
Abstract
This competence is about practising ethically with integrity and a respect for diversity.
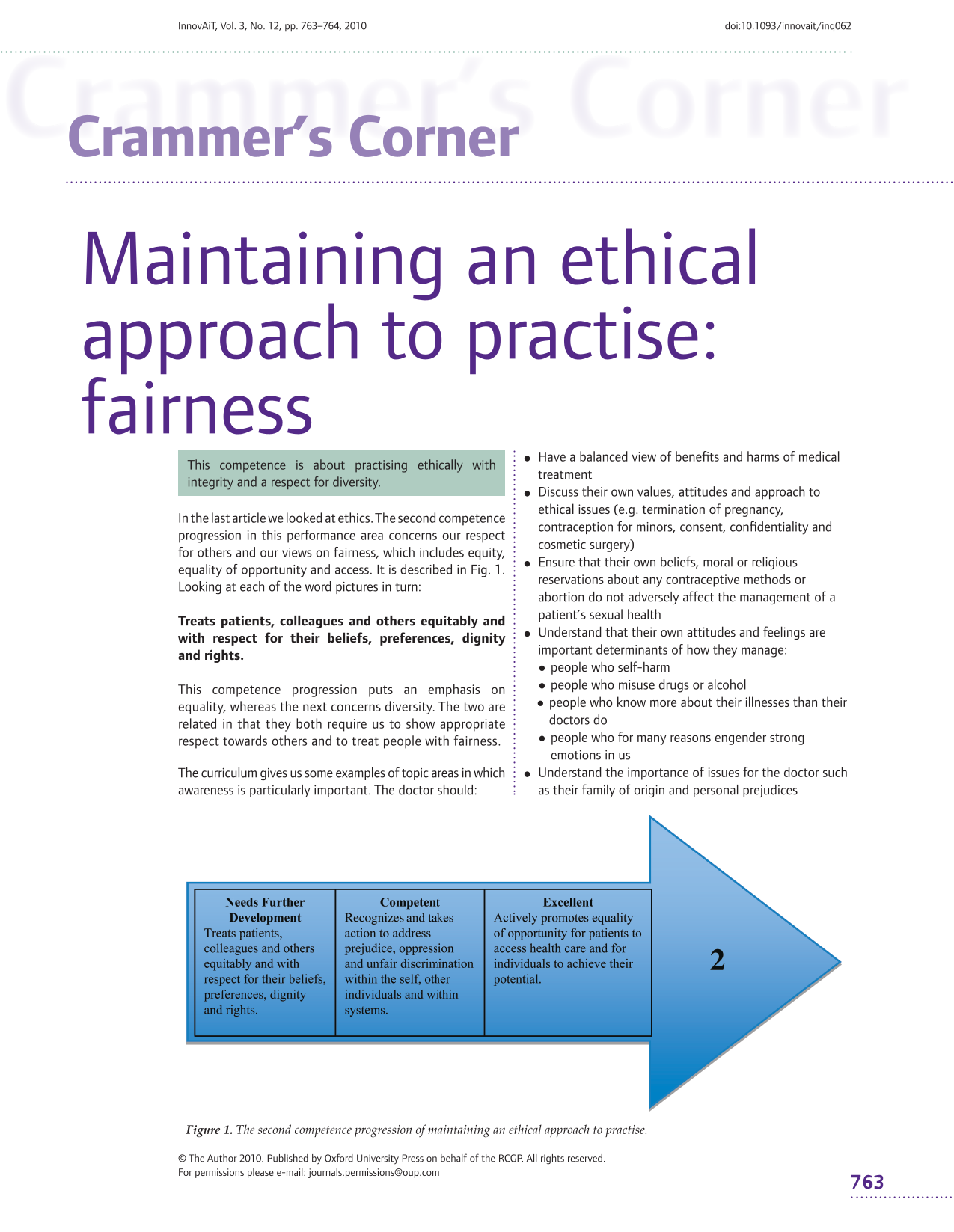
In the last article we looked at ethics. The second competence progression in this performance area concerns our respect for others and our views on fairness, which includes equity, equality of opportunity and access. It is described in Fig. 1. Looking at each of the word pictures in turn:

The second competence progression of maintaining an ethical approach to practise.
This competence progression puts an emphasis on equality, whereas the next concerns diversity. The two are related in that they both require us to show appropriate respect towards others and to treat people with fairness.
The curriculum gives us some examples of topic areas in which awareness is particularly important. The doctor should:
Have a balanced view of benefits and harms of medical treatment Discuss their own values, attitudes and approach to ethical issues (e.g. termination of pregnancy, contraception for minors, consent, confidentiality and cosmetic surgery) Ensure that their own beliefs, moral or religious reservations about any contraceptive methods or abortion do not adversely affect the management of a patient's sexual health Understand that their own attitudes and feelings are important determinants of how they manage:
people who self-harm people who misuse drugs or alcohol people who know more about their illnesses than their doctors do people who for many reasons engender strong emotions in us Understand the importance of issues for the doctor such as their family of origin and personal prejudices
Respect is therefore not a passive act but requires interest, communication and good negotiation both to elicit ‘preferences’ and to negotiate their place in a management plan.
This complex competence is the bedrock of becoming, and continuing to be, a fair person as well as a fair doctor. The wording ‘prejudice, oppression and unfair discrimination’ may be off-putting. For example, although many of us would admit to our ability to be prejudiced, how many of us recognize ourselves as being capable of oppression or unfair discrimination? Although these attributes may not be visible at work, perhaps they show themselves in our private lives? Ask your partner or family! If it is genuine, the ability to be fair should apply as much to our lives outside patient care as within it.
This competence describes three levels (self, other individuals and systems) but these are not the elements of a hierarchy. Without self-awareness and personal action, what we have to say about the other levels may lack insight, conviction and validity. It is not necessary or possible to be blameless in order to comment on others. Nevertheless, we should be humble enough to recognize the weaknesses of our position when making such comments.
Constructive comments with the aim of keeping the system fair for those who work within it and for the patients we work for are therefore necessary. However, taken beyond a certain point this can become oppression, which is unacceptable. The dividing line is not static and to be competent, we need to know what to look for that may alert us that the dividing line is being crossed.
Discrimination
Discrimination is the ability to separate people or items on the basis of some marker of quality. We should not be afraid of being discriminating because it is a necessary part of making judgements. Of course, a balance is needed and the important thing is to ensure that discrimination remains fair.
Equal opportunities
Doctors also select people to positions of responsibility, which may range from opportunities to lead a particular task to being formally employed. A condition, requirement or practice that has the effect of unjustifiably excluding or having an adverse impact on a group is covered by equal opportunities legislation that helps to guide the appropriate mindset.
Assessor's corner: is the doctor discriminating and doing so fairly?
Does the doctor discriminate between different levels of quality, e.g. in their own work or regarding the performance of others? Is the basis of this discrimination fair or are irrelevant or unjustified factors brought in? Does the justification lack insight? Look at the degree of insight that the doctor shows when discussing the ratings that are given by the assessor and by themselves to structured assessments, especially case-based discussion (CbD) and consultation observation tool (COT).
Taking action
Doctors may witness prejudice etc. in colleagues and systems and discuss these with those involved. To demonstrate competence, doctors need to know how to recognize prejudice, oppression and unfair discrimination, be vigilant for the signs of these and raise concerns appropriately and sensitively when they occur or discuss how they might do so.
Unfair positive discrimination
We all have ‘forceful features’ that can subconsciously (and therefore without our awareness) influence our opinion in a positive direction. For example, we can be drawn towards people who are physically attractive or well spoken and also towards people who are like ourselves or remind us of someone we feel positively towards etc. Can you think of any such examples? What are your own forceful features? In which situations would you try to raise your awareness of them? How?
Assessor's corner: is the doctor addressing prejudice?
To address the issues, the doctor must first recognize them. Evidence may come through events or through the discussion of hypothetical cases. Does the doctor admit to having prejudices? (We all have them!) What changes has s/he made or proposed? Where the doctor recognizes a personal issue, evidence of appropriate action to address prejudice etc. may come through the learning cycle, i.e. raising aspects of personal behaviour as issues for discussion with clinical/non-clinical colleagues and then taking steps to identify needs and attend to them.
At the ‘excellent’ end of the competence progression, we apply our understanding of fairness and equality more widely, showing leadership while doing so.