
Abstract
This competence is about maintaining the performance and effective continuing professional development of oneself and others.
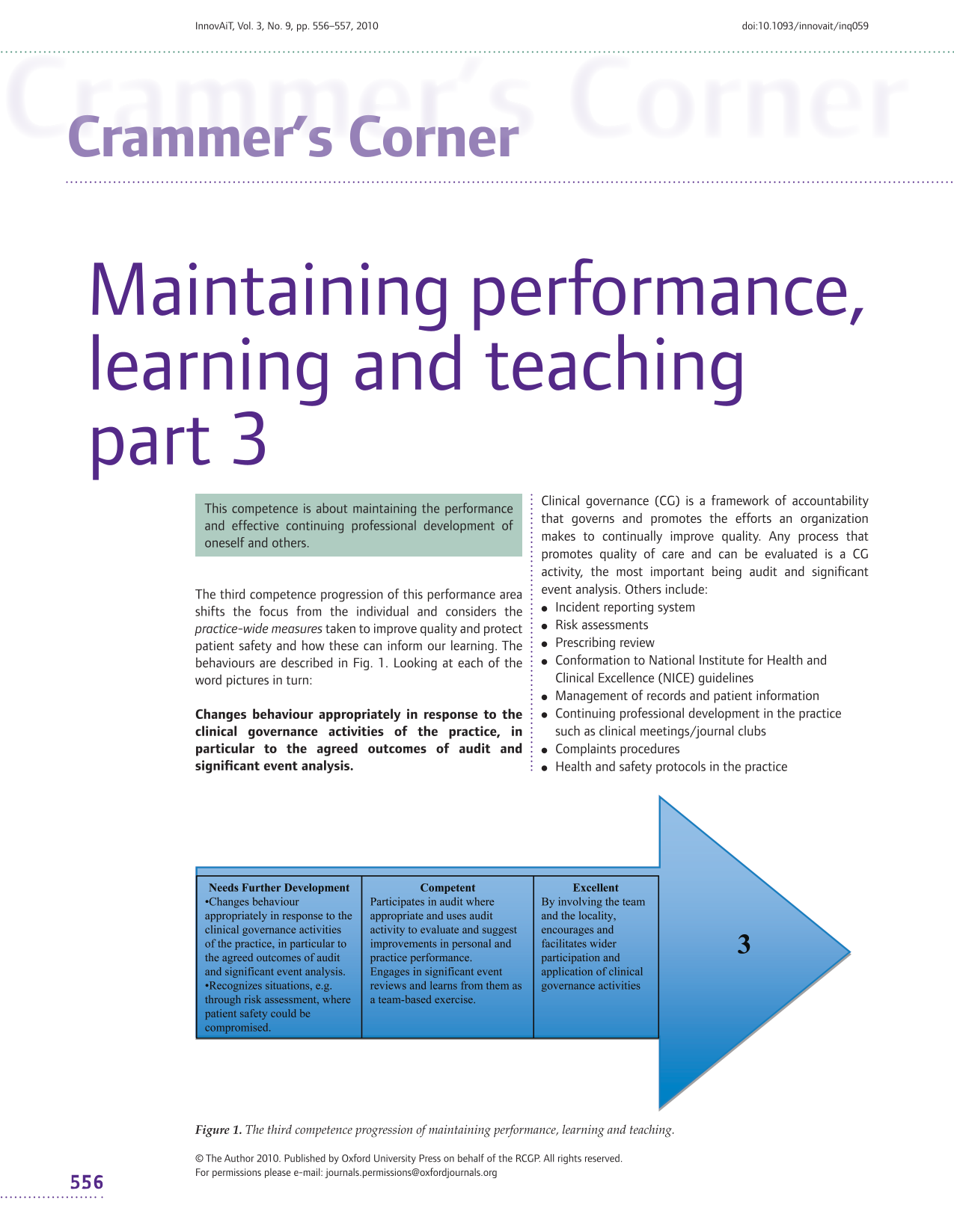
The third competence progression of this performance area shifts the focus from the individual and considers the practice-wide measures taken to improve quality and protect patient safety and how these can inform our learning. The behaviours are described in Fig. 1. Looking at each of the word pictures in turn:

The third competence progression of maintaining performance, learning and teaching.
Clinical governance (CG) is a framework of accountability that governs and promotes the efforts an organization makes to continually improve quality. Any process that promotes quality of care and can be evaluated is a CG activity, the most important being audit and significant event analysis. Others include:
Incident reporting system Risk assessments Prescribing review Conformation to National Institute for Health and Clinical Excellence (NICE) guidelines Management of records and patient information Continuing professional development in the practice such as clinical meetings/journal clubs Complaints procedures Health and safety protocols in the practice
Tip: collecting evidence on response to CG activities
Doctors who are temporary members of a team will have difficulty in obtaining information from many CG activities because data on their performance may not be routinely collected. Look at the list and highlight the ones that you feel you could obtain information from. Discuss your thoughts with doctors/managers early on as they may be able to help you collect information, for example, by adjusting computer data gathering systems to collect information on your referrals. If audits are taking place, find out how your activities could be included in the analysis. Make a note of your engagement with governance activities such as health and safety training. Your response to this information can be shown in a subsequent data collection or through activities in your learning plan.
Patient safety, as a concept, is becoming increasingly prominent and should involve: risk assessment, the identification and management of patient-related risks, the reporting and analysis of incidents and the capacity to learn from and follow up on incidents and implement solutions to minimize the risk of them recurring.
For patient safety to be improved, there are two widespread myths that need to be scotched. These are as follows:
The
The
Risk assessment involves collating information on incidents that the practice becomes aware of. There are three types of incidents that should be reported:
Tip: collecting evidence on patient safety awareness
This competence requires us to show awareness of safety issues. Evidence can arise through case discussion, where we may be asked to identify areas in which things might go wrong and safety might be compromised. The range of areas is extensive, for example, risks inherent in inadequate diagnosis, management and follow-up; risks that arise through poor teamwork (especially communication) and risks attributable to patient behaviour. Additionally, our behaviour such as incident reporting or participation in CG activities shows our awareness of safety. Likewise, those who actively seek information on errors perhaps by asking to be informed when things go wrong are demonstrating a solid understanding of this competence.
incidents that have occurred incidents that have been prevented (also known as near misses) incidents that might happen
To learn the most we can from patient safety incidents, we should apply Root Cause Analysis or Significant Event Audit techniques. Learning to recognize the range of factors allows us to make better safety netting arrangements.
Tip: collecting evidence on the use of audit
You should be able to demonstrate that you are aware of the audit that goes on in practice and you should show that you learn from the audit outcomes. You can show evidence of this by using tools such as the structured reflective template. Additionally, you could suggest/conduct an audit that is not already being done and is prompted by awareness of contemporary best practice, new developments or significant events. Audit can also be used to see whether steps that are taken to improve personal/practice performance have actually been successful. This activity is called ‘completing the audit cyclé.
This competence mentions our ability to ‘suggest improvements’. These should be relevant to the problem, feasible to undertake given the available resources, acceptable to those who are affected (including the patients to whom they apply) and preferably have measurable outcomes so that the degree of improvement can be gauged.
Tip: producing evidence of engagement with significant events
Good evidence would show, preferably from a reflective log, that you have picked up on the key points of the discussion, have thought about whether any of these points apply to you and then developed a learning plan related to these. Even better evidence arises when you bring one of your own significant events to be reviewed by the team.
Primary care organizations are relatively strong in dealing with the management and administration and doctors have a great deal to contribute in that they can comment on the quality markers that might be appropriate to a service. Remember the old adage that ‘What is measurable is not always important and what is important is not always measurable’.