
Abstract
This competence is about maintaining the performance and effective continuing professional development of oneself and others.
Over the next four articles we will deal with how GPs manage themselves sufficiently to maintain performance.
Maintaining our medical performance is no different to maintaining our physical or mental performance. Think of it as ‘health promotion’ but with the added dimension that we are doing it partly for ourselves but mostly because others may come to harm if we do not.
What does this mean in practice? Performance, like health promotion, is not just about having good intentions; anyone can give up smoking once they have been told they have lung cancer. Maintaining performance is about respecting its importance to those dependent upon us, having the commitment to do something regularly and having a mechanism for doing so.
The mechanism is vital because it underpins performance. This section is part of the ‘Management’ section of this book because it concerns our ability to manage ourselves by monitoring our performance, learning and development in all relevant areas and therefore maintain the capacity to keep working throughout our careers at a sufficiently effective and safe level.
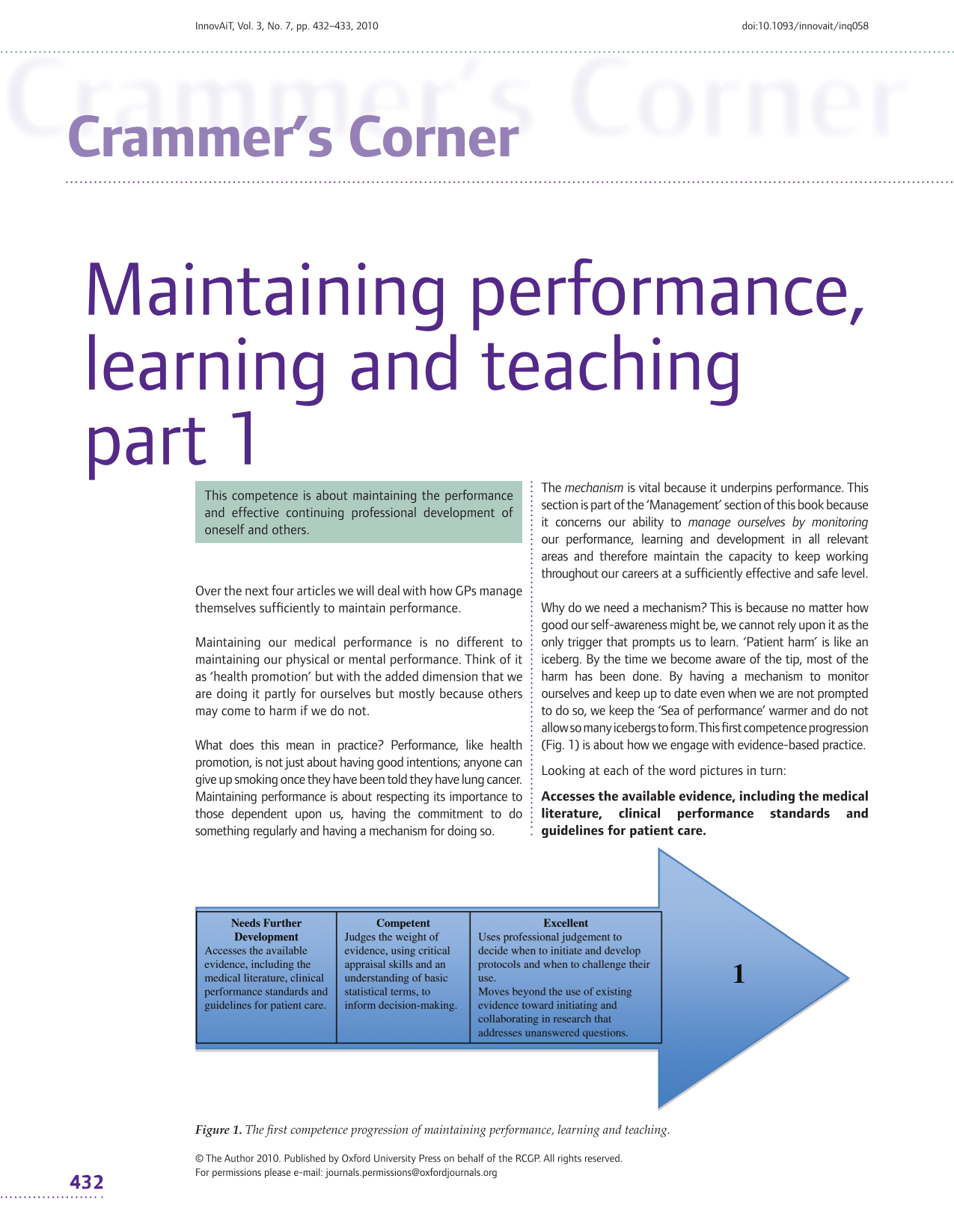
Why do we need a mechanism? This is because no matter how good our self-awareness might be, we cannot rely upon it as the only trigger that prompts us to learn. ‘Patient harm’ is like an iceberg. By the time we become aware of the tip, most of the harm has been done. By having a mechanism to monitor ourselves and keep up to date even when we are not prompted to do so, we keep the ‘Sea of performance’ warmer and do not allow so many icebergs to form. This first competence progression (Fig. 1) is about how we engage with evidence-based practice.
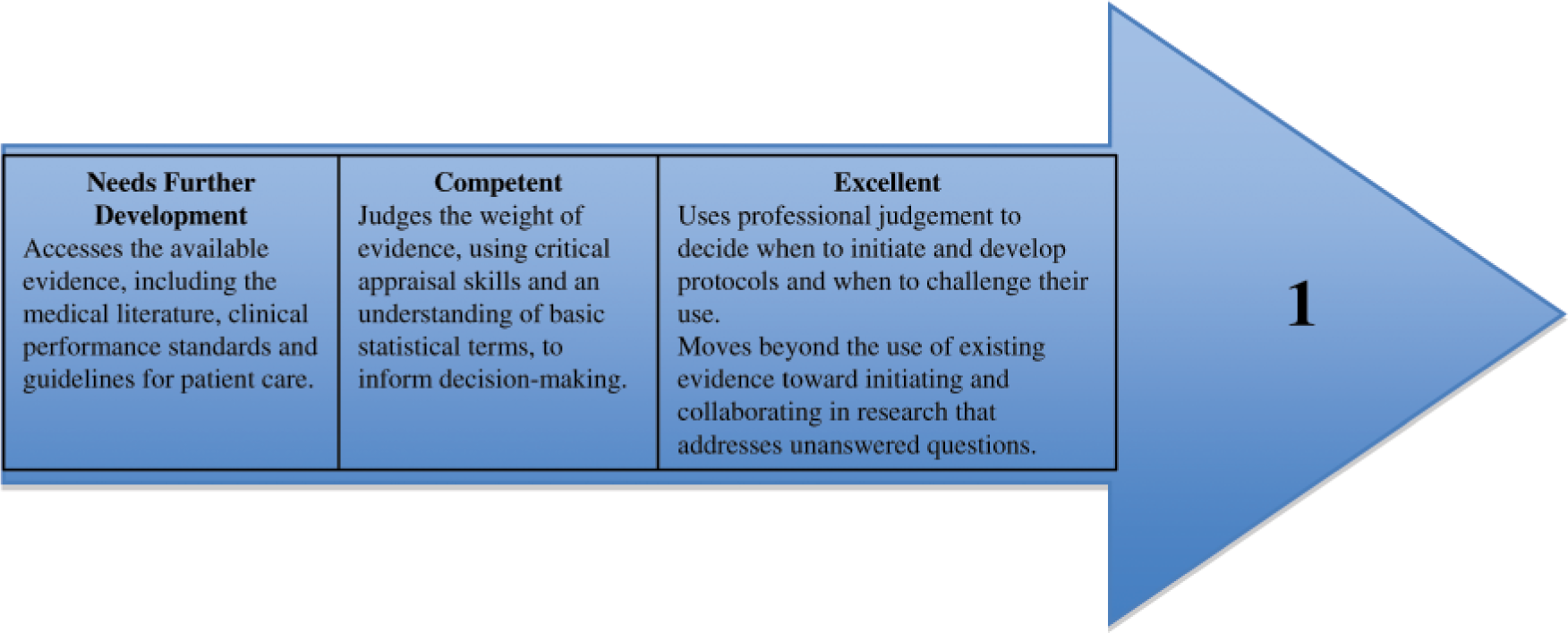
The first competence progression of maintaining performance, learning and teaching.
Looking at each of the word pictures in turn:
Evidence-based medicine (EBM) is the cornerstone of modern medical practice and an important part of maintaining performance is to make routine use of it.
The curriculum identifies the importance of being aware of relevant national guidelines and identifies a number that are particularly important. If you cannot recall whether a guideline exists, a quick Internet search is often worth doing as a check. In addition, to make any sense of the outcome of a search, we need to know which guidelines are more authoritative or trustworthy than others.
EBM is there to guide decision making but it is important not to use EBM in isolation. The curriculum speaks of recognizing the use of ‘value judgements’ to complement the evidence-based approach and this dual approach is explained in the curriculum statement
Tip: developing critical appraisal skills and obtaining evidence
Critical appraisal can seem abstract and therefore of low priority. The secret to developing the appropriate skills is to learn them in the appropriate practical context rather than simply from the books. That way, you will see their value and develop the motivation to want to be competent in this area.
Most practices have access to a prescribing adviser and these colleagues often have practical critical appraisal skills that they can share with you. Make time to discuss the issues they are working on for the practice and find out how critical appraisal helps them to give the appropriate advice.
Some practitioners get together to do a journal club, perhaps as part of a wider clinical meeting. Try taking an interesting article along and presenting a brief critique.
Increasingly, the documents that most powerfully influence (some would say, constrain) medical management are in the form of guidelines or protocols. Although these documents look authoritative, it is important that we do not simply accept them at face value but question their validity in primary care.
There is a systematic way of critiquing the guidelines, and when we do so, the following areas should be carefully thought about:
Are the guidelines dealing with an important-enough topic?
The nature of the health problem, the subjects and setting as well as the providers of care should be stated.
The various approaches to dealing with the problem that were considered in the development of the guidelines should be discussed.
The health and economic outcomes used to compare the clinical practice options should be stated.
How the evidence was gathered, selected and collated and by whom should be known.
These should be considered from the perspective of both the provider and the patient.
How strong is the evidence on which the guidelines are formulated?
Are the guidelines applicable to general practice (i.e. were they developed for use in secondary care?)
Are the guidelines comprehensive? They should deal with most clinical eventualities. To be useful, guidelines should help us manage patients who fall outside the clinical mainstream.
Are the guidelines feasible? Can I implement them in my practice, do I have the resources and would they be acceptable to my patients?
Have the guidelines been validated by external review or clinical testing?
Is there a conflict of interest (such as pharmaceutical sponsorship) that may influence the applicability of these guidelines?
Look for objectivity. Paradoxically, experts are less objective at appraising evidence in their own specialty than in someone else's.
This competence, at present in the ‘excellent’ category, describes how we show and apply our intellectual curiosity. To get into this mindset, try to move beyond asking yourself ‘What?’ and instead ask ‘Why?’ and ‘What if … ?’
Although the vast majority of us will not become researchers, we can fulfil a vital function by facilitating research in primary care so that the evidence base of the future is tailored to our needs and not imported from less suitable contexts.