
Abstract
In the UK, there are 9 million people who are deaf or hard of hearing and potentially facing significant communication barriers. Hearing loss can be broadly divided into two main types—conductive and sensorineural. The former is usually caused by pathology within the external or middle ear, the latter by inner ear disease (the cochlea or neural pathway to the auditory cortex). A patient can also have a mixed picture with both conductive and sensorineural elements. This article describes the initial assessment and investigation of a patient presenting with hearing loss, outlines the more common causes of both conductive and sensorineural deafness and outlines strategies to optimize hearing.
The GP curriculum and hearing loss
To be able to manage primary contact with patients who present with hearing loss. The following are listed as important and common ear, nose and throat (ENT) conditions, all of which can contribute to hearing loss: earwax, otitis media, glue ear, otitis externa, cholesteatoma, perforated tympanic membrane, trauma involving the ear, foreign bodies within the ear, Ménière's disease and unilateral hearing loss in the absence of external ear pathology or obvious cause (e.g. acoustic neuroma). To have knowledge regarding the role of otoscopy, tuning fork tests and key specialist investigations (including pure tone threshold audiograms, speech audiometry, impedance tympanometry, auditory brainstem responses and otoacoustic emissions). Otoscopy and tuning fork tests are also listed as relevant psychomotor skills. To be aware of the screening programmes in place for hearing impairment To be aware of iatrogenic causes of ototoxicity
Communicating effectively with patients with hearing impairment as well as dealing effectively with parental concern (e.g. in children with glue ear) are listed as important communication and consultation skills.
The Newborn Hearing Screening Programme
One to two per 1000 babies are born with a hearing loss, most often into families with no history of deafness. Early identification is vital for optimal childhood development, particularly in terms of adequate speech and language.
A national screening programme for all newborn babies is now in operation across the UK, to try to facilitate early identification of hearing loss. Screening should be offered to parents of all babies and completed by 4 weeks of age for well babies in hospital-based programmes and by 5 weeks for those babies in community-based programmes. Babies who have been cared for on neonatal intensive care units for more than 48 hours should have screening completed by 44 weeks gestational age.
The screening test
The screening test, automated otoacoustic emission, is conducted by staff specially trained in hearing screening or the baby's health visitor. An earpiece is placed into the baby's ear sending a clicking sound to the cochlea. The test measures the resultant ‘echo’ produced by the inner ear if hearing is normal.
If the result of this test is inconclusive or unsatisfactory (commonly due to the baby being unsettled at the time of screening, background noise or a temporary middle ear effusion), a repeat test is offered at a later date. If this second test is also unsatisfactory, then the parents of the baby will be offered an auditory brainstem response screening test. The auditory brainstem response screening test records an evoked potential from the eighth cranial nerve, brainstem or auditory cortex with the use of electrodes placed on the skin, following acoustic stimulation of the cochlea.
Babies with normal screening tests
For babies with normal hearing screening tests, parents are provided with a checklist of milestones relating to speech and language corresponding to the different stages of development. They are advised to contact their health visitor or GP if they have any concerns about their child's hearing even in the presence of a normal screening test. Late-onset and progressive hearing loss make up a sizeable proportion of children with reduced hearing. Box 1 lists risk factors for hearing loss in childhood.
Childhood groups at risk of hearing loss
Birth factors
prematurity very low birth weight intraventricular haemorrhage neonatal jaundice use of aminoglycosides
Abnormal speech and language development Parents and siblings with hearing loss
Referral to audiology
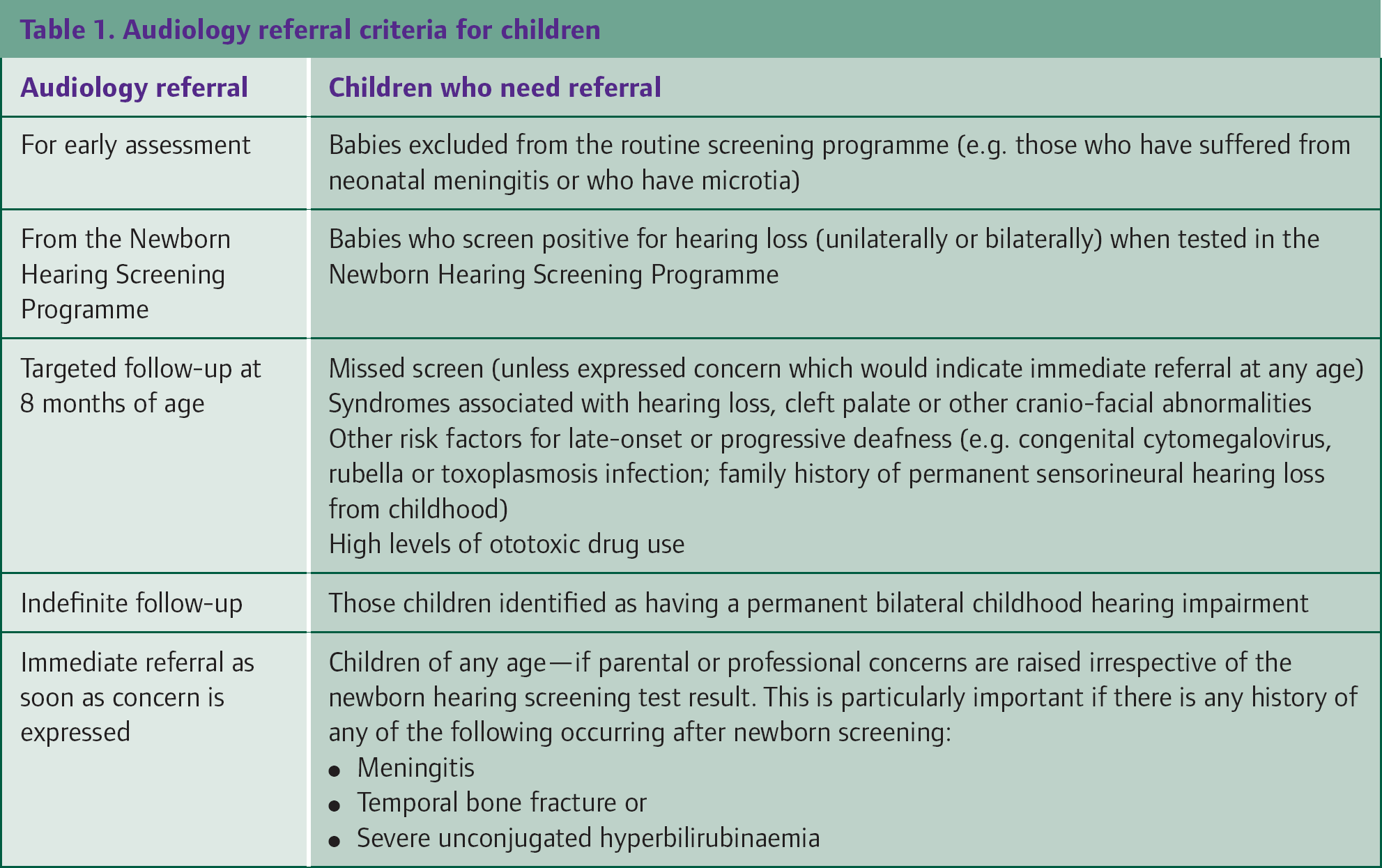
Table 1 lists criteria that should prompt referral for specialist audiology assessment.
Audiology referral criteria for children
Clinical assessment
There are a number of areas to explore when patients present with concerns about their hearing. These include:
Onset and rate of progression of hearing loss Whether the hearing loss is unilateral or bilateral Associated symptoms such as pain, discharge from the ears, tinnitus or imbalance
Ask about history of noise exposure, for example, as a result of occupation, while in military service or for recreational purposes. Enquire about past history of ear disease, injury or surgery, and take a full drug history looking for exposure to ototoxic agents. Ask about family history of hearing problems.
Children may present because parents or other professionals, such as teachers, have concerns about their hearing. However, they may present indirectly with symptoms that result from hearing loss. It is important to have a high level of suspicion for hearing loss in a child presenting with any of the following symptoms:
Slow general development and delayed milestones First word uttered late Small range of vocabulary for age Reduced verbal comprehension — may be noticed by parents/teachers Reduced attention span and concentration
Examination
Start your examination with inspection and palpation of the pinna and the surrounding soft tissues. Use an auroscope to examine the external auditory canal and the tympanic membrane. Examine the patient's neck and cranial nerves.
A gross evaluation of hearing can be made by whispering softly into a patient's ear while occluding the opposite ear (whispered voice test). Further assessment can be made with a 512 Hz tuning fork that is used for Weber's and Rinne's tests.
Weber's test involves striking the tuning fork and placing it in the midline of the patient's forehead. If the test is normal, the patient will hear the sound in the midline. Sound localizes to the affected ear in patients with conductive hearing loss and to the non-affected ear if the patient has sensorineural loss. If there is bilateral or symmetrical loss of either type, the sound is heard equally in both ears.
Rinne's test involves striking the tuning fork and comparing the intensity of sound when it is placed on the mastoid bone (bone conduction) compared to adjacent to the external auditory meatus (air conduction).
A Rinne-positive result (in which the sound heard by air conduction is louder than the sound heard via bone conduction) is the response in normal ears and also in those with a sensorineural loss in the test ear A Rinne-negative result (in which the sound heard via bone conduction is louder than that heard by air conduction) is the response seen if there is conductive hearing loss in the test ear
It is important to note that the picture can be complicated by a false-negative Rinne's test. This occurs when the patient has a profound sensorineural hearing loss (‘dead ear’) on the test side. The result is perceived as negative because there is no hearing at all via air conduction since the ear is ‘dead’. On bone conduction, however, the sound is transmitted not only to the ‘dead’ cochlea but also to the normal cochlea on the opposite side through the skull base, where it is heard. In specialist settings, masking of the non-test ear with a Barany noise box ‘occupies’ the non-test cochlea and hence allows a true-positive response.
However, a recent review article has concluded that both the Rinne and the Weber tuning fork tests are limited by inaccuracy and lack of precision data and so recommended that these tests should not be used for routine screening of hearing loss (Bagai et al., 2006). Instead, formal audiometric testing is recommended for any patient who has noticed a change in hearing. A whispered voice test is thought to be preferable for those patients not aware of any hearing impairment; audiology referral should follow if any hearing loss is detected.
Audiometry
There are a variety of audiological tests available. They can be broadly divided into objective (those not requiring a patient response) and subjective tests (where a patient response is needed). Impedance tympanometry, otoacoustic emission and auditory brainstem response testing are examples of objective tests. Pure tone audiometry and speech audiometry are subjective hearing tests. Referral is usually required to a specialist audiology service, but some practices do perform in-house pure tone audiometry and some health visitors are trained to perform otoacoustic emission testing.
Otoacoustic emission and auditory brainstem response have already been discussed within the context of newborn screening. Impedance tympanometry calculates the compliance or mobility of the tympanic membrane by varying the pressure in the external ear canal. Maximal sound energy passes through the eardrum when the pressure in the ear canal is the same as that in the middle ear. By varying the pressure in the ear canal and measuring the amount of sound reflected from the drum, the middle ear pressure can be determined. This is useful when screening for middle ear effusion and in the assessment of Eustachian tube function. The test produces a graph (Type A, see Fig. 1) where the peak coincides with the middle ear pressure. A negative middle ear pressure forces the peak to the left (Type C). Fluid in the middle ear produces a flat trace (Type B). An excessively tall peak indicates a hypermobile drum that may occur if there is ossicular discontinuity.
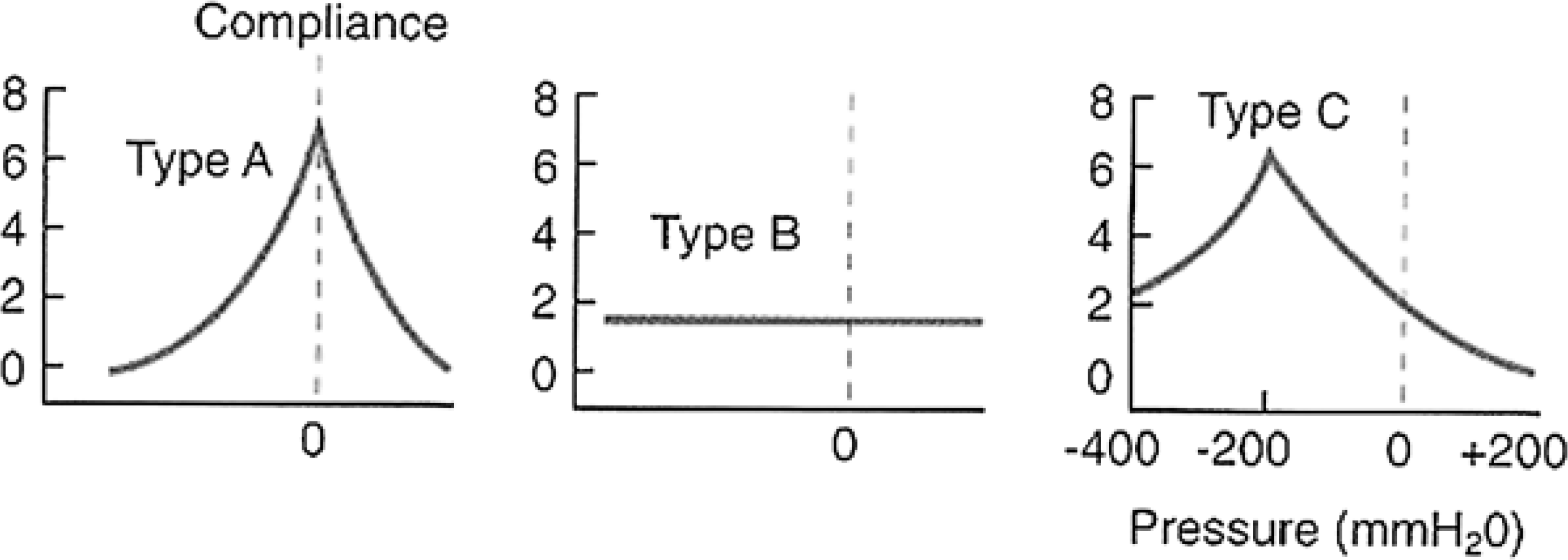
Typanometry (illustrating Type A, normal, Type B, middle ear fluid and Type C, negative middle ear pressure).
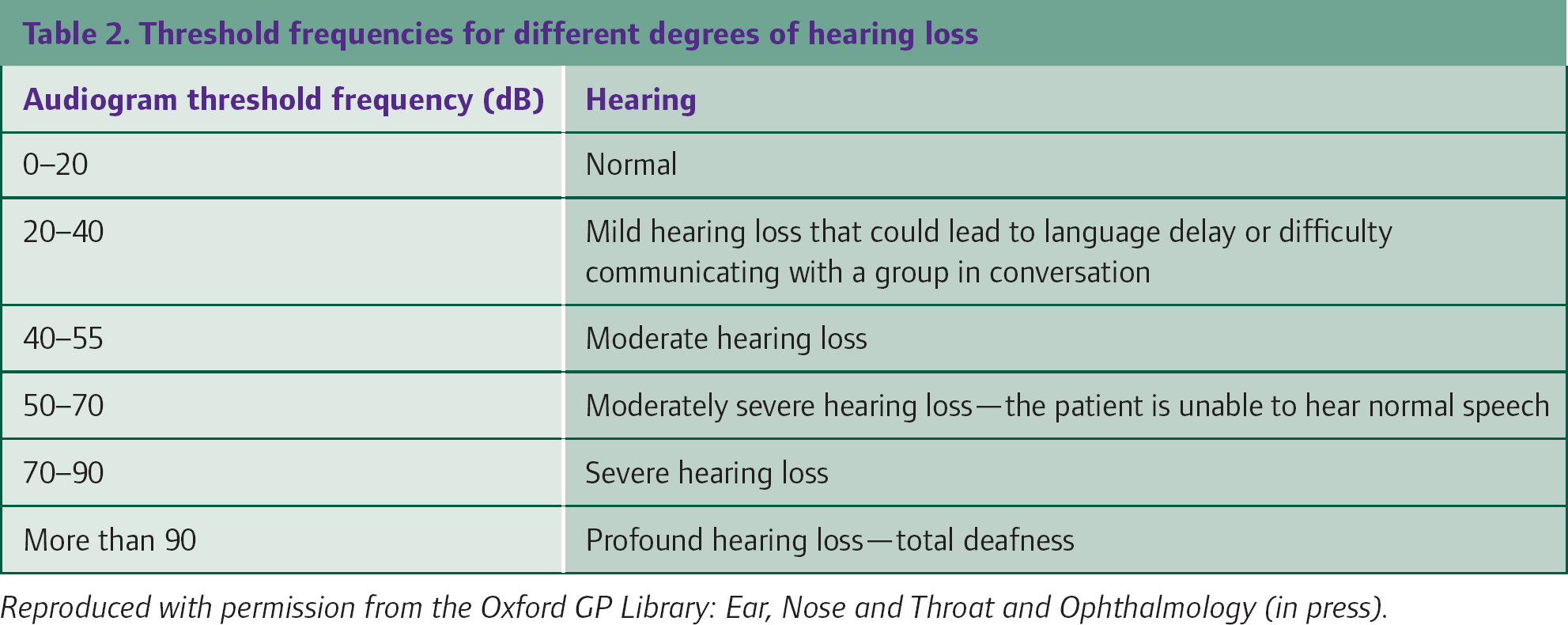
In pure tone audiometry, each ear is tested for air conduction and where necessary, bone conduction thresholds, with the use of headphones and a vibrator pad placed on the mastoid process. The results are plotted as a graph with hearing level in decibels (dB) on the vertical axis and frequency in Hertz (Hz) on the horizontal axis. Tests of the ‘normal’ population show that 95% have air conduction thresholds better than 25 dB over four frequencies. Fig. 2 illustrates a normal audiogram; the normal convention is for ‘x’ to denote air conduction on the left and ‘o’ air conduction on the right. Table 2 summarizes threshold frequencies for different levels of hearing loss.

Audiogram showing normal hearing in the left ear.
Threshold frequencies for different degrees of hearing loss
Conductive hearing loss is typically depicted with an ‘air—bone gap’, where a higher hearing level is associated with bone conduction in comparison to air conduction. When expressing bone conduction thresholds on an audiogram, the usual convention is for ‘]’ to denote bone conduction on the left side and ‘[’ to denote bone conduction on the right. It should be noted that it is not until the age of 3–4 years that a child will be able to cooperate with headphones and this type of testing.
Speech audiometry involves phonetically balanced words being presented to the patient at different volumes. The results are presented as a percentage score of correct answers. This is a useful tool for the evaluation of hearing aids.
Causes of conductive hearing loss
A summary of conductive causes of hearing loss is presented in Fig. 3.

Causes of conductive hearing loss.
Earwax
Occlusion of the external ear canal with wax is a common cause of hearing loss; just less than one-third of older people experience this at some time. The chances of wax accumulation are increased by the use of hearing aids and cotton buds to clean the ears.
A 5 day course of wax softeners is a useful initial step, these include olive oil or sodium bicarbonate 5% drops. In cooperative patients, and in the absence of previous or current tympanic membrane perforation, ear infection, current grommets or a history of ear surgery, wax may be removed mechanically via ear syringing. This usually takes place in the community and is performed by practice or district nurses.
Possible complications of syringing include perforation of the tympanic membrane, otitis externa, trauma to the external ear canal, pain, vertigo and tinnitus. It is important to tell patients about possible complications (providing a written information sheet is a good idea) and ask them to return if any of these symptoms are experienced. If patients are unsuitable for ear syringing or if syringing is unsuccessful, wax removal can be performed under direct vision in the secondary care ENT department.
Glue ear
Glue ear is the most common cause of conductive hearing loss in children. It is associated with Eustachian tube dysfunction and is not usually painful. On examination, the eardrum may look dull and there may be visible bubbles or a fluid level behind the drum. Risk factors for glue ear include:
Frequent ear infections or upper respiratory tract infections Atopy Smoking parents Enlarged adenoids and/or narrow nasopharyngeal dimensions Down's syndrome Cleft palate
The natural history of glue ear in children tends towards spontaneous resolution and so active observation over 3 months is the first management step, associated with advice on educational and behavioural strategies to minimize the impact of hearing loss. On review after this time, the National Institute for Health and Clinical Excellence (NICE, 2008b) recommends referral to an ENT specialist for consideration of ventilation tube (grommet) insertion if the glue ear still persists. Grommet insertion is indicated if:
There is persistent bilateral otitis media with effusion with a hearing level of 25–30 dB or worse in the better ear or There is evidence that the hearing loss is having a significant impact on the child's developmental, social or educational status
Hearing aids are a non-surgical alternative when surgery is either contraindicated or not acceptable. NICE do not recommend the use of antibiotics, decongestants or steroids in otitis media with effusion. Adjuvant adenoidectomy is not recommended in the absence of persistent or frequent upper respiratory tract infections. Grommets extrude after 3–12 months and review is required to recheck hearing. Up to 25% may require further grommet insertion.
In an adult, chronic serous otitis media, i.e. the presence of a unilateral middle ear effusion persisting for more than 3 months, has to be assumed to be due to a nasopharyngeal tumour until proven otherwise. Refer for urgent ENT review.
Otitis externa
Otitis externa is an infection of the external ear canal causing blockage of the canal through oedema and accumulation of infected debris. The most commonly associated pathogens are Pseudomonas aeruginosa and Staphylococcus aureus. Hearing loss resolves with the treatment of the infection, usually with a combination steroid and antibiotic drop. A previous InnovAiT article (Bajwa, 2009) provides a full overview of the presentation and treatment of otitis externa in the community.
Tympanic membrane perforation
Tympanic membrane perforations can be associated with infection or trauma. A tympanic membrane perforation may cause hearing loss in the affected ear.
In a patient with otitis media and a perforation, discharge will often be present in the ear canal. NICE (2008a) recommends immediate treatment with oral antibiotics (amoxicillin, erythromycin or clarithromycin) for children with acute otitis media and otorrhoea. Only when the ear is dry can accurate assessment of the perforation be made.
Most perforations heal spontaneously within 2 weeks. Therefore, plan a review of the patient after this time. If the perforation has not healed, monitor closely for any worsening of symptoms. Refer to an ENT surgeon if symptoms worsen or if there is a persistent defect at 6 weeks for consideration for surgical repair.
Exostoses
Exostoses are benign bony growths of the external ear canal that are often multiple and bilateral and usually close to the tympanic membrane. They are associated with a history of cold-water swimming. They rarely cause significant hearing loss and thus surgical removal is not usually required.
Otosclerosis
Otosclerosis is abnormal bone deposition on the stapes footplate and oval window causing fixation of the stapes footplate at this site. It is an autosomal dominant condition that is more common in women and in 85% of cases, both ears are affected. Symptoms present in early adult life (typically 20–40 years) and are progressive and become worse during pregnancy and in the menopause. Treatment of otosclerosis involves surgical repair by stapedectomy or alternatively the use of hearing aids.
There is also concern that the combined oral contraceptive pill (COCP) can make otosclerosis worse. The summary of product characteristics for many COCPs states that the use of a COCP is contraindicated if a patient has experienced deterioration of otosclerosis during pregnancy or with previous steroid use. However, a large contraceptive cohort study has not shown any significant association between the use of the COCP and otosclerosis. The Faculty of Sexual and Reproductive Healthcare suggests that women with otosclerosis who are anxious about the use of hormonal contraceptives may wish to consider an intrauterine device or barrier methods as alternative forms of contraception. Otosclerosis, however, does not feature as a risk factor in the UK Medical Eligibility Criteria (UKMEC) for combined oral contraceptive use.
Cholesteatoma
Cholesteatoma is an accumulation of squamous epithelium within the middle ear that is locally destructive. Conductive hearing loss caused by ossicular erosion is present in 90% of patients with cholesteatoma.
Cholesteatoma may be congenital or acquired and primary (an accumulation within a tympanic membrane retraction pocket) or secondary (ingrowth of skin through a tympanic membrane perforation). It has a distinctive pearly white appearance and is associated with unilateral foul smelling discharge unresponsive to treatment. Over time, cholesteatoma may expand to involve the mastoid, inner ear and facial nerve. Rarely, cholesteatoma can erode through the skull, causing meningitis or brain abscess and may even lead to death if not treated promptly. If suspected, refer the patient for a specialist ENT opinion.
Causes of sensorineural hearing loss
Box 2 lists the more common causes of sensorineural hearing loss. It is useful to classify causes as unilateral or bilateral since unilateral hearing loss should act as a red flag for more serious conditions (especially acoustic neuroma).
Causes of sensorineural hearing loss

Presbyacusis
Presbyacusis is a symmetrical progressive deterioration of hearing for high-pitched sounds with age (Fig. 4). It usually begins before the age of 30 years but is not usually noticed until there is difficulty with the hearing of speech. Hearing is most affected in the presence of background noise. The cause is a combination of inherited and environmental factors including lifetime noise exposure and tobacco use. It is a diagnosis of exclusion and hearing aids are the usual treatment.
Audiogram showing high-pitched hearing loss in the left ear in a patient with presbyacusis.
Noise exposure
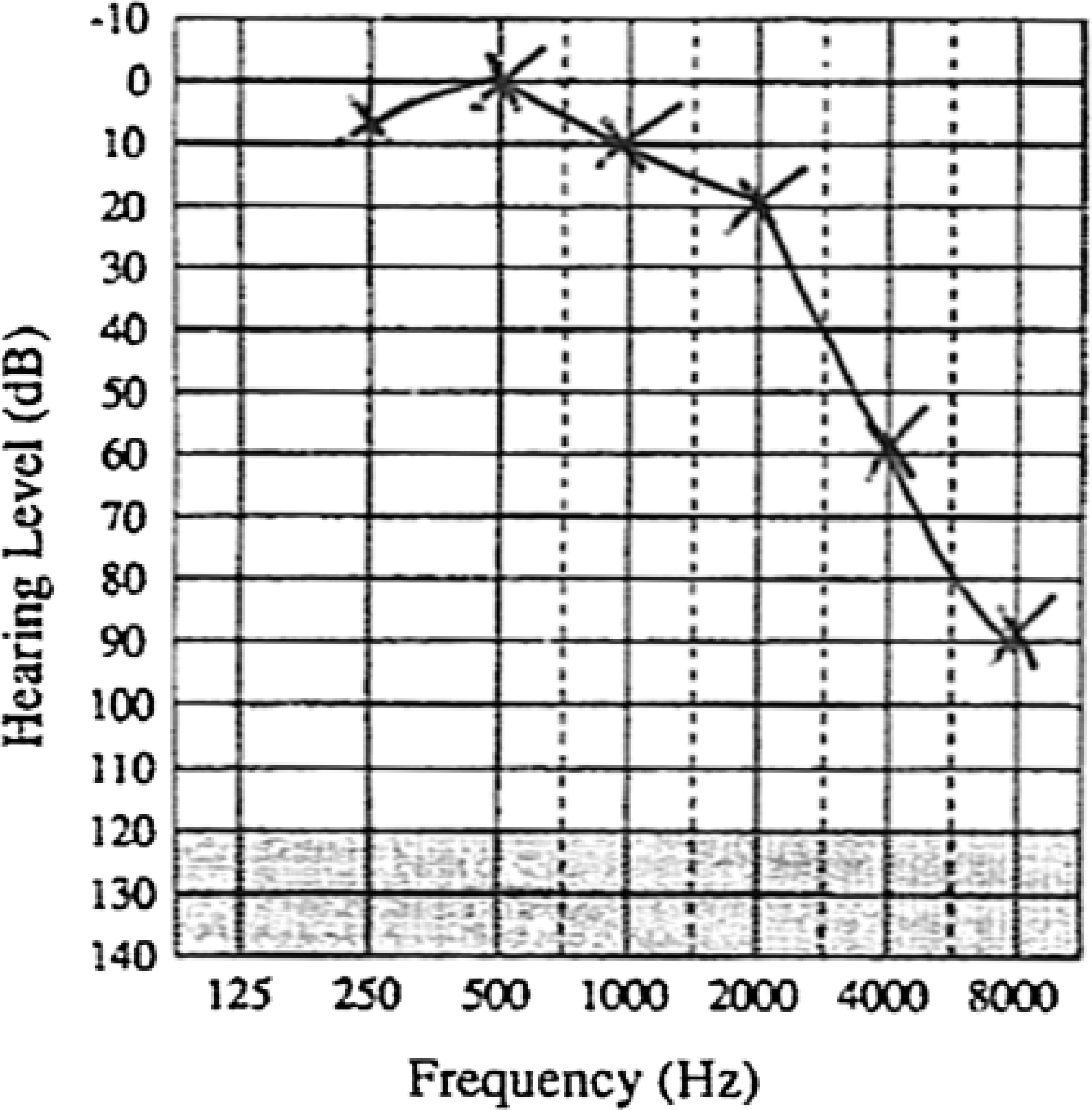
Hearing loss associated with noise exposure is the most common preventable cause of sensorineural deafness. The noise source may be identified from an occupational history and can include gunfire, explosions or loud music. Ear protection is required to prevent this form of hearing loss. High frequencies are affected first (typically 4000 Hz—Fig. 5) and hearing loss may be associated with high-pitched tinnitus.
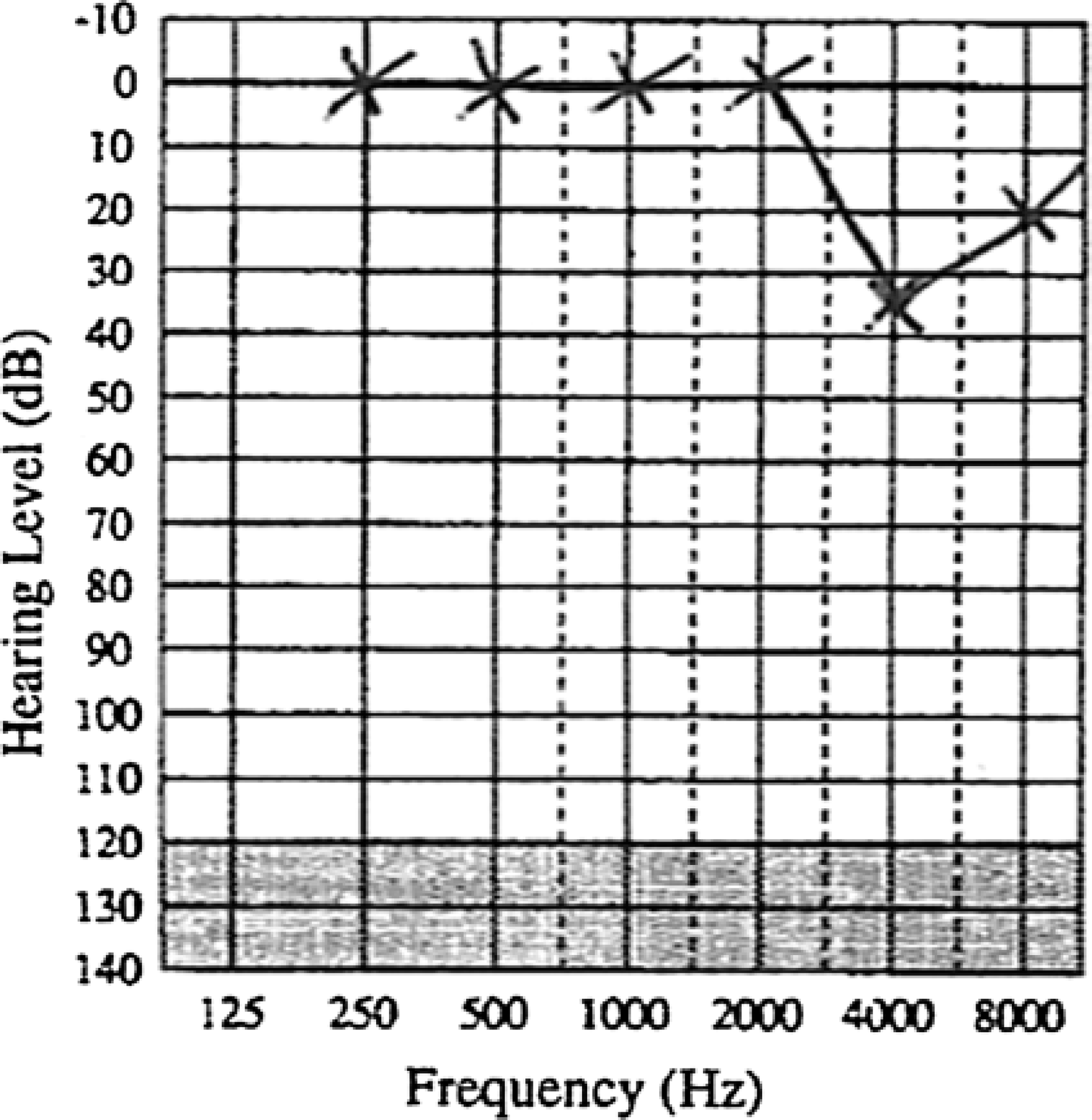
Audiogram showing noise-induced hearing loss in the left ear.
Occupational deafness is an industrial disease, and if deafness as a result of occupational exposure to noise is suspected, it is important to seek a specialist ENT opinion for specialist confirmation of the diagnosis. Patients with confirmed occupational deafness may be eligible for industrial injuries benefits. The patient's employer should be informed of any new diagnosis or Reporting of Injuries, Diseases and Dangerous Occurrences Regulations (RIDDOR) if the patient is self-employed.
Ototoxic agents
Ototoxic agents can result in sensorineural hearing loss. Such agents include aminoglycosides, diuretics, salicylates and many chemotherapy agents. These agents need to be administered with caution in the elderly, those with poor renal function or when a combination of ototoxic agents is required.
Ménière's disease
Ménière's disease is caused by dilatation of the endolymphatic spaces of the membranous labyrinth. It causes unilateral fluctuating hearing loss associated with tinnitus, aural fullness and episodic vertigo that can last up to 12 hours at a time. Initially, low-frequency hearing is affected but this progresses to include high-frequency sounds. Attacks often occur in clusters and vertigo tends to be the most prominent symptom. Symptoms tend to start in one ear but can progress to affect both.
Patients should be advised to inform the Driving and Vehicle Licensing Agency (DVLA) and driving must cease on diagnosis but may be recommenced once symptoms are well controlled. For vocational licensing, patients must be symptom free and controlled for 1 year before reapplication.
Treatment involves symptomatic relief from acute vertigo with antihistamines; diuretics are not recommended. Hearing aids are often ineffective as patients have poor speech discrimination and reduced tolerance to amplified sound. If patients are suffering from recurrent attacks, then specialist ENT referral is appropriate. Possible surgical interventions include vestibular neuronectomy (but this causes total ipsilateral deafness) or transtympanic instillation of gentamicin that usually avoids deafness.
Acoustic neuroma
Acoustic neuroma presents with unilateral sensorineural hearing loss usually in the absence of any external ear pathology. Any patient with asymmetric sensorineural loss needs specialist evaluation to exclude this diagnosis. Magnetic resonance imaging (MRI) is the current gold standard investigation.
Sudden sensorineural hearing loss
All cases of sudden sensorineural hearing loss require urgent referral for assessment and investigation since prompt institution of treatment improves the prognosis for hearing recovery. Diagnosis is made if there is a loss of at least 30 dB in three connected frequencies. Such hearing loss is unilateral in 90% of cases and can be associated with vertigo and tinnitus. Sixty percent of cases are labelled as idiopathic and many of these will recover spontaneously (often in the first 3 days but some cases can take up to 2 weeks). Other possible causes include:
Labyrinthine viral infection, such as cytomegalovirus or mumps Labyrinthine vascular compromise, such as in hypercoagulable states (Waldenstrom macroglobulinaemia) or as a result of emboli, following coronary artery bypass graft surgery for example Immune-mediated inner ear disease, such as Cogan syndrome
Treatment is controversial and empirical, often with steroids; most agree that if treatment is given, then it should be started within 48 hours of onset of the hearing loss.
Trauma
Barotrauma results from changes in atmospheric pressure (e.g. during air travel, while diving or as a result of direct trauma to the ear) in those with poor Eustachian tube function. It presents with a sensation of pressure or pain in one or both ears, conductive hearing loss and sometimes vertigo as well. Examination may reveal haemorrhagic areas in the tympanic membrane, fluid behind the eardrum or a perforated drum. Generally, spontaneous resolution occurs within 2–3 weeks. If a perforation has not healed within 6 weeks, or symptoms persist, refer for ENT review. To prevent barotrauma, patients with acute otitis media or known Eustachian tube dysfunction should be advised not to fly.
Temporal bone fractures can be associated with both conductive and sensorineural hearing loss. Sensorineural loss occurs if the fracture line involves the bony labyrinth. They can also be associated with facial nerve damage and cerebrospinal fluid leakage.
A perilymphatic fistula occurs when there is rupture of the round or oval window leading to leakage of perilymph into the middle ear. This can be caused by trauma but also following straining, lifting, coughing or sneezing. Patients describe an abrupt loss of hearing that can be associated with vertigo and tinnitus. Referral for surgical repair may be considered if symptoms are persistent.
Aids to hearing
There are a number of simple strategies that can be employed in order to improve communication with patients who are hard of hearing and who may rely partly on lip-reading:
Reduce background noise Use short sentences Place yourself at the same height as the patient Ensure that light falls on to your face and that your face and lips are not covered
In addition, routine daily life can be made easier by a number of environmental aids. These include changing doorbells to flashing lights and telephones can be fitted with volume controls or converted to be used with ‘T’ induction aids. Organizations providing support and advice to deaf people and their families are listed in Box 3.
Organizations providing advice and support for deaf people and their families
Royal National Institute for the Deaf. Website: www.rnid.org.uk
National Deaf Children's Society. Website: www.ndcs.org.uk
Electronic hearing aids
Many hearing aids are fitted with a ‘T’ setting that allows the use of electromagnetic induction waves to provide sound and cut out background noise. Most hearing aids are postauricular but can also sit within the ear or may be body worn in cases of severe hearing loss. Fitting aids to both ears is preferable to most patients. They may find that discrimination is not improved but they have better recognition of rhythms and phrases.
Common problems with hearing aids include acoustic feedback due to a poorly fitting ear mould and otorrhoea either due to otitis externa or an allergy to the mould. In cases of allergy, non-allergenic material can be tried or alternatively bone-anchored hearing aids (BAHAs) can be used instead.
The BAHA consists of a small titanium implant that is surgically inserted into the mastoid bone. A small screw is connected to this fixture through the skin and is itself connected to the external part of the BAHA. The external part contains a microphone, battery and processor. Some patients with severe hearing loss will have a body worn amplifier that connects to the BAHA. Patients using BAHAs report fewer cases of otitis externa and also experience less feedback compared to conventional air conduction hearing aids. However, the BAHA may not be able to provide as much power or such a high sound quality and so an air conduction aid is always the better option if possible. Other possible indications for a BAHA include malformations of the middle or external ear or conductive hearing loss in both ears that neither surgery nor conventional hearing aids would help.
Cochlear implants
Cochlear implants are used in patients with non-functioning cochlea but who have normally functioning auditory nerves. NICE recommend unilateral cochlear implants in adults with severe to profound deafness (only hearing sounds louder than 90 dB at frequencies of 2 and 4 kHz without hearing aids) who do not receive adequate benefit from acoustic hearing aids. They recommend bilateral implantation in children who fulfil the above criteria as well as adults who are also blind or have other disabilities that increase their reliance on auditory stimuli for spatial awareness.
The Disability Discrimination Act
Under the 1995 Disability Discrimination Act (DDA), it is unlawful to treat a person with hearing impairment less favourably than a person with normal hearing. In terms of health care, this means that reasonable adjustments need to be made in order to enable a hard of hearing person to use the provided service effectively. For example, this may mean the provision of communication support in the form of British Sign Language interpreters, lip speakers or note takers and the provision of an induction loop. Some Primary Care Trusts offer free interpreting services to GPs.
Key points
Deafness is a common problem that can have a huge impact on development within childhood and communication in adulthood The national Newborn Hearing Screening Programme is highly sensitive but may not detect late-onset or progressive hearing loss. Parental concern is an important trigger for referral of children to audiology at any age. Otitis media with effusion is the most common cause of hearing loss in children Unilateral hearing loss in the absence of external ear pathology or obvious cause warrants referral for the exclusion of acoustic neuroma Sudden sensorineural hearing loss should be assessed by an ENT specialist as a matter of urgency within 48 hours of onset