabolic monitoring.
Assessment of capacity
The issue of capacity is a central concept when dealing with this patient group. Previously in institutional settings there was a paternalistic attitude towards the health care and routines of PWLD. The move towards care in the community and the implementation of the Mental Capacity Act (2005) have led to greater empowerment. PWLD who have capacity may now experience the autonomy enjoyed by the general population with regard to lifestyle and health care choices.
The five principles of the Mental Capacity Act (2005) with a focus on PWLD are as follows:
A presumption of capacity—every adult must be assumed to have capacity unless proved otherwise. The fact that someone has a learning disability or a mental illness should not lead to an assumption of inability to make decisions.
The right to be supported to make decisions— depending on the severity of learning disability, PWLD may have some ability to communicate whether it is through vocabulary, non-verbal gestures or sign language (e.g. Makaton). Every effort must be made to enable and support PWLD to make decisions and communicate them effectively.
Individuals must not be judged unable to make a decision merely because their decisions are seen as eccentric or unwise. It is not necessary for people involved in the care of PWLD to agree with the individuals' decisions.
Best interests—when decisions are taken on behalf of people without capacity they must be in their best interests. This may be achieved by holding a best interests meeting.
Less restrictive alternative—before decisions are taken or acts performed, it is important to consider whether an acceptable outcome can be achieved in a way that is less restrictive of the person's rights and freedom of action.
Useful websites and resources

However, there is some controversy over the concept of capacity in PWLD. Hasan et al. (2006) suggested that PWLD may have greater difficulty relating to understanding the concept of risk and future ill health, and that if we need to act in their best interests, we need not only to use the traditional best medical interests model, but to incorporate social, psychological and even spiritual considerations.
It has been recognized that PWLD may at times lack capacity to make certain health care decisions. It is then a priority for the health care team to act in the patient's best interests. For PWLD who are deemed not to have capacity to make a decision regarding a particular issue, a best interests meeting can be arranged. Any person who is involved in the care of an individual lacking capacity may call the meeting, including GPs, nurses and hospital consultants. The meeting is in the form of a discussion, which aims to reach a consensus or majority decision regarding health care choices for that individual. The meeting takes into account people's opinions, beliefs and the risks and benefits of any intervention.
Enough emphasis cannot be placed on the importance of assessing capacity, making team decisions either in their best interests or in partnership with individuals with capacity. Useful websites that may help you manage PWLD in your surgery are listed in Box 1.
Key points
Over 2% of the population have a learning disability
PWLD have higher psychiatric and medical comorbidity
PWLD suffer from many barriers to obtaining adequate health care, including reduced access and suboptimal medical care
Improving access and quality of health care for PWLD is a Royal College of General Practitioners and a Department of Health priority.
The Mental Capacity Act outlines key principles around the issue of capacity. Understanding capacity is vital when dealing with people who have a learning disability.