
Abstract
This article focuses on providing an overview of severe learning disability. We seek to define learning disability and look at the aetiological basis for severe learning disability in the UK. We will look at the important role that GPs play in diagnosis and long-term management of people with severe learning disability.
The GP curriculum and learning disability
Demonstrate an awareness that there will be a few individuals with special needs accessing services with moderate, severe and profound learning disabilities who need to be identified, monitored and reviewed appropriately
Demonstrate an awareness of likely associated conditions and the knowledge of where to obtain specialist help and advice
Demonstrate an awareness of the particular importance of a person-centred approach when consulting, often with communications involving carers
Demonstrate the ability to optimize communication through the use of consulting skills and communication aids
Demonstrate an awareness of the concept of diagnostic overshadowing
Demonstrate an understanding of the impact of the doctor's working environment on the care provided to PWLD, e.g. the measures taken to compensate for sensory impairment
We will explain and discuss relevant concepts such as baseline change and diagnostic overshadowing. This article will also outline strategies, which can be adopted to improve consultation and thus outcome when engaging with people with severe learning disability.
Introduction
PWLD make up about 2% of the UK population, approximately 985 000 individuals (Valuing People, Department of Health, 2001). Of this group, nearly 210 000 are severely or profoundly learning disabled. PWLD in general and those with more severe learning disability in particular face major hurdles to inclusion in our society. Improving the quality of life of PWLD is a national aim as highlighted by strategies such as Valuing People Now (Department of Health, 2009).
Reports such as Death by Indifference (Mencap, 2007) have highlighted the widespread obstacles encountered by people with severe learning disability seeking health care that include stigmatization, communication barriers, poor health care access and limited social opportunities. PWLD are known to suffer from greater medical and psychiatric morbidity than the general population and those with severe learning disability find themselves particularly affected. The most common co-morbid conditions include epilepsy, cerebral palsy and neurological impairment (Hand, 1994). Autistic spectrum disorders, mobility problems and sensory impairment are also significantly over-represented in those with severe learning disability.
The move to the community and deinstitutionalization of PWLD over the last 30 years has resulted in the increasing importance of the role of the GP. GPs have key roles in both diagnosis and ongoing management of health conditions in PWLD. It is important therefore for GPs to be aware of the classification, associated co-morbid conditions and approaches to the management of PWLD.
Classifying disability and recognizing people
Diagnosing learning disability involves the assessment of intellectual quotient (IQ) and evaluation of a person's adaptive behaviour (the ability of an individual to carry out everyday life skills that include personal care and communication). An IQ level of less than 70 combined with demonstrable impairment of adaptive behaviour prior to the age of 18 years makes a diagnosis of learning disability likely.
IQ levels may be directly determined by psychological testing such as the Wechsler Intelligence Scale or indirectly assessed by the use of scales such as the Vineland Adaptive Behavior Scale. Table 1 outlines the levels of learning disability, which have been correlated to corresponding IQ, level and approximate mental age.
Severity of learning disability and IQ levels

While the term learning disability has been used in the UK since 1991, the International Classification of Disease (ICD-10) refers to learning disability as mental retardation. Given the social unacceptability and stigmatization of the term mental retardation, the term learning disability is preferred in the UK. Learning disability may also be referred to as intellectual disability; however, this is discrete and separate to learning difficulty and a term used to identify specific difficulties in learning, the most well known of which is dyslexia.
When we refer to severe learning disability in this article, we refer to PWLD whose IQ is less than 35 and who fall either into the severe (IQ between 20 and 34) or profound classification categories (IQ less than 20). While the current ICD-10 classification system has strengths, for example, in planning services for PWLD, it overlooks individual strengths and weaknesses. Thus a person-centred approach is of great importance in understanding the ideas, concerns and expectations of PWLD, their families and carers.
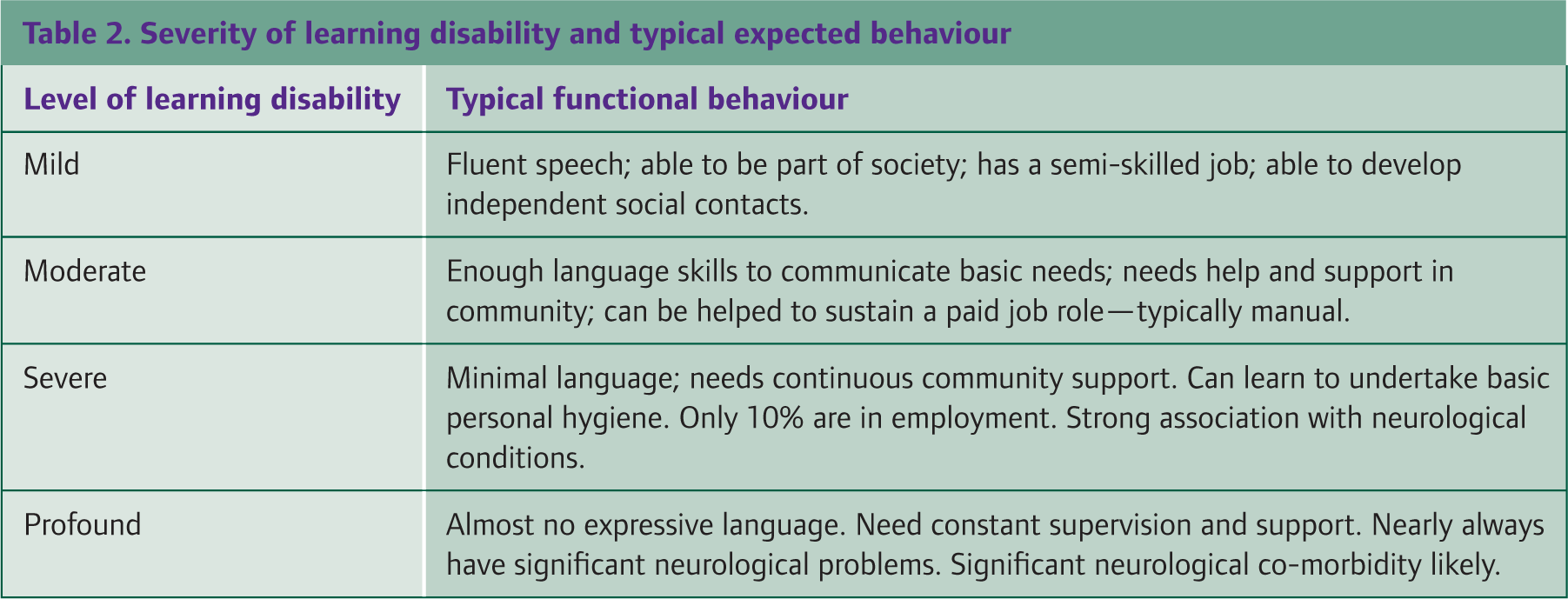
People with more severe learning disability tend to have poorer functional ability. People with severe learning disability often find themselves needing specialized care combined with close supervision. Table 2 outlines typical functional behaviours as correlated with severity of learning disability. While those with severe learning disability may be taught very basic tasks, such as personal care, such accomplishments are difficult to achieve among those with profound learning disability. People with profound learning disability may require extensive training for activities such as eating. We should also consider that every person is an individual and improvements in a person's environment and support may result in greater functional abilities.
Severity of learning disability and typical expected behaviour
Aetiological considerations
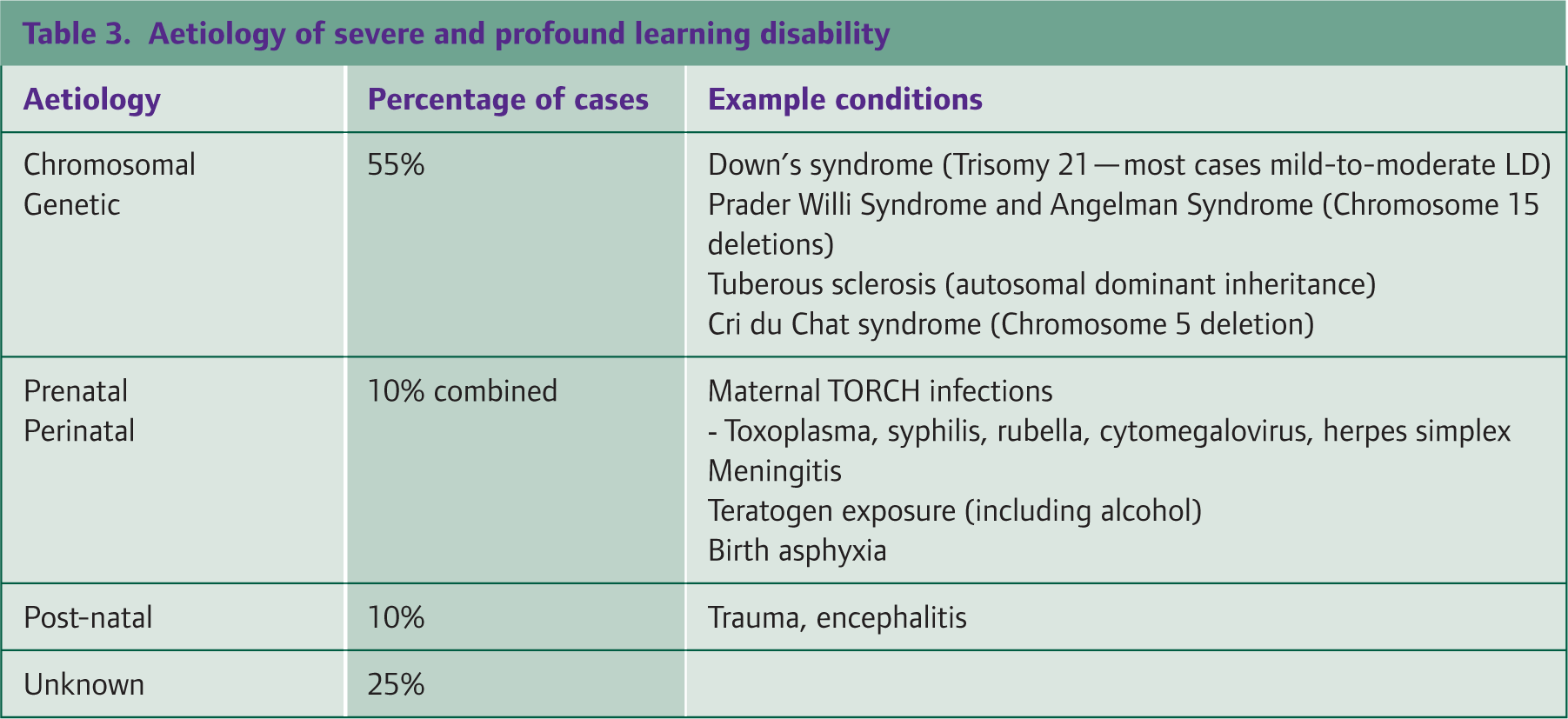
Diagnosis of learning disability is based on IQ and impairments in adaptive functioning as opposed to aetiology. While genetic factors, maternal infections and birth trauma are known aetiological factors, in approximately 30–50% of cases, the cause of the learning disability is unknown. Severe learning disability is more closely linked to aetiological factors, especially chromosomal abnormalities. In those with severe or profound learning disability, approximately 55% of cases are due to chromosomal and genetic abnormalities. A further 10% are caused by prenatal and perinatal factors and 10% may be attributed to post-natal factors. In 25% of cases, no specific cause is known. Table 3 summarizes the aetiology of severe and profound learning disability.
Aetiology of severe and profound learning disability
Physical and mental health
PWLD experience greater medical and psychiatric co-morbidity in comparison to the general population. Those with severe disability experience even greater co-morbidity. The Lavin et al. (2006) study into life expectancy in PWLD demonstrated those with severe learning disability to have the shortest life spans. The profoundly learning disabled lived on average to 29 years.
Many conditions are known to disproportionately affect those with severe learning disability. The most common group of conditions experienced are neurological complications such as epilepsy and cerebral palsy. It is thought that the basis of severe learning disability and its strong association with neurological conditions stems from a common aetiology of underlying brain injury.
Epilepsy
While lifetime risk of epilepsy is between 3 and 5% in the general population, between 7 and 15% of those with mild to moderate intellectual disability, 45–67% of those with severe and 50–82% of those with profound learning disability have epilepsy (NHS Evidence: Learning disability). Conditions such as tuberous sclerosis and Angelman syndrome are both associated with severe learning disability and are associated with epilepsy in 80–90% of cases (Pelc et al., 2008; Thiele, 2010). PWLD often have epilepsy with more than one seizure type and experience seizures that are more resistive to anti-epileptic medication.
Sensory impairment
Those with severe learning disability also suffer from high rates of sensory impairment including visual and hearing difficulties. Unfortunately, as highlighted by Kiani and Miller (2010), these conditions are under-recognized by carers and under-diagnosed by clinicians. A Dutch study by Van den Broek et al. (2006) found that over 92% of people with severe or profound learning disability had visual impairment, the majority of which remained unnoticed by their carers.
Psychiatric illness
The association between learning disability and psychiatric illness is more complex. Psychiatric morbidity among PWLD is higher in comparison with the general population. A recent study by Morgan et al. (2008) involving over 11 000 PWLD revealed rates of psychosis, in particular schizophrenia to be significantly higher among PWLD. They also found that PWLD with severe psychiatric illness have earlier contact with services and more frequent and lengthy inpatient stays compared to people with severe mental illness but without learning disability. While mood disorders are not uncommon among PWLD, currently it is not clear whether these occur at rates above those in the general population.
Autistic spectrum disorders
It is well recognized that pervasive developmental disorders such as autistic spectrum disorders are more common among PWLD. Bhaumik et al. (1997) found an association between severity of learning disability and number of autistic traits present, which is in keeping with previous research, suggesting that autistic spectrum disorders are increasingly prevalent with decreasing IQ.
Self-injury and aggression
PWLD may undertake repeated self-injuring behaviour or be aggressive to others. While these activities may occur on the background of a specific aetiological condition such as the hand biting seen in Lesch—Nyhan syndrome, they may also occur in PWLD of unknown cause. Sadock et al. (2009) outline key aspects that should be explored in both aggression and self-injury, which include the situational nature of the behaviour, the chronicity of their development, the function served by carrying out such actions and if the actions are localized to a particular location—such as hitting the right side of the head in the case of a right-sided otitis media.
Gustoimages/SPL

Primary care perspectives
A significant proportion of PWLD have not been formally diagnosed and are not in contact with health care services. However, people with severe learning disability are more likely to be receiving help and support from health care or social services. It is important to be aware that the Quality and Outcomes Framework (QOF) has a learning disabilities domain that currently awards practices points and thus payment for producing a register of patients aged 18 and older with learning disabilities. There are also learning disability Directed Enhanced Services (DES) in place throughout the UK, although the detail of service requirements varies according to whether your practice is in England, Scotland or Wales. The core aim of the DES is an annual health check of PWLD registered with a general practice. The health check is a review of physical and mental health with referral if needed. Areas of particular focus include:
Health promotion
Chronic illness and systems enquiry
Physical examination
Epilepsy
Dysphagia
Behaviour and mental health
Specific syndrome check
Check on the accuracy of prescribed medications
Review of coordination arrangements with secondary care
Review of transition arrangements if required.
Understanding baseline change
When a person with severe learning disability is brought into clinic, it is important to think holistically and assess biological, psychological and social factors when undertaking an assessment. Clinicians should seek to identify if a change in behaviour has been noted and if there are any possible triggers that may explain a new or recurrent presentation. The concept of baseline change is important when we look at assessing a patient with severe learning disability. Baseline change looks to see if a person's current behaviour is different to their normal baseline behaviour. For example, a young man who grinds his teeth and has been doing so for the last 10 years may be unlikely to have an acute presentation of illness; however, if his teeth grinding had only occurred over the last 2 days coupled with other changes in behaviour, then a medical or psychiatric cause would need to be ruled out. Figure 1 outlines possible factors that may contribute to changes in baseline behaviour in a person with severe learning disability.

Factors influencing changes to baseline behaviour.
Barriers in primary care
GPs are often the first physicians to be consulted when concerns are raised regarding either the developmental progress of a child or an older individuals' functional ability. It is recognized that there are several barriers in primary care that hinder diagnosis and management of learning disability and co-morbid conditions. These were outlined by Lennox et al. (1997) and include:
Communication difficulties between the doctor and patient
Communication difficulties between health professionals
Difficulties with accessing the health care system
Difficulties that short consultation times have on history taking
Negative attitudes held by the medical professionals
GPs' limited view of their role and responsibilities as health care providers for people with intellectual disability.
Despite these challenges, there are steps that can be undertaken to seek to overcome these barriers. In people with severe learning disability, communication difficulties are a particularly significant barrier. Allowing for a longer consultation combined with use of simple language will help facilitate communication. Use of audio-visual aids such as demonstrating the use of an otoscope or thermometer on a carer coupled with reassurance can also be productive in enhancing the interaction between patient and GP and improving compliance with physical examination.
Referring to a specialist
First presentations of learning disability may occur in primary care. Referrals from primary care to secondary care services for suspected learning disability among 2- to 6-year-old children tend to be as a consequence of speech and language delay. Older children tend to present with more global impairment of their functioning. These factors underscore the importance of having a sound knowledge base of children's developmental milestones. Prompt referral for further assessment should be undertaken if clinical abnormalities are noted or caregiver concerns persist, so that potentially treatable causes can be investigated and managed. For example, in the case of speech and language delay, differential diagnosis may include psychosocial deprivation, autistic spectrum disorders and hearing impairment (congenital or acquired).
GPs are gatekeepers to secondary care services, which include community paediatrics, child and adolescent mental health services and learning disability services. Availability and organization of services vary widely throughout the UK and familiarization with local services would be of significant benefit. Once diagnosed, PWLD, especially those with severe learning disability continue to require support and input. Despite involvement of community services such as learning disability services, GPs continue to be key in liaising with services, raising concerns, treating medical conditions and acting as advocates for PWLD.
While it is important to attempt to engage PWLD directly, often carers have to be consulted to provide collateral history. Carers can be variable in their experience and knowledge, making consultation potentially challenging. It should be recognized that caring for a person with severe learning disability can be stressful. Efforts should thus be directed toward providing help and support to both formal (paid) and informal (unpaid) carers alike.
Assessment of symptoms
As mentioned previously, there is a heavy burden of medical and psychiatric co-morbidity among PWLD. In those with severe learning disability, the symptomatology may be particularly difficult to ascertain and may be less familiar to GPs. Clinicians also need to be aware of the concept of diagnostic overshadowing, which causes changes in behaviour and function to be falsely attributed to learning disability rather than the underlying medical or psychiatric condition.
Like medical co-morbidity, assessment of psychiatric co-morbidity in people with severe learning disability can be difficult. Clinicians may have to rely on more objective evaluations of behaviour and function as opposed to psychological symptoms, which are voiced less commonly than in the general population. Depression, for example, may present with crying, sleep disturbance and weight change as the most prominent symptoms. Case study 1 outlines Sarah's story, which highlights how depression may present in a person with severe learning disability. Case study 2 tells of Daniel's story of early-onset dementia in a person with Down's syndrome.
Despite limited consultation time, GPs are in a unique position to promote engagement and concordance with long-term management plans, including educational, social and medical interventions. Establishing a good rapport with patients, families and carers can foster better health-seeking behaviour for people with severe learning disability and enhance willingness to engage with services.
Recognizing that both patients and their carers may require support in accessing services such as housing and benefits, and proactively raising these issues, enhances the quality of life experienced by people with severe learning disability.
An issue of capacity
People with severe and profound learning disabilities should not be assumed to lack capacity. This is one of the principles of the Mental Capacity Act 2005 (MCA). A person who lacks capacity refers to someone who is unable to make a particular decision or take a particular action for themselves at the time the decision or action needs to be taken. Hence, capacity is decision specific and thus needs to be assessed for every decision.
Case study 1
Sarah is a 34-year-old woman with severe learning disability. She also suffers from cerebral palsy as a result of a birth asphyxia following a complicated delivery. She has poor vision and has always been wheelchair bound. She resides in a learning disability nursing home where she needs continuous supervision and care.
Recently, staff noted that Sarah would at times appear tearful, appear less interactive and more sleepy than normal. They also noticed that she did not seem as interested in food during meal times. The carers consulted Sarah's GP since the next appointment with learning disability services was several months away.
The GP noted that Sarah's main carer for the past 4 years had recently left the home, and Sarah's symptoms had begun shortly thereafter. Sarah's GP suspected depression; however, she ordered a range of blood tests to rule out other conditions that might account for Sarah's symptoms such as anaemia or hypothyroidism. Following normal results, the GP discussed the case with the specialist looking after Sarah who suggested a trial of fluoxetine.
Over the next month, staff noted Sarah to be more lively and interactive, with no further episodes of crying. A member of the learning disability team visited Sarah and recorded a marked response and improvement with the antidepressant.
Case study 2
Daniel is a 40-year-old man with a learning disability secondary to a diagnosis of Down's syndrome. His mother is his principal carer and has noticed some gradual changes in Daniel's behaviour over the last few months. His sleep has been disturbed and she has begun to find him wandering around the house at night. He has also had difficulty carrying out regular activities such as bathing himself and now requires her help.
Daniel attends a day centre nearby. Staff there have reported to his mother that over the past month, they have noted that Daniel is more unsettled and irritable than normal.
His mother decided to consult his GP. After taking a careful history, the GP suggested the possibility of dementia. The GP explained to Daniel's mother the association between Down's syndrome and early-onset dementia and arranged a series of blood tests including thyroid function tests to rule out medical causes of Daniel's symptoms.
The GP subsequently referred Daniel to the local Learning Disability Service where a diagnosis of dementia was confirmed. Daniel's behaviour continued to deteriorate and eventually he moved into a group home for PWLDs as his elderly mother was struggling to cope at home. He continues to receive input from both the Learning Disability Service and his GP.
The MCA also reiterates the right of every person to be supported to make a decision for themselves. In people with severe and profound learning disability, this will invariably mean involving the primary carer and family who know the individual, their preferences and the best ways to communicate with them. This will include communication with gestures, body language and simple signs/words that carers and family will be familiar with. This may also relate to using pictures in communication, allowing enough time and making use of specifically designed material that are available to facilitate decision making.
The MCA places a duty on the decision maker (who could be a GP) to consult other people when making decisions in a persons' best interest when they lack capacity. This includes anyone the person has previously named as someone they want to be consulted, anyone involved in caring for the person, anyone interested in their welfare (family carers, close relatives or an advocate already working with the person), an attorney appointed by the person under a Lasting Power of Attorney or a deputy appointed for that person by the Court of Protection. When there is no one to consult about the person's best interests, the person may need an Independent Mental Capacity Advocate (IMCA).
The MCA also states that individuals must not be judged unable to make a decision merely because their decisions are seen as eccentric or unwise. It is not necessary for people involved in the care of PWLD to agree with the individuals' decisions. Any decisions taken or acts performed should be in a way that is least restrictive of the person's rights and freedom of action.
Useful links
There are several websites, which may provide useful and wider background information on PWLD, and these are outlined in Box 1.
Useful websites and resources

Key points
People with severe learning disability face many barriers to inclusion in society
Medical co-morbidity and mortality are higher among people with severe learning disability than people with milder learning disability
Sensory impairment and speech impairment are common among those most severely learning disabled
Improving access and quality of health care for PWLD is a Royal College of General Practitioners and a Department of Health priority
GPs are in a unique and important position to help support people with severe learning disability, their families and carers.