
Abstract
Glaucoma is a group of common sight-threatening disorders affecting the optic nerve and visual fields. It afflicts 2% of the population over the age of 40 years with an incidence of 2.5 per 1000 people per year and is the second most common cause of blindness in the UK. Incidence and consequent morbidity are increasing as a result of increased life expectancy. This article aims to provide an overview for GPs of the common types of glaucoma, their presentation and management.
The GP curriculum and glaucoma
Glaucoma is listed as a common and important condition within the knowledge base for
manage primary contact with patients who have an eye problem demonstrate an understanding of the importance of risk factors in the diagnosis and management of eye problems generate a differential diagnosis and formulate a management plan, which should include an assessment of severity and the need as well as urgency for referral to specialist services recognize and institute primary management of ophthalmic emergencies and refer appropriately coordinate care with other health and social care professionals to provide effective and appropriate care promote visual well-being by applying health promotion and disease prevention strategies explain the definition of blindness and partial sightedness, when and how to register a patient and facilitate access to sources of financial and social support describe the Driving and Vehicle Licensing Agency (DVLA) driving regulations for people with visual problems describe and be able to implement the key national guidelines that influence healthcare provision for eye problems, e.g. National Institute for Health and Clinical Excellence (NICE) guidelines for glaucoma.
Role of the GP
Management of glaucoma, with its many types, presentations and treatments, is a complex field that is mostly specialist led. Nevertheless, it is common and sight-threatening and GPs are often the first point of contact for the patient. The GP is also often responsible for ongoing prescription of medication and may be able to help the patient cope with a diagnosis of glaucoma. NICE (2009) identifies the following roles for GPs in the management of glaucoma:
Health promotion Helping to identify ‘at-risk’ patients Making appropriate referrals Supporting specialist management plans Educating and helping patients to make informed decisions Providing advice about matters such as driving regulations, how to register sight impairment and where to get additional support and benefits
Definitions and pathophysiology
Glaucoma is a non-specific term used for a group of ocular diseases that culminate in characteristic optic nerve head changes and typical defects in the visual field, with or without raised intraocular pressure (IOP). Glaucoma is classified by whether
it is congenital or acquired it is primary or secondary to another eye disease the IOP is elevated or not the drainage angle is ‘open’ or ‘closed’
Of patients with a diagnosis of glaucoma in the UK, about 70% have primary open-angle glaucoma (POAG), 10% have acute angle-closure glaucoma (AACG) and the remainder have secondary glaucomas.
The role of increased IOP
Ocular hypertension (OHT) is a consistently or recurrently elevated IOP of greater than 21 mmHg in the absence of optic nerve damage or visual field defect. This is a major risk factor for developing primary open-angle glaucoma (POAG). The pressure within the eye is a balance of the rates of aqueous production and drainage, as described in Fig. 1.

Aqueous formation and drainage. IOP is determined by the rate of aqueous secretion from the ciliary body and the rate of drainage. Secretion remains constant up to pressures of 50 mmHg. Ninety percent of outflow is via the trabecular meshwork that lies in the irido-corneal angle of the anterior chamber of the eye; 10% drains across the ciliary body (uveoscleral route). The angle is described as ‘closed’ when the iris obstructs its drainage. Courtesy: National Eye Institute, National Institutes of Health.
In open-angle glaucoma, there is increased resistance to outflow within the trabecular meshwork, which may be caused by a variety of mechanisms including:
Obstruction of the meshwork by foreign material (e.g. by cells or other debris) Loss of trabecular endothelial cells Reduction in trabecular pore density and size Loss of giant vacuoles in the inner wall endothelium of the canal of Schlemm Loss of normal phagocytic activity Disturbance of neurological feedback mechanisms
In angle-closure glaucoma, the iris is pushed forward against the posterior surface of the cornea and obstructs the drainage angle before the trabecular meshwork (Fig. 2).
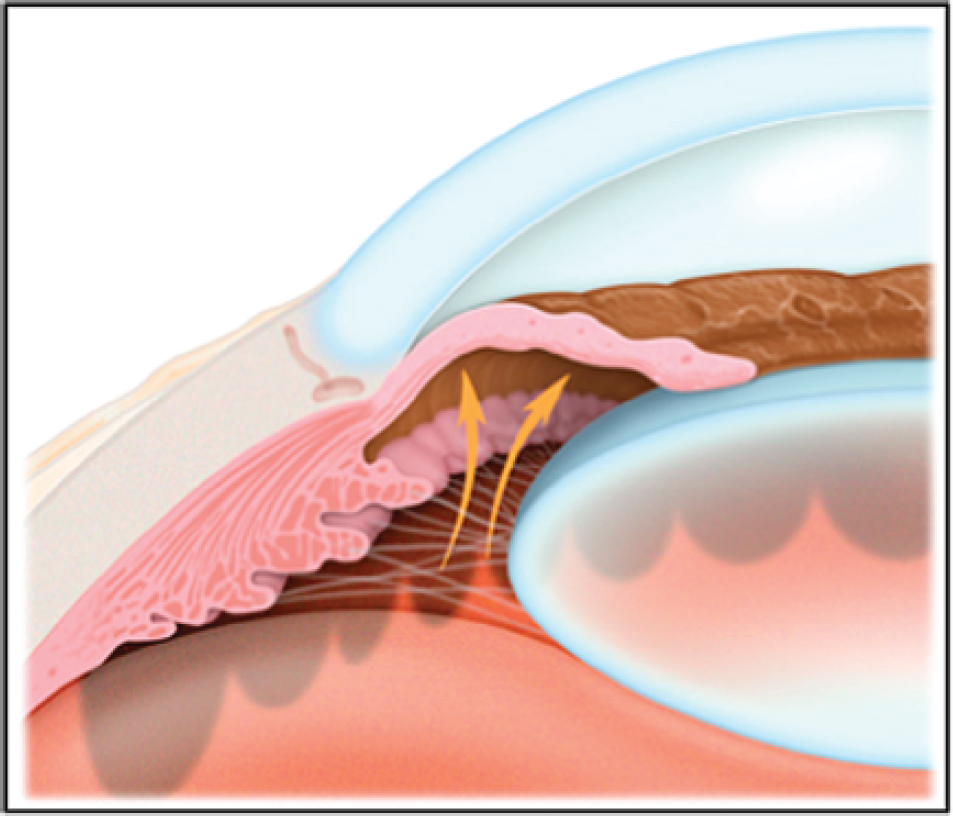
Angle-closure glaucoma.
Normal-tension glaucoma (NTG) is the development of glaucomatous characteristics without elevated IOP and is a diagnosis of exclusion after other causes for optic neuropathy have been ruled out. About 30–40% of those with POAG have IOPs of less than 21 mmHg. It is hypothesized that the absolute pressure within the globe is not as important as the pressure difference between the eye and the cerebrospinal fluid.
Optic nerve damage
It is hypothesized that damage to the optic nerve itself is caused via ischaemia, direct mechanical pressure or by optic nerve head remodelling either as a primary process or as a secondary response to local factors such as raised IOP, ischaemia or axonal loss.
Clinical features
Glaucoma can be regarded as a group of diseases that have a common end point. Patients have a characteristic optic neuropathy that is determined by both structural (optic disc) change and functional deficit.
Optic disc changes
The normal optic disc is circular and pink with a pale central depression. The pink (neuroretinal) rim of the disc contains nerve fibres, whereas the white cup is a pit devoid of them. A measure of the diameter of the cup in proportion to the total disc diameter is called the cup-to-disc (C:D) ratio. In healthy eyes, this is usually less than 0.5. As glaucoma advances, the cup enlarges and its sides steepen (Fig. 3) causing the C:D ratio to decrease. More specific for glaucoma than an enlarged cup is a growing cup or a disparity of greater than 0.2 between C:D ratios of both eyes (i.e. C:D asymmetry).

Glaucomatous optic disc changes.
Blood vessels enter the disc centrally and then course nasally following the edge of the cup. As the cup deepens and its sides steepen in glaucoma, the vessels angulate backwards and then turn along the excavated wall before angling back on to the floor of the disc. This is termed ‘bayoneting’.
Other changes suggesting glaucoma include
notching of the neuroretinal rim disc margin haemorrhages and the appearance of pigmentary changes around the optic disc, as well as a ‘see through’ ring of the retina around the optic disc (‘parapapillary changes’) making visible the underlying thick choroidal vessels and pale-coloured sclera
Visual field loss
Visual field loss (Fig. 4) is difficult to detect without automated visual field testing as the patient does not usually complain of blind spots, holes or tunnel vision. This is because (in the binocular patient) the brain creates a single image from dual stimuli, and visual field defects in one eye can be ‘filled in’ by a healthy corresponding field in the other eye. Tunnel vision is a very late presentation.
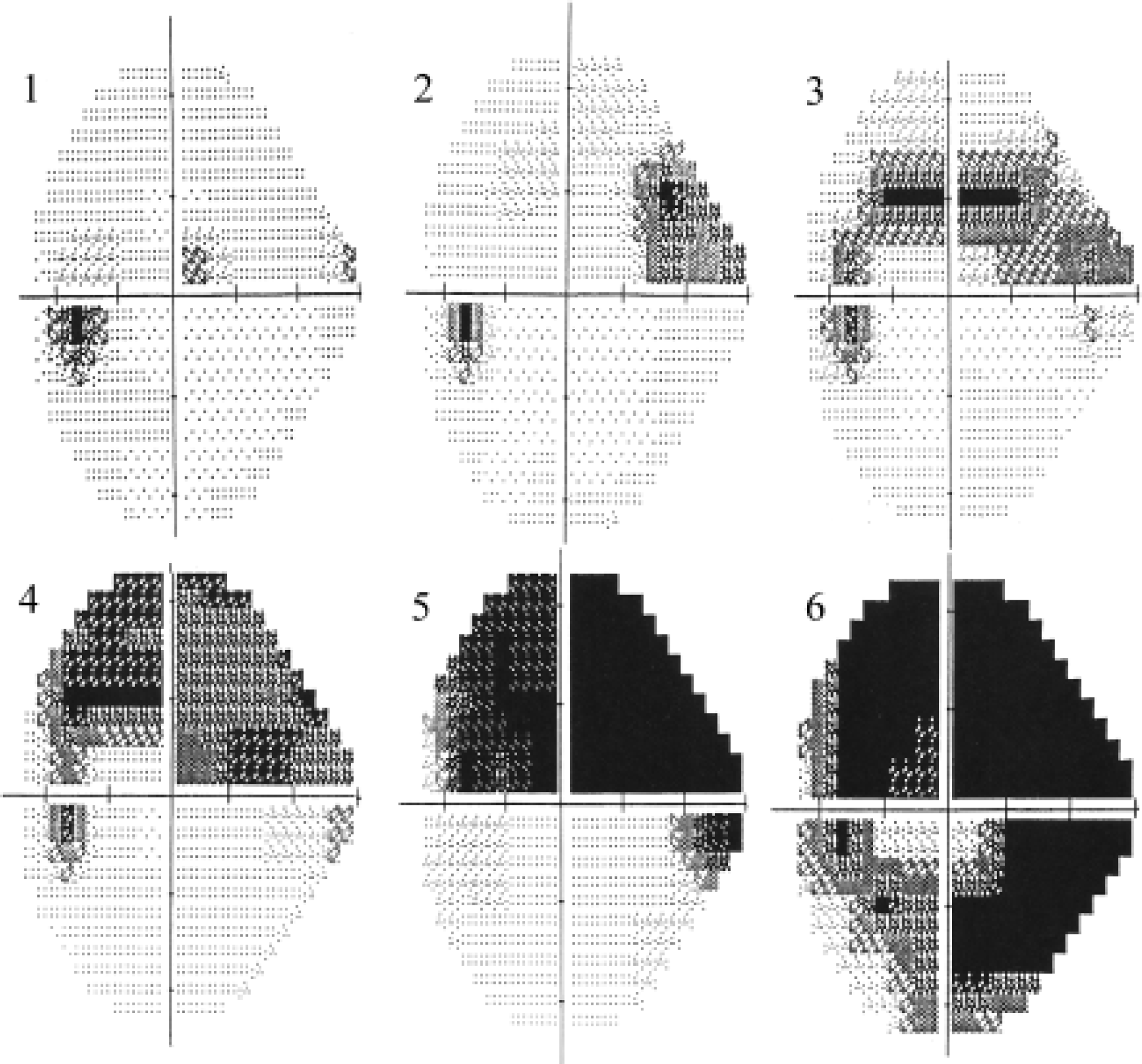
Left eye field defects over time in a patient with glaucoma. Visual field testing by confrontation is unreliable because it is subjective, crude and non-standardized. Glaucoma clinics use automated visual field analysers, which can either use stationary or moving lights of varying intensity known as static (e.g. Humphrey) or dynamic (Goldmann) perimetry. The classic progression of defects, as detected by a Humphrey's visual field analyser, is displayed here: (1) superior-nasal paracentral, (2) nasal step, (3) arcuate shaped, (4) enlargement, (5) deepening and (6) ring scotoma.
Primary open-angle glaucoma
POAG (synonymous with chronic open-angle glaucoma) represents almost three-quarters of all forms of glaucoma and accounts for over a million ophthalmic outpatient appointments annually and 10% of UK blindness. It has an insidious and progressive course and patients only complain of visual field symptoms once damage has occurred bilaterally. Once sight is lost, it cannot be restored. Box 1 lists conditions that should be considered when a patient presents with visual field defects.
Differential diagnoses for visual field defects.
Glaucoma Some types of optic atrophy, e.g. Leber's hereditary optic neuropathy Causes of papilloedema (but classically an enlarged blind spot) Retinal abnormalities, e.g. retinitis pigmentosa and choroido-retinitis Acute ischaemia, e.g. migraine Bilateral lesions of the anterior calcarine cortex Hysteria
NICE guidelines for the diagnosis and management of POAG and OHT in adults were published in April 2009. They do not cover angle-closure glaucoma, secondary glaucoma or adults with childhood glaucoma. These guidelines emphasize that management of glaucoma is a specialist field and should not be undertaken without the necessary specialist training and experience.
Risk factors for POAG
GPs are ideally placed to identify ‘at-risk’ patients and advise them to visit an optician for a glaucoma check. Although the precise cause of POAG has not been identified, risk factors include
elevated IOP (greater than 21 mmHg) age greater than 40 years family history—patients with a family history of glaucoma over the age of 40 years are entitled to free National Health Service (NHS) eye tests race myopia
Raised IOP is the most important known risk factor for the development and progression of glaucoma. Elevated IOP alone, however, does not constitute POAG. Those without clinical signs of glaucoma but with IOPs ranging from 24 to 31 mmHg have an average 10% risk of developing glaucoma over the following 5 years.
POAG is more common in older individuals. Most cases present in the over 65s and it is unusual to diagnose POAG under 40 years of age. Two percent of people aged over 40 years have POAG and this rises to 10% in white Europeans over the age of 75 years. The average age of diagnosis is 69.1 years for Caucasians and 63.7 years for Afro-Caribbeans.
The risk of POAG is greater than 4–10 times higher for individuals with an affected relative; the closer the relative, the greater the risk. The genetics and pattern of inheritance are uncertain, but there is probably an interaction of several genes and environmental factors too. Although there is an available test for one of the identified genes (Myocilin), only about 3% of all POAG is caused by single-gene defects and therefore testing is only really useful in those already identified as being ‘high risk’.
POAG is three to four times more likely to occur in people of Afro-Caribbean origin than in Caucasians. It tends to be more advanced at time of diagnosis and is six times more likely to cause blindness in Afro-Caribbeans than in Caucasians. Note that this is different for acute angle-closure glaucoma (AACG), as opposed to POAG, where it is the Asian population who are most at risk because of a predisposition to shallow anterior chambers.
Near-sighted (myopic) patients have a 2- to 3-fold increased risk of POAG. The higher the myopia, the stronger is the association with glaucoma. This contrasts with far-sightedness being a risk factor for AACG.
Most studies support a weak association between diabetes and POAG. Whether or not it is a significant risk factor for glaucoma is controversial. In the USA, all diabetics are screened for glaucoma. Diabetic proliferative disease with vessels spreading on to the iris (rubeosis iridis) is a distinct form of secondary glaucoma.
On average, people of Afro-Caribbean origin have thinner corneas than Caucasians. Patients with a corneal thickness less than 555 microns have a 3-fold greater risk of glaucoma than those with corneas thicker than 588 microns. Consequently, corneal thickness measurement (pachymetry) is an important part of the workup in secondary care. In addition, since IOP is determined by a measurement of the force needed to flatten the corneal surface, a thinner cornea will give a ‘falsely’ low IOP reading, and for the same measured pressure, the threshold for treatment is lower in patients with a thinner cornea.
Screening
A national programme for glaucoma screening does not exist in the UK at present. This is because there is no single reliable screening test available. Visual field testing and IOP together are the ‘best-choice’ screening test combination. Static automated perimetry tends to only identify abnormality after a significant number of optic nerve axons have already been damaged and so detect changes too late to be a useful screening test. Optic nerve head assessment lacks sufficient specificity.
Therefore, detection of potential cases of POAG relies on a clinical suspicion (based on the history and risk factors identified) or on opportunistic finding by an optometrist performing an NHS eye test. GPs have an important role to alert ‘at-risk’ patients that
it is important to have regular eye tests for early disease detection they may be eligible for free eye tests (Box 2) patients already on glaucoma medication should be monitored regularly at intervals stipulated by the specialist
Criteria for ‘free NHS eye tests’.
All patients in Scotland are entitled to free NHS eye tests. In England and Wales, a patient is entitled to a free NHS eye test if
over 60 years (or under 16 or under 19 years and in full-time education) over 40 years with a glaucomatous first-degree relative or if advised by an ophthalmologist that he/she is at risk of glaucoma diagnosed as having diabetes or glaucoma registered blind or partially sighted prescribed a complex lens, e.g. bifocals qualified for income-based exemptions
There are two parts to the free NHS eye test:
assessment of visual acuity (VA) and checking general eye health that usually includes pressure measurement and fundoscopy
If there is a raised IOP or a family history, the optometrist may also perform perimetry. Beware of certain chains of opticians that offer ‘free-for-all’ schemes but which may only include VA in the free test.
Referral
Patients with suspected glaucoma may be referred to ophthalmology for specialist confirmation of POAG and advice on further management either directly by their optician or via their GP. All patients with raised IOP or changes in the optic disc or visual fields suggestive of glaucoma should be referred.
Investigations
Beyond referral to the optician for VA, IOP and visual field testing, there are no other investigations that should be done in primary care. Baseline evaluation in secondary care involves VA testing, slit lamp biomicroscopy, applanation tonometry (IOP measurement), gonioscopy (iridio-corneal angle visualization), ophthalmoscopy, perimetry (automated visual field analysis) and assessment of central corneal thickness.
Medical treatment
The main goal of treatment is to prevent further optic nerve damage while avoiding harmful drug side effects. The only proven method to prevent disease progression is by reduction in IOP, even if the IOP is normal at presentation.
The specialist ophthalmologist sets a target pressure (typically a 30–40% drop in IOP) on the basis of the severity of optic nerve damage, the current IOP, the speed of disease progression and the general health of the patient. The adequacy of the target is determined by monitoring optic nerve changes and visual fields. It is uncommon for progression to occur with IOPs below 16 mmHg.
Most medications work by reducing aqueous secretion, by increasing drainage or a combination of both. Medications are usually topical preparations in the form of eye drops, but a few are systemic. The decision about which drugs to use depends on the type and severity of glaucoma, the patient's medical history (e.g. beta-blockers may be contraindicated in patients with asthma or bradycardia), drug side effects and patient concordance. Table 1 lists common drugs used for glaucoma treatment and summarizes their important side effects.
Summary of glaucoma medications

A common side effect to most topical drugs is irritation or allergy causing conjunctivitis and associated hyperaemia. Systemic side effects to topical drugs can be reduced by lacrimal punctal occlusion or closing the eyes for 3 minutes after instillation. No agents are recommended in pregnancy or breastfeeding.
Only beta-blockers and prostaglandin analogues are licensed for first-line treatment in OHT and POAG. Usually, the specialist prescribes the lowest possible dose with the least frequent dosing regime for the desired effect. If there is insufficient effect, then the medication is withdrawn and substituted with an alternative. If there is still a treatment failure, then another medication is added or a switch is made to a combination treatment (see Box 3).
Combination eye drops for glaucoma.

Key: beta-blocker;
carbonic anhydrase inhibitor;
prostaglandin analogue;
alpha-2 agonist
GPs may be asked questions about how patients should administer and look after eye drops (Box 4). Figure 5 shows the recommended technique for instilling drops. A common cause for failure of treatment is non-compliance, which is thought to occur in up to 25% of cases. If IOPs are proving hard to control, it is worth checking how often a repeat prescription is being requested on the practice computer.

Instilling eye drops and then punctal occlusion: good technique maximizes efficacy and can reduce systemic absorption by up to 50%.
Advice for patients on use of topical eye preparations for glaucoma.
Allow at least 5 minutes between using different eye preparations to avoid ‘wash out’. Order of use of different preparations should be thinnest first and gel or ointment last. Instil drops as directed by the specialist ophthalmologist: into the correct eye, at the right dose, at the right time.
Topical treatments may give rise to systemic effects—close the eyes and practise punctual occlusion after instillation of eye drops to minimize systemic absorption (Fig. 5).
Use eye preparations safely and hygienically and store correctly (e.g. refrigerated)—in particular, note the date of opening and when the medication needs replacing.
Seek medical help if:
Persistent local side effects, e.g. red eye Possible systemic side effects, notably shortness of breath, light-headedness, faints, palpitations or rashes Potentially unidentified drug interactions or contraindications to current glaucoma therapy Struggling to comply with dosing regime Pregnant (or breastfeeding)
Laser treatment and surgery
Trabeculoplasty is the process of using a laser to coagulate the trabeculum that paradoxically increases aqueous outflow by causing contractures that open up neighbouring ‘pores’. The effects have a delayed onset and only last for a few years but are useful when medical compliance is poor, polypharmacy is a problem or if trying to avoid surgery (e.g. because the patient has a short life expectancy).
Trabeculectomy is a form of surgery augmented with mitomycin or 5-fluorouracil, which involves making a fistula between the anterior chamber and the outside of the sclera and which creates a visible pearl-like drainage bleb on the surface of the eye. It achieves much greater and more stable pressure drops and is used when medical or laser treatments have failed or when disease is advanced and requires very low IOP targets.
Follow-up
Once diagnosed with POAG, individuals need lifelong specialist monitoring and follow-up. This varies typically from monthly to yearly, depending on target pressures and disease progress.
Acute angle-closure glaucoma
AACG is a sight-threatening medical emergency. The risk of blindness is much greater for patients with AACG than POAG even though there are fewer cases. Globally, about 10% of diagnosed POAG patients are bilaterally blind, but the figure for AACG is almost 25%. It only takes a few hours at very high pressure (around 50 mmHg) to cause blindness.
AACG results from a sudden blockage of the drainage angle of the eye. There is a consequent rapid and dramatic increase in IOP that, if left untreated or if recurring intermittently, can cause irreparable optic nerve damage.
Pathogenesis of AACG is not fully understood but the most widely accepted theory is that there is a pre-existing contact between the central iris and the lens, which produces a slight pressure difference between the anterior and posterior chambers. As the pupil dilates, the peripheral iris becomes floppier and bulges forward under pressure from the posterior chamber. It eventually comes into contact with the cornea and obstructs the drainage angle (see Fig. 2).
Risk factors and triggers of AACG
The classic precipitant event of AACG occurs when the iris dilates either in response to dim light (e.g. at the cinema), accommodation for near vision or eye drops (e.g. anticholinergics, sympathomimetics and rarely even miotics). Rare cases have been associated with antidepressant medications and rapid correction of hyperglycaemia. Certain individuals (particularly Asians and Eskimos) are more prone to attacks than others because the anatomy of their eyes predisposes to a ‘tighter’ drainage angle (shallow anterior chamber, anteriorly situated or larger lens, shorter axial length/long-sightedness or a thin floppy iris).
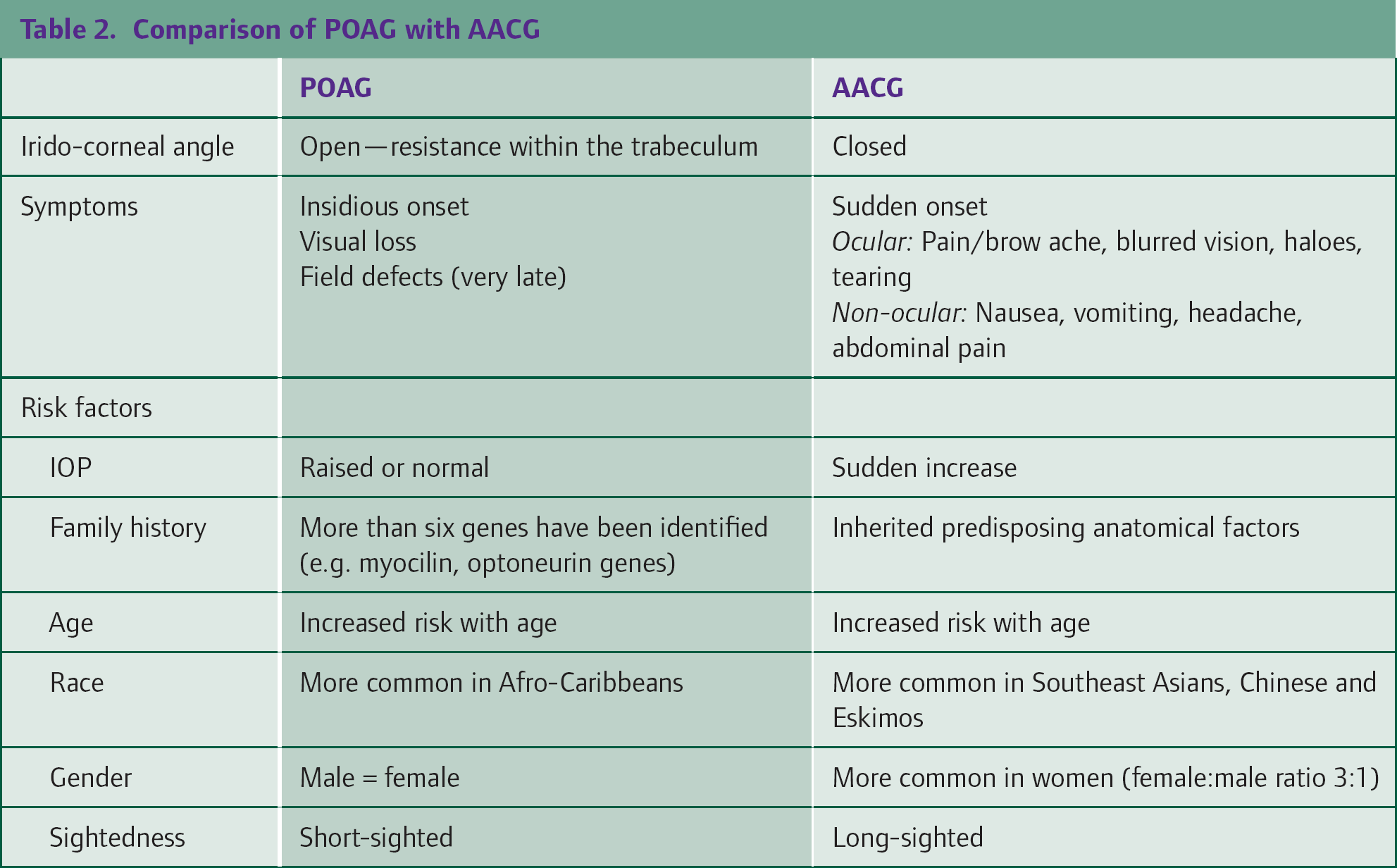
Prevalence is 2–4/100 in Eskimos, 1/100 in Asians and 1/1000 Caucasians. Meanwhile, women tend to have shallower anterior chambers and are thus three times as likely as men to suffer AACG, except among Afro-Caribbeans, where there is equal prevalence between the sexes. Risk also increases with age because the lens grows continually throughout life. Table 2 compares risk factors and features of AACG and POAG.
Comparison of POAG with AACG
Symptoms of AACG
Usually, the patient with AACG presents with predominant ocular symptoms, such as painful ‘red eye’, blurred vision, haloes around lights and profusely watering eye. Commonly these are acute onset, unilateral and associated with headache, nausea, vomiting and even abdominal pain. Sometimes, the non-ocular symptoms are the main complaints and patients may be misdiagnosed with migraine or an acute abdomen. The diagnosis is even less clear if there is a more gradual or intermittent history.
Signs of AACG
Clinical examination in the GP surgery may reveal an eye which is red (Fig. 6), especially around the cornea, and an iris which is mid-dilated and fixed or poorly reactive to light. The cornea may be relatively hazy compared to the ‘good’ eye because of corneal swelling, which contributes to the blurred vision. It may even be possible to detect a shallow anterior chamber simply by shining a light from the side and comparing the anterior depth of each eye. On palpation, the eye feels hard and rock-like.

Red eye of AACG: Hazy/oedematous cornea (due to hydrostatic pressure) and unreactive or sluggish, mid-dilated slightly oval pupil.
Referral
Refer any patient with suspected AACG as an emergency to a specialist eye unit. The patient should be transported ideally lying supine (so that lens falls away from the iris), and eye patches should be avoided as they will enhance dilation and maintain the attack.
Investigations
Once in secondary care, the ophthalmologist will be able to confirm findings, exclude other conditions that might elevate IOP and check for more subtle features of AACG with specialist equipment. Investigations likely to be performed include tests for
elevated IOP (via tonometry) occluded drainage angles (via gonioscopy) adhesions between iris and cornea, iris atrophy or ‘glaucoma flecks’ on the lens (with slit lamp biomicroscopy) and optic disc swelling if acute or disc ‘cupping’ if recurrent and long-term AACG (via ophthalmoscopy)
Specialist treatment of AACG
In the specialist setting, the aims of treatment are to reduce IOP (using systemic acetazolamide, a topical beta-blocker, an alpha-agonist and/or osmotic agents), suppress inflammation with topical steroids and reverse angle closure with a topical miotic such as pilocarpine. Pain and vomiting are treated symptomatically because they increase IOP. Definitive treatment may require peripheral laser iridotomy, which is the creation of a hole in the iris to allow drainage of fluid by-passing the pupillary blockage.
Complications of AACG include permanent visual loss, recurrence, attacks in the other eye and retinal vein or artery occlusions. For this reason, patients should be followed up long term by an ophthalmologist.
Secondary glaucoma
Secondary glaucomas are those that are consequent of another disease process (see Box 5). The most common pathogenesis is the obstruction of outflow by particulate matter within the trabecular meshwork (e.g. inflammatory cells, red cells or lens material) or by chronic changes in the lens, iris and/or meshwork that result in a tighter drainage angle.
Examples of secondary glaucomas.
Inflammatory glaucomas, e.g. uveitis of all types Lens-related glaucoma
Angle-closure with mature cataract Lens capsule rupture or lens subluxation Phacolytic glaucoma (lens particles block the trabecular meshwork) Traumatic glaucoma Hyphaema Angle recession glaucoma Post-surgical glaucoma
Neovascular glaucoma, e.g. rubeosis iridis
Drug-induced glaucoma, e.g. steroids/'steroid responders’
Glaucoma of miscellaneous origin, e.g. intraocular tumours and severe chemical burns
The presentation of secondary glaucoma is as varied as the disorders with which it is associated. In some instances, there may be no symptoms, ocular or otherwise. Alternatively, secondary glaucoma may present in a non-specific way, such as vomiting. Therefore, from a GP perspective, it is important to be aware of the possibility of secondary glaucoma, especially in those with relatively common systemic inflammatory conditions, such as reactive arthritis, inflammatory bowel disease, ankylosing spondylosis and psoriatic arthritis.
Eye trauma also requires a special mention because glaucoma may occur following a relatively ‘minor’ injury, for which the patient does not seek hospital or acute medical attention. If in doubt, the GP should refer to the eye department for review. The specialist will follow-up with serial examinations and tonometry. If red blood cells are present in the anterior chamber (i.e. ‘hyphaema’; Fig. 7), they may occlude the trabecular meshwork in the short term. However, in the longer term, scarring within the angle itself may set up a chronic process inhibiting aqueous outflow.

Hyphaema—there is an 85% chance of raised IOP developing if the surface of the hyphaema reaches the inferior level of the pupil.
Advice about driving with glaucoma
All drivers must have good central VA and adequate peripheral vision. For a Group 1 entitlement (normal private car or motorbike), this means:
Being able to read a post-2001 number plate from 20 m with both eyes open, with or without glasses. This equates to 6/10 vision. Unfortunately, no such line appears on a Snellen chart and Snellen acuity is a poor predictor: in one study, 26% of patients with 6/9 vision failed the number plate test, while 34% with ‘poorer’ 6/12 vision passed it. Anyone with glaucoma should have a peripheral field of vision of 120 degrees on the horizontal meridian and there should be no significant defect within 20 degrees of the central fixation point (as determined by automated perimetry). Anyone who has bilateral visual field defects is legally bound to inform the DVLA. If only one eye is affected and the other eye is perfectly normal, then it is not necessary.
It is the patient's responsibility, and not that of any healthcare professional, to inform the DVLA of any condition likely to affect driving. Once informed, the DVLA will contact the patient's eye specialist for details and sometimes arrange further visual field testing.
Group 2 vehicles (heavy goods vehicles and passenger carrying vehicles) have more stringent standards and patients who wish to drive these vehicles should seek advice from the DVLA.
Partial sight and blindness registration
Registering with the local authority can make it easier for people with restricted vision to get practical support from social services. Registration entitles the patient to concessions and benefits, such as tax allowances (£1890 in 2009/10), discount travel (bus pass/rail card), parking and television licence concessions. Registration is voluntary.
To be registered, a patient must be certified as ‘severely sight-impaired’ (blind) or simply ‘sight-impaired’ (partially sighted) by a consultant ophthalmologist (Boxes 6 and 7). Usually, this will happen automatically if the patient is already under the hospital eye services, but if the patient is not known to the hospital, then the GP will need to refer the patient. If the patient is dissatisfied with the eye specialist's certification (or indeed a DVLA decision), then the patient is able to seek a second opinion or appeal to the Magistrate's court.
Severely sight-impaired (i.e. blind) criteria.
Any one of the following with glasses:
Less than 3/60 VA with a full visual field 3–6/60 VA with a severe reduction of field of vision 6/60 or better VA but with reduced visual field, especially if missing lower hemispheres
Sight-impaired (i.e. partially sighted) criteria.
Any one of the following with glasses:
3–6/60 VA with a full field of vision Less than 6/24 VA with a moderate reduction of visual field or central scotoma or blurriness
Key points
Glaucoma is a group of disorders affecting the optic nerve and visual fields Glaucoma is the second most common cause of blindness in the UK and prevalence is increasing because of our ageing population POAG has an insidious course and only becomes symptomatic after significant bilateral and irreparable visual field loss has already occurred AACG is a medical emergency and a sight-threatening cause of painful red eye with reduced VA that requires urgent admission Glaucoma management is a specialist field and all patients with glaucoma should be under specialist ophthalmology follow-up GPs have a role in detection of glaucoma, referral for specialist management, providing ongoing prescriptions for glaucoma treatments, support and advice about rights and responsibilities