
Abstract
Meningitis and encephalitis are both acute medical emergencies with considerable morbidity and mortality. They have public health implications and are listed as notifiable diseases. This article aims to give an overview of meningitis and encephalitis, outlining their recognition and management relevant to general practice.
The GP curriculum on meningitis and encephalitis
Have knowledge of the natural history and aetiology of brain infections such as meningitis and encephalitis Have knowledge of the clinical features of patients presenting with meningitis and encephalitis Have an awareness of secondary care investigations and treatments Be competent in the initial emergency management of meningitis and meningococcal septicaemia Understand the management of encephalitis and meningitis Be aware of prevention of meningitis in the form of vaccination Be familiar with notification of these diseases and follow-up of sufferers
Meningitis
Meningitis is defined as inflammation of the meninges. Meningitis and meningococcal septicaemia are separately notifiable diseases, and it is compulsory to notify confirmed and suspected cases. It is estimated that every day nine people become ill with the disease resulting in one death. A further two people will be left with life-altering after effects such as brain damage, deafness and multiple amputations.
Epidemiology
The incidence of meningitis is approximately two to six cases per 100 000 per year in the UK. The incidence is highest in winter and the under fives are most at risk (400 per 100 000 in neonates), followed by teenagers aged 15–17 years. The causative pathogen varies depending on the age and immune status of the patient (Table 1). Viral meningitis is the most common, being generally associated with less severe disease than the bacterial form and with the majority making a full recovery.
Causes of meningitis
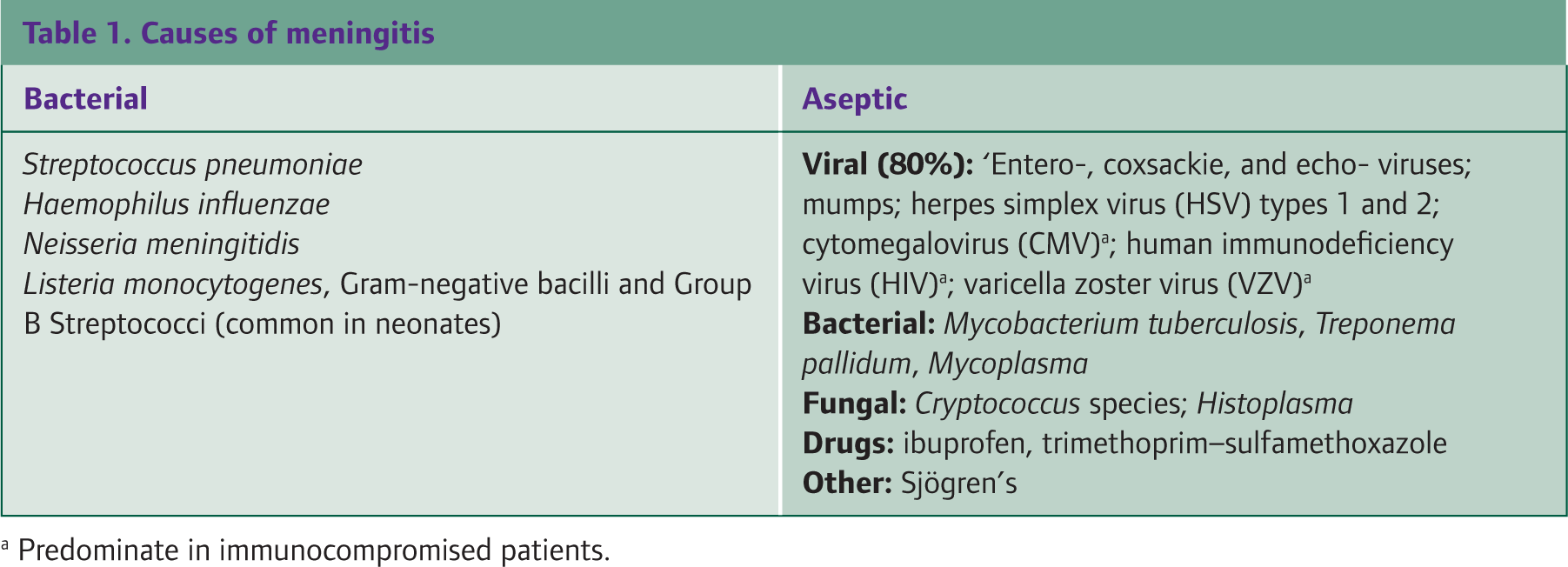
Predominate in immunocompromised patients.
Meningococci can cause meningitis and/or septicaemia that may present alone or in combination. Most cases of meningococcal disease occur sporadically, with less than 5% of cases occurring in clusters. The most common serogroups that cause disease worldwide are groups B, C, A, Y and W135. Septicaemia is the most common and malignant form of meningococcal disease and carries significant mortality and morbidity.
Pathogenesis
Most organisms that cause bacterial meningitis are normal inhabitants of the upper respiratory tract. Spread is via the droplets and secretions of carriers through prolonged close contact, coughing, sneezing or sharing utensils. The incubation period for bacterial meningitis is 2–5 days. Progression to meningitis or septicaemia occurs in a small percentage of those exposed to the organisms and is dependent on host factors and the strain of the organism involved. Haematogenous spread and breach of the blood-brain barrier are the most common methods of central nervous system (CNS) invasion. The resulting inflammation leads to cerebral oedema and abnormalities in cerebral blood flow and may result in neurological damage. Alternatively, proliferation in the blood leads to septicaemia and circulatory compromise.
Risk factors
The following patients are at increased risk of bacterial meningitis:
Those at the extremes of age (the over 60s, children under 5 and neonates) Immunocompromised patients: diabetics, those with human immunodeficiency virus (HIV), alcoholism or malignancy Those who have had close contact with cases Those from lower socio-economic groups Males
Neurosurgery, cerebrospinal fluid (CSF) shunts, cochlear implants and penetrating head trauma all also predispose to bacterial meningitis. Implicated bacteria in these cases are usually staphylococci and Gram-negative organisms.
The consultation
The majority of litigation against GPs in the context of meningitis is because of a delay or failure to diagnose the condition. GPs need to be competent in recognizing meningitis early as this improves survival and long-term outcomes.
The history should elicit information on symptoms, travel and immunizations. Examination should include a record of basic vital signs such as respiratory rate, heart rate, conscious level and capillary refill time. A thorough cardiovascular, respiratory and neurological examination should be performed. The entire body should be examined to look for a petechial rash (Fig. 1), and in infants, the fontanelles should also be checked.

Use of the ‘glass test’ to detect the non-blanching purpuric/petechial rash of meningococcal disease.
The early prodromal phase may be non-specific, and distinguishing this from more common benign self-limiting viral illness may be impossible. Certain symptoms or signs may point to a diagnosis of meningococcal disease (Table 2), and patients, relatives and practice staff should be educated in recognizing these. Safety netting should form an integral part of all consultations, with the option of further follow-up where appropriate. This should include information on seeking help should the illness get worse, or if there are any concerns regarding the patient's well-being. Despite obvious time pressures, this can be performed and documented in minutes and augmented by the use of written patient information leaflets.
Red flag symptoms and signs of meningitis and septicaemia

Note: Small children, the elderly and the immunocompromised may not present with typical signs - have a low threshold for referral if you suspect meningitis in these groups.
GPs should be particularly vigilant when assessing the elderly, infants or immunocompromised patients. These patients often present atypically, which may result in diagnostic delay and increased mortality. Telephone consultations are particularly fraught with danger. It is very difficult to assess infants and children over the telephone and if there is uncertainty regarding the severity of the illness, it is pertinent to see the patient. Documentation of telephone consultations is essential as details can be easily forgotten and in the case of an adverse incident may have significant medico-legal implications. Practices should have agreed procedures in place for dealing with urgent calls, and significant event analysis is an invaluable way of reflecting on these systems.
Presentation in adults
Suspect meningitis in patients presenting with symptoms of:
fever headache neck stiffness and/or altered consciousness
Although a ‘classical presentation’ with all four of these: symptoms occurs in less than half of adult patients presenting with meningitis, at least two of the four symptoms occur in over 95% of patients, and the absence of all of these four symptoms makes meningitis unlikely (van de Beek et al., 2007). Symptoms such as nausea and vomiting are non-specific and therefore poor predictors of meningitis.
Neck stiffness occurs as a result of meningeal irritation. True neck stiffness can be illicited by asking patients to kiss their knees or by assessing the ease of passive flexion in a relaxed patient. However, this finding itself may be found in only a third of adults and is also absent in septicaemia. Kernig's and Brudzinski's signs are used to elicit meningeal irritation and are often documented in the clinical examination (Fig. 2). Although very specific (95%), these signs have been shown to have poor sensitivity (5%), therefore their absence is never reassuring (Thomas et al., 2002).

Kernig's and Brudzinski's signs. Kernig's sign: with patient supine and thigh flexed to 90 degrees, the leg is straightened. The sign is positive if there is resistance to straightening or extending leg. Brudzinski's sign: flexion of the neck causes involuntary flexion of the knees and hips. Pictures of Kernig's and Brudzinski's neck signs courtesy of Mr M. Roche.
Presentation in infants
Infants and neonates may present with non-specific complaints such as irritability, excessive crying, apnoea, rash, lethargy or poor feeding. In order to identify neonates at high risk of Group B streptococcal (GBS) meningitis, enquire about:
Delivery under 37 weeks gestation Ruptured membranes for 18 hours or longer Intrapartum antibiotic prophylaxis Previously delivered child with GBS GBS bacteriuria during pregnancy Intrapartum fever (38°C or greater)
Examination may reveal irritability on handling, a ‘high-pitched’ or ‘moaning’ cry, abnormal tone or posture, cyanosis and/or a bulging fontanelle.
Presentation in children and adolescents
A national study into the presenting symptoms of meningitis in children and adolescents found that almost 50% of patients who were initially seen by their GP were sent home and were subsequently more likely to die (Thompson et al., 2006). This study suggested that the classical features of meningitis and/or septicaemia were preceded by a prodrome lasting between 4 and 8 hours.
‘Particularly significant early symptoms and signs (appearing within 8 hours of onset) were: Severe leg pain - so bad that the child cannot stand or walk. Cold hands or feet when the child is running a fever. Pale skin with or without blueness aound the lips.
The classical petechial rash was next, developing at around 9 hours, later followed by neck stiffness and photophobia at 12–15 hours
The petechial rash is arguably the most widely recognized sign of meningococcal disease among the general public, with parents often consulting their doctor over concerns about its presence. It may indicate septicaemia, spread within minutes and can be checked for using the ‘glass test’ (Fig. 1). The National Institute for Health and Clinical Excellence (NICE) guidelines for feverish illness in children (NICE, 2007) identify this rash as a ‘red’ or ‘high risk’ sign in its traffic light system, therefore its presence warrants serious consideration for hospital admission. However, many other conditions can cause a purpuric rash (Box 1) and so it should always be evaluated in the clinical context.
Causes of purpuric rash
Meningococci or Meningococcal infection Idiopathic thrombocytopenic purpura Leukaemia Viruses-particularly enterovirus Pressure, e.g. from tight clothing Henoch Schönlein purpura Forceful coughing or vomiting
Doctors and patients should not be falsely reassured by the absence of a petechial rash or the presence of one that does blanch on pressure in an ill child. Remember that even with severe disease children may look very well due to their high reserve but may decompensate rapidly.
Presentation in the elderly and immunocompromised
Elderly patients may present with confusion, which may be mistakenly attributed to psychiatric illness, infections or medications. Furthermore, Kernig's and Brudzinski's signs can be falsely positive as these may be found in healthy elderly people, possibly as a result of cervical spine disease and reduced neck mobility. Certain pathogens (e.g. Cryptococcus) may result in a more subacute presentation or even chronic meningitis in the immunosuppressed. It is important to elicit a history of pneumococcal vaccination.
Partially treated meningitis
The often non-specific presentation of early meningitis may mean that some patients initially receive oral antibiotics for other infections (e.g. otitis media). This may mask symptoms and delay presentation. Consider this diagnosis in patients with suspicious symptoms whose illness fails to resolve as expected.
Pre-hospital management
All patients with suspected meningitis or meningococcal disease should be admitted to hospital via emergency ambulance. Intravenous (IV), intramuscular (IM) or intraosseous (IO) antibiotics should be administered immediately while arranging hospital transfer. These should be given as proximally as possible into a part of the limb that is well perfused. Benzylpenicillin is the pre-hospital antibiotic of choice in the UK and guidelines recommend that all GPs should carry and administer it intramuscularly, unless contraindicated by known allergy (Box 2) [Health Protection Agency (HPA), 2006]. GPs do not have to carry alternative antibiotics, but cefotaxime, ceftriaxone or even chloramphenicol may also be used (HPA, 2006).
Pre-hospital treatment of suspected bacterial meningitis and meningococcal septicaemia [British National Formulary (BNF) recommendations]
Child younger than 1 year: 300 mg benzylpenicillin IM Child 1–9 years: 600 mg benzylpenicillin IM Child older than 10 years and adult: 1.2 g benzylpenicillin IM
Diagnosis in hospital
All patients should have blood cultures, throat swab and blood sent for polymerase chain reaction (PCR) tests and serology. Routine full blood count (FBC), urea and electrolytes (U/Es), lactate, glucose, clotting and C-reactive protein (CRP) tests should also be performed. Aspiration of petechiae is often forgotten but may detect meningococci in two-thirds of patients.
Lumbar puncture (LP) and examination of CSF is essential. Localized back pain and post-LP headache (32%) as a result of prolonged spinal fluid leakage may occur. Patients may consult their GP following discharge with these symptoms. This headache is postural and often associated with nausea, diplopia or vestibular symptoms. It is usually self-limiting to several days and patients may be reassured and managed with bed rest and analgesia. Occasionally, post-LP headache may be incapacitating and referral to hospital for consideration of an epidural blood patch may be required. A brain computed tomography (CT) may help identify patients at increased risk of herniation prior to LP and exclude mass lesions.
Treatment in hospital
Antibiotic therapy with cefotaxime or ceftriaxone is recommended because of their broad spectrum of activity and good penetration into the CSF. Giving IV dexamethasone to immunocompetent patients results in a reduction in mortality (from 34 to 14%) and other neurological sequelae (van de Beek et al., 2007).
Case reporting
All cases of suspected meningitis or meningococcal disease should be reported to the Consultant in Communicable Disease Control (CCDC) or Consultant in Public Health Medicine (CPHM). This is usually done by the hospital on confirmation of the diagnosis, but GPs should ensure that this has been done. The CCDC or CPHM ensures that intimate and household contacts receive chemoprophylaxis with rifampicin, ciprofloxacin or ceftriaxone irrespective of vaccination status (Table 3). This aims to reduce invasive disease by eliminating carriage in the group of close contacts. Rifampicin and ceftriaxone can be used in pregnancy or breastfeeding mothers, but ciprofloxacin is not recommended.
Indications for prophylaxis in meningitis

Management of contacts
As a GP, you may be faced with queries regarding those who have been in contact with cases of meningitis. Although the risk to contacts is low, the highest documented risk is to people who live in the same household as an index case. The risk is highest in the first 2–7 days after a case and falls rapidly during the following weeks. Beyond the 4 week period, the risk is probably close to background levels (less than 1 in 300).
For non-household contacts, after a confirmed isolated case, the risk to another child in the same institution of developing the illness within the next 4 weeks is as follows:
Pre-school-1 in 1500 Primary school-1 in 18 000 Secondary school-1 in 33 000
Close contacts of cases due to Neisseria meningitidis should also be offered an appropriate vaccine once diagnosis has been confirmed and up to 4 weeks after onset of illness. Patients should still be vigilant, however, and be given appropriate information and leaflets on meningitis and meningococcal disease. These can be ordered from various organizations such as the Meningitis Research Foundation.
Complications
Prognosis is dependent upon the age, presence of co-morbidity, pathogen, delay in treatment and severity of neurological impairment at presentation. Streptococcus pneumoniae meningitis has a mortality as high as 37%, with meningococcal meningitis ranging from 3 to 13%. Up to one-third of patients develop complications (Box 3), some of which may not surface for years after recovery.
Complications of meningitis and meningococcal septicaemia
Death (10%) Hearing loss (7%) Cortical blindness Orthopaedic damage, including amputation Focal neurological deficits (hemiparesis, monoparesis and aphasia) Neurodevelopmental deficits (cerebral palsy and learning difficulties) Epilepsy, cerebral infarction and hydrocephalus Chronic organ damage Psychiatric and behavioural problems (bed wetting) Sleep disturbance and nightmares
Survivors should be followed up early to assess for long-term complications. Hearing tests should be conducted within 4 weeks of being fit to test, as ossification of the inner ear may limit successful cochlear implantation. These tests might need to be repeated and sometimes require referral from general practice. Follow-up from a psychological viewpoint is also important. One must never forget the emotional impact to patients and their families of being given a label of even ‘suspected meningitis’. Even if patients make a full recovery, they may continue to harbour long-lived anxiety towards medical professionals and illnesses in the future, however benign. GPs are well placed to offer long-term support and direct patients to the appropriate support agencies (Box 4). Depression is a common problem, so have a low threshold for screening and treating for this.
Useful meningitis support agencies and links
Meningitis Research Foundation-www.meningitis.org/
The Meningitis Trust-www.meningitis-trust.org/
HPA-www.hpa.org.uk/HPA/Topics/InfectiousDiseases/InfectionsAZ/1191942172836
Meningitis UK-www.meningitisuk.org
Prevention
At present all children in the UK are vaccinated against Neisseria meningitidis type C, Haemophilus influenzae and pneumococcus. Haemophilus influenzae type b (Hib) meningitis has almost been eliminated in many developed countries since routine childhood Hib vaccination started. The UK was the first country to introduce the meningitis C (MenC) conjugate vaccine in 1999, resulting in a 90% reduction in cases in the under 20 age group. Pneumococcal conjugate vaccine (PCV) produced similar results. There is currently no meningitis B vaccine available, despite this being more common and having higher mortality than MenC.
Remember that meningitis caused by these pathogens may still occur even in vaccinated people. This is particularly true in children under 2 years old due to their poorer antibody response. Furthermore, one must remember that patients immigrating from abroad may have a different vaccination history compared to UK residents.
Encephalitis
Encephalitis is the presence of inflammation within the brain with clinical evidence of neurological dysfunction. It is a rare condition and the average full-time UK-based GP may encounter one confirmed case every 15 years. All cases require notification.
Epidemiology
The worldwide annual incidence of encephalitis is between 3.5 and 7.4 per 100 000, and 1.5 per 100 000 in the UK. Viruses are the most common cause of encephalitis, with bacteria and fungi also being implicated (Table 4). Herpes simplex encephalitis (HSE) is the most common and important cause of encephalitis and has an incidence of two to four cases per million per year, with 90% resulting from HSV I and 10% due to HSV II. All ages are affected but there is an increased incidence in children and males.
Causes of encephalitis

Common in neonates and the immunocompromised
Pathogenesis
Pathogenesis is dependent on the virus involved but is generally characterized by a combination of direct cell destruction and a post-infectious immune-mediated response. Most viruses directly attack the brain parenchyma and neurons.
History
The diagnosis of encephalitis should be suspected in patients with acute onset of fever and headache progressing to altered consciousness and/or focal neurological signs/seizures. A detailed history from the relatives is required as patients may be confused or stuporous. Enquire about foreign travel and contact with people with infectious diseases. Certain animals may act as reservoirs for viruses, therefore a history of insect and animal bites may give clues to the underlying diagnosis. The past medical, vaccination and occupational history may reveal risk factors for particular pathogens such as Lyme disease in forestry workers. A preceding history of cold sores is not diagnostic of HSE as only 25% of patients with HSE have a history of cold sores, which is no different from the normal population.
Clinical features
Patients with encephalitis commonly present acutely with symptoms including:
Headache Fever (91% of patients with HSV I on admission) Cognitive and acute memory disturbances Behavioural change: disorientation, hallucinations, psychosis, agitation and personality changes Altered consciousness Focal neurology: hemiparesis, ataxia, aphasia, pyramidal signs, cranial nerve deficits and involuntary movements Seizures (33%)
Several caveats must be borne in mind however. Immunosuppressed patients may have subacute and chronic presentations. Furthermore, encephalopathy with or without fever may be precipitated by other infections and conditions outside of the CNS (Box 5). As with meningitis, the elderly may present with non-specific behavioural change, in the absence of fever, which may be mistaken for chest or urine infections, psychiatric illness or medication side effects. There is also usually a degree of co-existent meningeal inflammation (meningoencephalitis) therefore the diagnoses should be considered simultaneously.
A systemic physical examination should be performed looking for skin rashes (rickettsial fever and varicella zoster), mucous membrane lesions (herpes virus) and upper respiratory and chest findings (influenza and mycloplasma). Cytomegalovirus (CMV), varicella zoster virus (VZV) and Epstein Barr virus (EBV) may involve the peripheral nervous system, while polio, enteroviruses and Japanese encephalitis may cause myelitis.
Hospital management
All patients with suspected encephalitis need urgent hospitalization. The causative agent in around up to 75% of cases of presumed infectious encephalitis remains unknown. In spite of this, identification of a specific pathogen is important for prognosis, focusing treatment and public health intervention. Investigations are generally aimed at excluding other causes of encephalopathy and identifying the underlying cause. This generally involves FBC, U/Es, CRP, calcium, blood/viral cultures, chest x-ray, liver and thyroid function tests. Magnetic resonance imaging (MRI) may show some pathognomic changes particularly in HSE (Fig. 3). CT is a less sensitive but suitable alternative. Electroencephalogram (EEG) is recommended in all patients: with suspected encephalitis (Tunkel et al., 2008).

HSE: MRI brain showing T2 hyperintensity involving the right temporal lobe (‘bright’ areas). Neil Borden/SPL.
Causes of encephalopathy List is not exhaustive
Metabolic: hypoglycaemia, electrolyte imbalance and liver failure Hypoxia Epilepsy Trauma: head injury and intracranial lesions Raised intracranial pressure/space occupying lesion Alcohol withdrawal Vitamin deficiencies Systemic infections: urine/chest infections Drugs: sedative and opiates
LP and examination of CSF for PCR (HSV, VZV, EBV and enteroviruses), antibody detection and bacterial culture are crucial. Brain biopsy is reserved only for cases in which there is serious diagnostic doubt. Therapy is directed against HSV and VZV until a definitive cause is identified. This involves treatment with IV acyclovir in all patients as soon as there is a suspicion of encephalitis (IDSA, 2008). The use of steroids warrants further study, but they may be beneficial in patients with cerebral oedema and/or VZV encephalitis.
Mortality
Untreated HSE has a mortality of over 70%, with less than 3% of survivors returning to normal function. Early treatment reduces mortality to around 20–30%, with 50% having subsequent neurological disability. Delay in initiation of therapy of more than 4 days from start of symptoms leads to an adverse outcome. Rabies encephalitis is invariably fatal.
Neonatal HSE
This is typically caused by HSV 1 and rarely by HSV 2. Presentation is usually in the first week of life to 17 days, often with irritability, poor feeding, fever or focal seizures. Neonatal HSE tends to be diagnosed later and carry a high incidence of mortality and permanent neurological disability. Treatment is as in adult HSE but only around 30% of neonates survive without long-term neurological sequelae. Recommendations for the prevention of HSV transmission in pregnancy may be found on the British Association of Sexual Health and HIV (BASHH) website.
Prognosis
More than half of patients with encephalitis who are treated early and make good recovery may still suffer from residual neurological and neuropsychological impairment and disability; therefore, novel treatments are desperately needed. Morbidity associated with encephalitis is shown in Box 6.
Morbidity from encephalitis
Epilepsy (25%) Behavioural change (45%) Parkinsonism Dysphasia (41%) motor deficits Chronic amnesic states (69%) Chronic fatigue syndrome
Regular follow-up of these patients is necessary especially in children where behavioural problems such as depression and disinhibition may be problematic and require antidepressants. Useful aids for memory problems are available, including diary keeping, labelling items and the neuropage system (www.neuropage.nhs.uk). The latter sends reminder messages to a pager held by the patient to aid daily living.
Prevention
In the UK, children are routinely vaccinated against certain viruses that are associated with encephalitis such as measles, mumps, rubella and poliovirus. The varicella vaccine is available but does not form part of the immunization schedule. Patients intending to travel to areas with endemic causes of encephalitis should be counselled regarding specific vaccination for these, e.g. rabies and Japanese encephalitis. There is currently no vaccine for herpes simplex.
Key points
Meningitis and encephalitis are rare acute medical emergencies that carry high mortality and serious morbidity Early recognition and treatment is essential to reduce mortality and morbidity It is essential for doctors to be competent in administering initial antibiotic therapy in primary care in suspected meningitis and meningococcal disease Both conditions are notifiable diseases and cases should be reported to the CCDC or CPHM Survivors are often left with residual physical or neurological disability and GPs are well placed to provide long-term care and support for patients and their families