
Abstract
Failure to thrive is a description applied to children whose current weight or rate of weight gain are significantly below that of other children of similar age and sex. It is a common problem that is often seen in general practice. Medical and social factors may both contribute to the condition. These range from paediatric disorders such as coeliac disease to childhood neglect. Early diagnosis and intervention are important for preventing malnutrition, as well as mental, emotional and social problems in adulthood.
The GP curriculum and failure to thrive
The GP curriculum statement on
GPs are required to coordinate care with other health care professionals, adopt a family-centred approach in dealing with children and their problems, understand normal development and manage conditions that may present early and in an undifferentiated way.
Many infants with FTT are not identified unless careful attention is paid to plotting growth parameters at routine check-ups. A detailed history is the best means of establishing the aetiology and directing further evaluation and management. All children with FTT need additional calories for catch-up growth. Few need laboratory evaluation. Close liaison between those involved in the management of infants presenting with FTT, including the family, health visitor, GP and paediatrician, should usually enable appropriate intervention to correct the condition. This article aims to provide an overview of FTT and its management in primary care. It also offers an approach to the assessment of infants presenting with FTT.
Definition and epidemiology
FTT is a general term applied to children whose current weight or rate of weight gain are significantly below that expected of similar children of the same sex and age. It is a common problem, usually recognized within the first 1–2 years of life, but may present at any time in childhood.
FTT is best identified using a standard growth chart (see Fig. 1). There is no single accepted measure to diagnose the condition, and a variety of cut-off points are used. However, most practitioners diagnose FTT when a child's weight for age falls below the fifth centile of the standard growth chart. This means that, by definition, the same percentage of all children are diagnosed with FTT. The disadvantage of using an isolated reading is that it identifies many naturally small children with only minor variations in weight gain but may miss children who drop from higher centile positions.
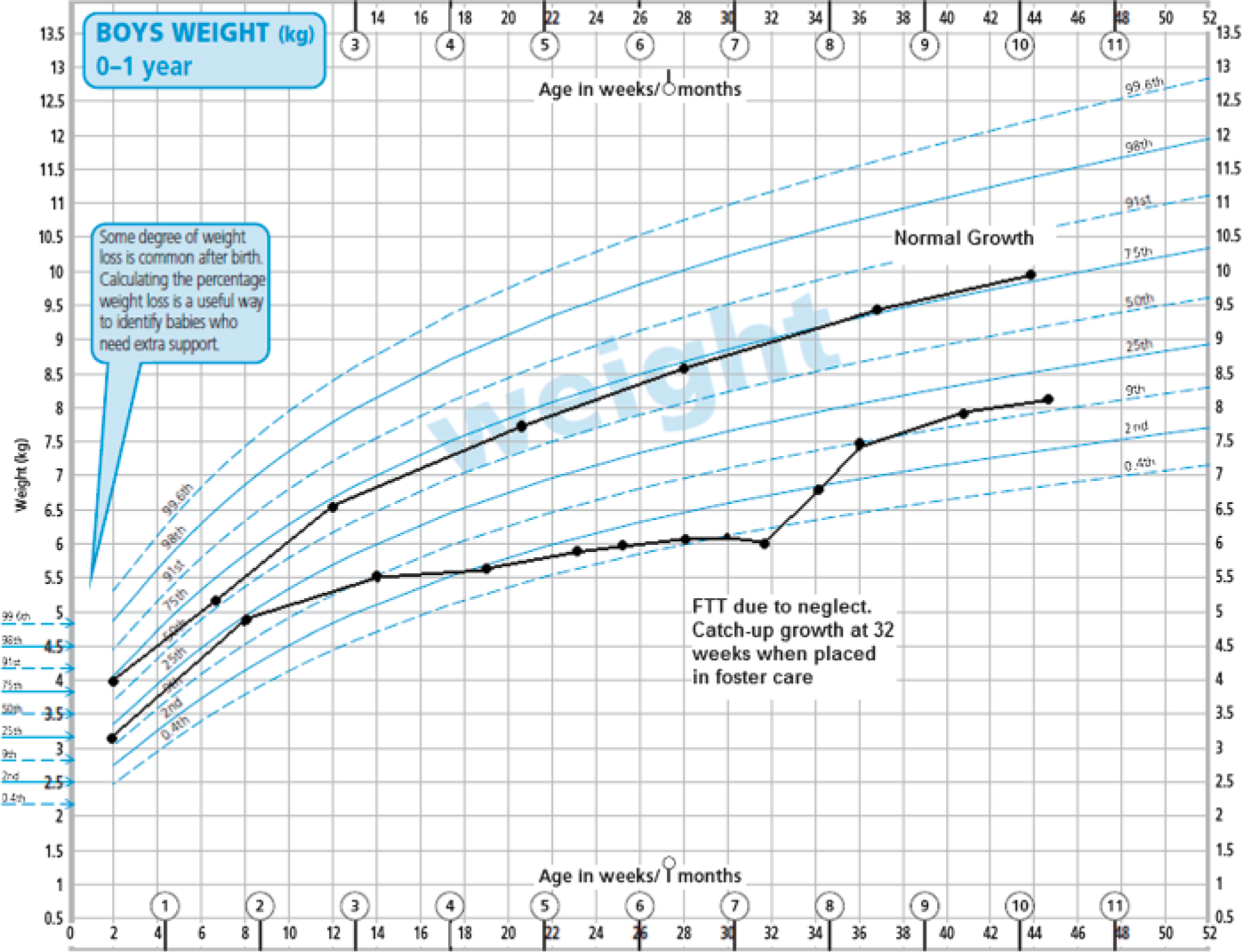
UK WHO growth chart. Boys weight age 0–1 year. Copyright© 2009 Department of Health. Reproduced under the terms of the Click-Use Licence
A more useful definition that is frequently used is if a child's weight for age crosses more than a certain number of centiles, usually set as two major centile lines. Other growth parameters that can assist in making the diagnosis are weight for height and height for age. FTT is diagnosed if a child falls below the 10th centile for either of these measurements or if weight for height is less than 80% of the ideal weight.
Normal growth variations
The first consideration in a child presenting with presumed FTT is recognizing normal variants of growth. Many children are naturally small and should not be diagnosed with FTT.
An obvious example is premature infants. These infants often grow below their age-matched peers but parallel to the normal growth curve. When corrected for gestation, their growth parameters usually fall within the normal range. This correction is helpful until around the second year of life, at which time delays of only a few months become negligible.
Then there are those with genetic short stature. These infants have small parents and often have a low or normal birth weight and grow along their low centile line for both weight and height, following their genetic potential. Other populations with normal growth variations include certain ethnicities (e.g. Asian) and children with specific conditions. In fact, there are separate growth charts for children with Down's syndrome and Turner's syndrome that can help reassure GPs that these children are growing appropriately.
It is also estimated that about 25% of normal infants will shift to a lower centile in the first 2 years of life and then follow that centile. There are several reasons for this and health care professionals should not treat these children as having FTT:
Firstly, there are infants who are exclusively breastfed. Breastfed babies often gain weight and cross centiles upwards in the first 4 months but slow down later. Then there are those infants who are larger than expected at birth (e.g. macrosomic infants of mothers with gestational diabetes) who after birth undergo a period of ‘catch-down’ growth where their weight for age crosses centiles and then follows a lower growth centile line (see Case study 1). Many normal babies may also lose up to 10% of their birth weight within the first few days of life. However, this weight should be regained by 2 weeks of age. Finally there are those infants with constitutional growth delay whose growth is delayed when compared with their peers of the same age. A similar growth pattern is often noted in their parents or siblings. This is best identified by assessing bone age.
Aetiology
FTT is not a final diagnosis but a description of a physical state, therefore a cause for the FTT must always be sought. Historically, FTT was classified as either organic or non-organic.
Case study 1
Max is 5 months old. He is brought to see his GP because his parents are worried about his poor weight gain. He was born at term following a pregnancy complicated by maternal gestational diabetes. His birth weight was 4.8 kg, just above the 97th centile. At 2 months old, his weight was on the 90th centile and at 3 months his weight was on the 75th centile. It is now just below the 50th centile. His length is on the same centile. He is otherwise healthy and his examination is normal. He is followed up over the next few months and his weight and length remain just below the 50th centile. A diagnosis of ‘catch-down’ growth followed by now normal growth is made.
Using this classification, over 90% of children with FTT have a non-organic cause. However, it is now recognized that these two distinctions are overly simplistic, as most cases of FTT are influenced by many factors. For example, an infant may have a medical illness that causes feeding problems and stress within the family. The stress can add to the feeding problem and worsen the FTT. A more useful system is based on pathophysiology. This can be divided into four main groups: • Inadequate caloric intake
Inadequate absorption Excess metabolic demand Defective utilization
Inadequate caloric intake
Most cases of FTT are due to failure of food intake. Inadequate calorie intake can be unintentional or intentional. It may result from lack of available food as a consequence of poverty and/or food shortages, lack of knowledge about infant feeding, improper feeding techniques, family dysfunction (e.g. substance abuse and domestic violence), maternal depression or specific dietary beliefs that limit foodstuffs offered to the infant. This type of FTT often hinges on the parent—child interaction. For example, the problem may be the parent not offering enough food, the child refusing to take enough food or a combination of both (see Case study 2). Children in abusing or neglecting families are also at increased risk of FTT, but such families still only comprise a small proportion of total cases. Rarer causes include factitious disorder (Münchhausen's syndrome by proxy).
Case study 2
Sophie is 4 months old. She visits her GP because the health visitor is concerned about her low weight and the interactions between mother and baby. Sophie was born at term by emergency caesarean following a difficult labour. Her weight and height were on the 50th centile at birth. Her mother, Kate, had difficulty in establishing breastfeeding. Her father works long hours to try and support his family. Sophie is currently fully breastfed, feeding up to 10 times per day, including several feeds during the night. Kate is tearful and complains of low mood, fatigue and little enjoyment. Sophie appears thin and has a weight of 5.2 kg (third centile), length 61 cm (25th centile) but has no other signs or symptoms. Investigations are also normal. Her GP diagnoses Kate with post-natal depression and starts appropriate treatment. Both Sophie and Kate are followed up regularly and a significant improvement is seen in Kate's mood along with an increase in Sophie's weight.
There may also be specific organic issues with the infant that limit feeding, such as poor appetite as occurs with iron deficiency anaemia, chronic infection and psychological disorders. Other examples include inability to suck or swallow, especially with central nervous system (CNS) or muscular disorders or anatomical abnormalities such as cleft palate.
Inadequate absorption
Inadequate absorption is usually due to malabsorption or persistent emesis. Recognized causes of malabsorption include chronic diarrhoea, inflammatory bowel disease, coeliac disease, protein-losing enteropathy, pancreatic insufficiency (e.g. cystic fibrosis), liver disease, food sensitivities (e.g. cow's milk protein allergy) or excessive juice intake. Persistent vomiting can be caused by gastrooesophageal reflux, bowel obstruction (e.g. pyloric stenosis), infections, raised intracranial pressure, medications or underlying metabolic or CNS disease.
The diagnosis is often aided by the age of the child. For example, coeliac disease usually presents after the introduction of gluten-containing solids, such that a fall-off in growth is seen around 4–8 months of age. An earlier drop in growth associated with gastrointestinal symptoms would indicate other causes such as gastro-oesophageal reflux. An acute illness, such as gastroenteritis, may also cause poor weight gain although this should be temporary rather than permanent. The child should be reviewed 6–8 weeks later.
Increased requirements and defective utilization
Increased requirements occur in those infants with a higher metabolic rate or defective energy utilization. This is frequently due to chronic illness, such as congenital heart disease, chronic lung disease, hyperthyroidism, diabetes, renal tubular acidosis, liver disease, chronic immunodeficiency, recurrent infection or malignancy. Defective utilization is usually associated with genetic abnormalities, congenital infections and metabolic disorders (e.g. storage diseases and amino acid disorders). Some of these conditions may also contribute to the FTT by other mechanisms described above. For example, cystic fibrosis can cause maldigestion via pancreatic enzyme deficiency, reduced intake due to chronic infection and increased requirement due to liver disease.
Diagnosing FTT
Children with FTT are most often identified when parents or carers raise concerns about the child's feeding or growth patterns or when a physician or health visitor notes a decrease in the child's growth on physical examination. In both situations, the key to diagnosing FTT is finding the time in a busy surgery to carefully measure and plot a child's weight, height and head circumference.
Weight assessment is best done either bare or in minimal clothing. Length is usually performed up until the child is 1–2 years old, after which a height measurement is more reliable. An accurate assessment of growth also requires comparison with past measurements. Once FTT has been identified, the next step is to focus on careful history taking and physical examination in order to establish the underlying cause and exclude significant organic pathology.
History
The first issues to address are the specific worries of the concerned adult, be they parent, carer, health visitor or midwife. A thorough history should include an assessment of diet and feeding behaviours. Relevant information can usually be gained by asking about what is eaten, how often it is eaten, beverage consumption and what behaviours occur around mealtimes. Information on shopping, budgeting and cooking equipment in the home may also be revealing. It is also important to take a detailed birth history, as well as past and current medical, social, family and developmental history. This may include general questions about the social, emotional and financial stability of the family, as well as illnesses that the child or family has had. Specific items that should be covered in each category are shown in Table 1. Some of this information may be best gained from talking to other professionals involved with the child and/or family. This is particularly important if there are concerns about neglect.
Areas to cover when taking a history of FTT
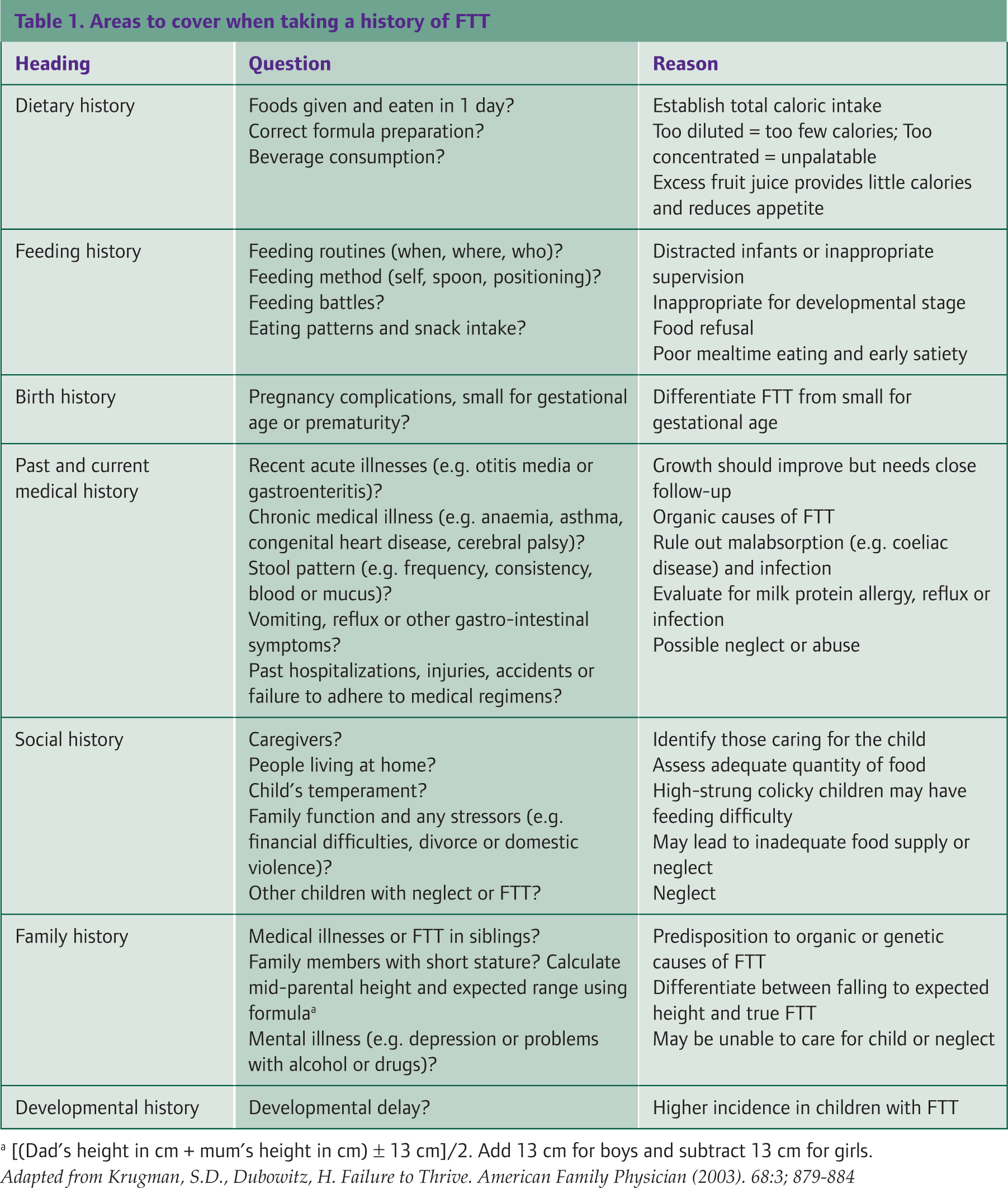
[(Dad's height in cm + mum's height in cm) □ 13 cm]/2. Add 13 cm for boys and subtract 13 cm for girls.
Physical examination
A complete physical examination is essential in order to detect any underlying disease that may hamper growth. This should include a search for minor and major anomalies, such as skin rashes and cleft palate. Examination of the chest may identify features of chronic respiratory or cardiac disease, for example, cyanosis and tachypnoea, whereas examination of the abdomen may reveal distension due to malabsorption or organomegaly. Other mandatory assessments include neurologic examination, evaluation of suck—swallow coordination, observation of the child's developmental skills and an assessment for dysmorphic features suggestive of a genetic disorder, such as Down's syndrome.
Another main aim is to identify signs of possible child neglect or abuse. An assessment should look for any suspicious injuries and note how the child interacts with his or her parents. Observing the interaction during a feeding session is particularly helpful, although this is difficult to undertake in the surgery. It is often best done during a home visit by an appropriately trained health care professional. It is helpful to note a carer's ability to recognize the child's cues, as well as the parental warmth and appropriate behaviour towards the child. It is equally important to observe the nature of the child's cues, the child's temperament and responses towards the parent.
Finally, examination helps establish the severity of malnutrition. This can be crudely done by observing the child to see if he or she looks well-nourished or starved. There may be signs of dehydration. Wasting of the buttocks indicates general muscle wastage. A more precise measure can be determined using the Gomez criteria. This involves comparing the child's current weight for age with the expected weight (50th centile). If the weight is less than 60% of expected, then FTT is severe, 61–75% denotes moderate FTT and 76–90% is mild.
Investigations
Laboratory and radiological studies are usually unnecessary and rarely help establish the diagnosis or prognosis. Most children with FTT have normal results. Further investigations should only be performed as guided by positive findings from the history and examination:
Infants who are generally well, with no positive findings, rarely require immediate investigations and should be followed-up with a ‘wait-and-see’ approach. Infants who are unwell or have significant positive findings need immediate investigation and paediatric referral.
An obvious example is a child with steatorrhea. He or she should have a stool sample sent for faecal fat and perhaps a sweat test if there is suspicion of cystic fibrosis, such as recurrent respiratory infections.
If the child's growth has not improved at follow-up, screening tests should then be considered either by the GP or following referral to a paediatrician. These typically include:
Blood tests for full blood count, urea and creatinine, liver function tests, erythrocyte sedimentation rate and coeliac antibody profile Urinalysis Stool sample for fat and reducing substances
Other tests occasionally performed include blood tests for human immunodeficiency virus (HIV) infection, thyroid function tests, growth hormone levels, calcium/phosphate levels, glucose levels, iron studies, immunoglobulins and karyotyping, as well as stool studies for parasites and urine for organic and amino acids (metabolic screen).
Radiological studies can be useful in assessing bone age and help distinguish between genetic short stature and constitutional growth delay. In children where significant doubt persists and tests have been unhelpful, a brief stay in hospital for a trial of observed feeding may be helpful.
Complications
Children with FTT are at higher risk of short stature, behaviour problems and lower cognitive performance. It is likely that FTT is a confounding factor to these adverse outcomes rather than an isolated cause. However, it is important to recognize and treat FTT promptly in order to help limit these sequelae. For example, identification of poor growth in a small number of children is a route to diagnosing important, treatable organic conditions. A further small proportion of poorly growing children may do so as a result of neglect, where poor growth can be an important marker for the need for intervention.
Management
FTT is common and often resolves with simple interventions from primary care, such as nutritional advice and modification of feeding behaviour. In the UK, health visitors are ideally suited to undertake this work. A home visit might reveal obvious dietary issues and this input alone often results in improvement. Having parents write down the types of food and amounts a child eats over a given period (usually 3 days) helps quantify caloric intake. In some instances, it can make parents aware of how much the child is or is not eating.
High-calorie diet
All affected children, regardless of the reason for FTT, need a high-calorie diet for catch-up growth. In infants, this increased calorie intake may be achieved by concentrating formula or adding rice cereal to pureed foods. Toddlers can receive more calories by adding fats such as cheese and butter to commonly eaten foods. Limiting fruit juice can aid weight gain as too much fruit juice provides relatively empty carbohydrate calories and reduces a child's appetite for nutritious meals. Multivitamin supplements are sometimes required, although this is usually guided by specific testing of these levels. Additional input from a dietician may be needed to allow exact caloric requirements to be calculated, such as by formulae based upon current and ideal weight and usual calories required for age.
Feeding behaviours
The aim of feeding behaviour strategies is also to promote better caloric intake. GPs should advise parents to encourage, but not force, their child to eat. Meals should be pleasant, regularly scheduled and ideally eaten with other family members. Praise should be given when food is eaten. It also helps if the child is positioned so that he or she is comfortable and has his or her head up. Parents should consider foods that the child likes, although it is important to encourage some variety and to cover the basic food groups. Small amounts of food should be offered first and then the amount increased rather than starting with large quantities. Snacks need to be timed in between meals so that the child's appetite will not be ruined.
Underlying cause
The other key goal to managing FTT is to identify any underlying medical cause and correct it. Such cases usually require referral to a paediatrician. Examples include, starting a gluten-free diet for coeliac disease (see Case study 3), diuretics for heart failure or pancreatic enzyme replacement for cystic fibrosis. It is also necessary to address any identified psychosocial issues. If a mother is not coping, she is likely to need help and advice with plenty of input from the health visitor. Post-natal depression may need specific treatment. If the child is judged to be at risk, he or she must be reported to the appropriate child protective services agency. Their interventions may increase parental compliance or allow for additional support services such as childcare, counselling and home visitation. Occasionally, it may be necessary to remove the child, but this is a last resort and should not be done without considerable thought and attempts to rectify the situation.
Referral and hospitalization
For children who do not respond to initial management, a referral to a paediatrician is needed. This approach is particularly useful for children who are not improving because of an undiagnosed medical condition or a particularly difficult social situation. In such cases, a multidisciplinary approach involving physicians, nurses, dieticians, social workers and psychologists produces the best outcome. The time taken before deciding on referral may vary from a few days to weeks, depending on the child's age, current weight, rate at which the weight is crossing centiles and possible underlying cause.
Case study 3
David initially presents at 10 months of age to his GP with a history of poor weight gain over the past 4 months. He was born at term following an uneventful pregnancy, and his weight and length were on the 50th centile. He was exclusively breastfed until 5 months of age when solid foods were introduced. At the time of presentation, his parents deny any symptoms but examination reveals slight wasting of his buttocks. He is referred to a paediatrician who undertakes further investigations. This reveals an abnormal anti-endomysial antibody level and elevated anti-gliadin antibodies. Coeliac disease is confirmed by subsequent colonoscopy, and David is started on a gluten-free diet. Soon afterwards, his weight begins to increase.
Immediate referral by a GP may also be appropriate if the child is unwell or has significant positive findings at their initial assessment. Hospitalization is rarely required but may be necessary for children with severe FTT, when outpatient management has failed or if abuse or neglect is suspected.
Follow-up
Ideally, children with FTT should be followed at least monthly until catch-up growth is demonstrated. They should then be observed at regular intervals to ensure the positive trend is maintained. Health visitors are ideally suited to undertake this work.
Key points
FTT describes children whose current weight or rate of weight gain is significantly below other children of similar age and sex A variety of cut-off points are used to diagnose FTT, including weight below a particular centile or crossing more than a certain number of centiles It is imperative for GPs to understand normal growth variation in order to avoid over-diagnosing FTT There are a very wide range of causes of FTT, including environmental and social factors and medical disorders, and more than one may be applicable A careful assessment involving history taking and physical examination is required to determine the aetiology and direct treatment Management of FTT always involves a high-calorie diet, as well as correction of the underlying cause