
Abstract
There are a number of common oral problems (COPs) that patients may consult their GP about. Some patients are concerned about the appearance of structures within their mouth that are manifestations or variants of normal anatomical structures and only require reassurance. The majority of oral mucosal conditions are benign and do not represent any sinister pathology or an underlying systemic condition. This article describes the clinical presentation of some common oral lesions and conditions. Guidance is given concerning their management and when referral to an oral specialist is required. Recurrent mouth ulcers are the subject of another article in this journal.
The GP curriculum and oral health
Variants of normal oral anatomy
The mouth has a number of soft tissue structures that may concern patients but are manifestations or variants of normal anatomy. These include Fordyce's spots, lingual papillae, palatal and lingual tori, sublingual varicosities and fissured, coated and geographic tongue. The clinical appearance of these and their management are outlined in Table 1.
Normal anatomical features (or variants) seen in the mouth

Figure 1 shows a deeply fissured tongue, which is best demonstrated by spreading the tongue laterally. Figure 2 shows the characteristic clinical appearance of a geographic tongue.

Deep fissures on tongue. Reproduced from Tyldesley, W.R. Color atlas of oral medicine (2nd edition) (1994). Copyright Elsevier.
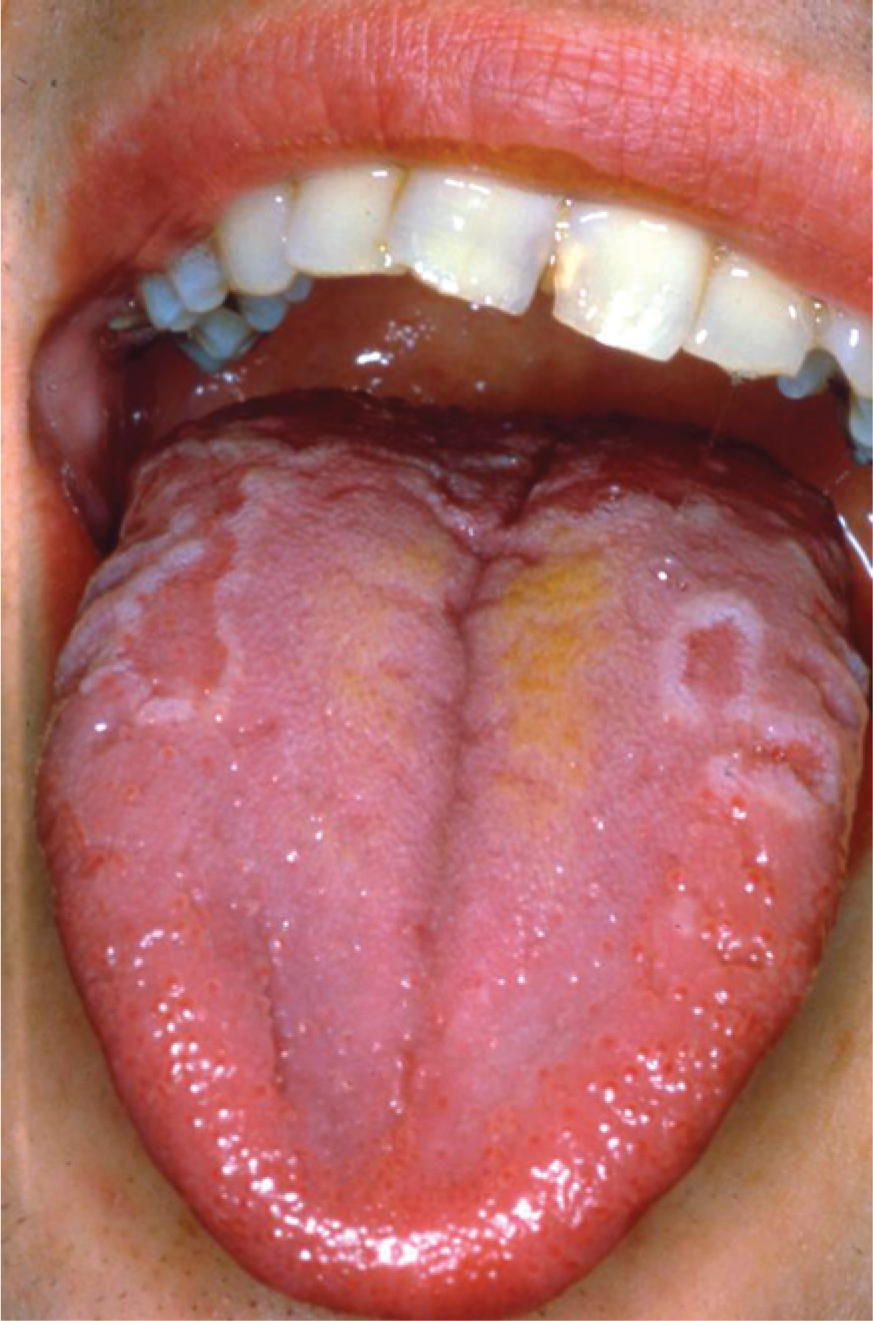
Geographic tongue: a typical clinical appearance. Reproduced from Tyldesley, W.R. Color atlas of oral medicine (2nd edition) (1994). Copyright Elsevier.
Benign oral lesions and conditions
Oral mucosal swellings
The most common causes of benign oral mucosal swellings are cysts arising in the minor salivary glands of the lower lip (mucoceles) and inflammatory overgrowths resulting in fibroepithelial polyps (Fig. 3) or hyperplastic tissue related to ill-fitting dentures. Squamous cell papillomas are relatively common benign neoplasms that occur on the oral mucosa. Viral warts are ‘papilloma-like’ lesions that occur in response to a virus, usually the human papilloma virus (HPV). These can be spread from warts on the hands and fingernails and usually resolve spontaneously. Viral warts are more frequent in immunocompromised patients, including those with human immunodeficiency virus (HIV) infection.

A fibroepithelial polyp on the labial mucosa.
Fibromas and lipomas are relatively uncommon and present as mucosal swellings, which are usually diagnosed histologically following excision. Benign neoplasms of the minor salivary glands (e.g. pleomorphic salivary adenoma) may develop as slow-growing swellings on the palate or in the mucosa of the lip, usually the upper lip.
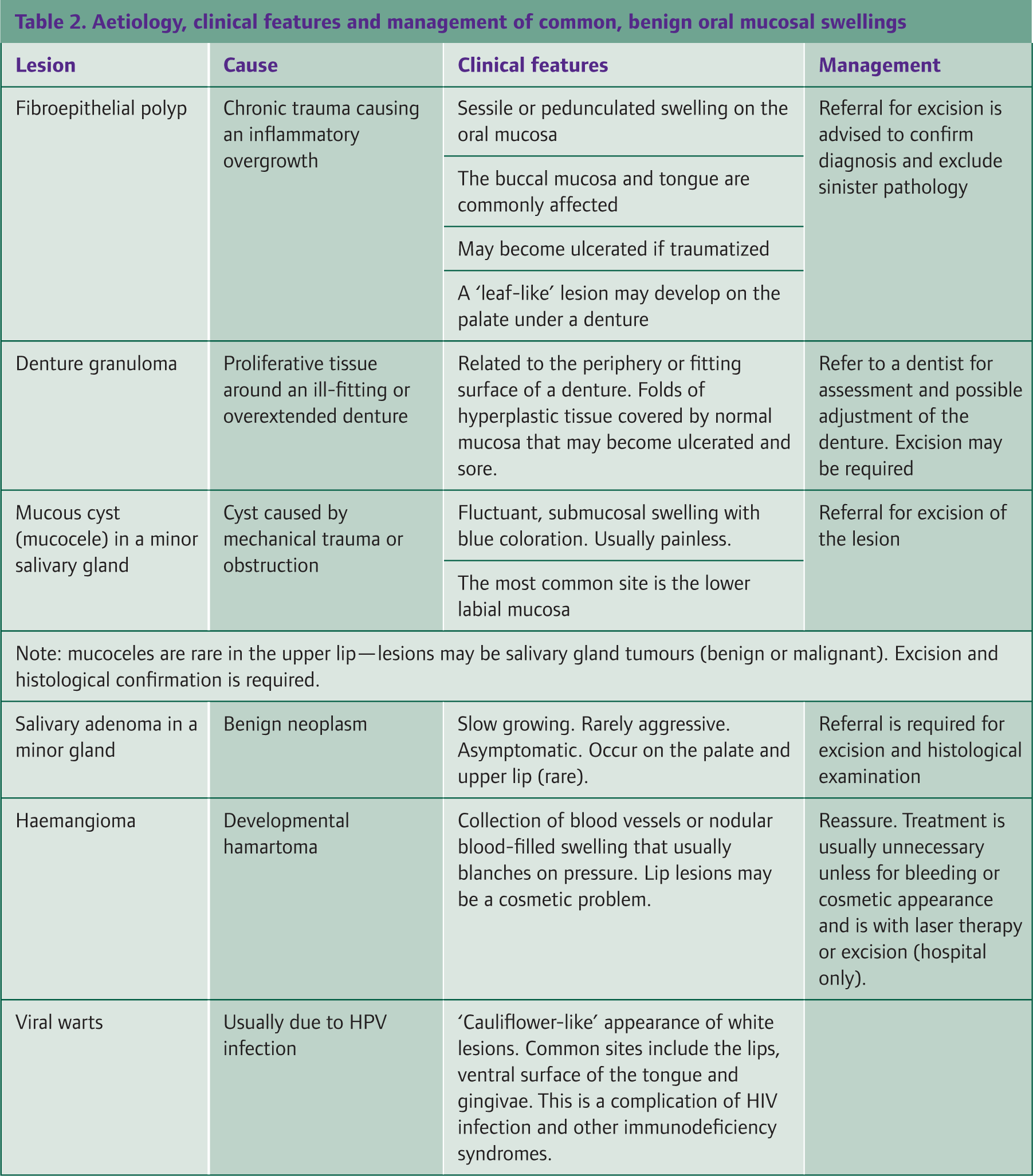
Haemangiomas are relatively common developmental lesions of the oral mucosa and may cause cosmetic problems if affecting the lips. Their appearance can be of a network of red capillaries in the mucosa or a nodular lesion filled with blood, which may blanch on pressure. Haemangiomas may bleed if traumatized but this is uncommon. The clinical features and management of common oral mucosal swellings are shown in Table 2.
Aetiology, clinical features and management of common, benign oral mucosal swellings
Red areas in the mouth
Widespread areas of the oral mucosa with an erythematous appearance may be due to candidal infection or an underlying haematinic deficiency. A raw, ‘beefy’ tongue has long been the classic textbook description of vitamin B12 deficiency, particularly as a result of pernicious anaemia. In clinical practice, patients with glossitis due to a haematinic deficiency (iron, vitamin B12 or folic acid) present with a smooth red appearance on their tongue, due to atrophy of the lingual papillae. The tongue is usually sore and there may be an accompanying candidal infection or angular cheilitis (cracking and erythema at the corners of the mouth). Midline glossitis is an erythematous patch in the midline of the tongue, associated with chronic candidal infection; this may be ‘lozenge’ shaped, hence its alternative name of median rhomboid glossitis (Fig 4).

Medial rhomboid glossitis: erythematous lesion in the middle of the tongue. Reproduced from Tyldesley, W.R. Color atlas of oral medicine (2nd edition) (1994). Copyright Elsevier.
Loosely adherent white plaques on an erythematous oral mucosa, which rub off with scraping, are highly suggestive of pseudomembranous candidiasis, which can be acute or chronic. This type of candidal infection may occur in neonates but in adults it is often due to local factors such as oral dryness, the use of inhaled corticosteroids, an underlying systemic disease including immunosuppression (e.g. HIV infection) and iron deficiency. Patients taking systemic corticosteroids or wide-spectrum antibiotics are also susceptible to pseudomembranous candidiasis.
Patients who wear dentures, either partial or complete, may have an erythematous palate underneath the fitting surface of the denture, particularly if this is worn throughout the night. This is the most common form of oral candidal infection and is painless. Patients need to leave their dentures out at night and clean them thoroughly; antifungal treatment is rarely needed unless there is an accompanying angular cheilitis.
Atrophic lichen planus may present as multiple or single areas of erythema on the oral mucosa but these are often interdispersed with reticular, white or ulcerative lesions, typical of oral lichen planus. Blood-filled oral blisters due to a platelet deficiency or an immunobullous condition such as oral pemphigus or pemphigoid may appear on the oral mucosa. There is also a condition known as angina bullosa haemorrhagica, in which idiopathic blood blisters appear.
Patients who have a low salivary flow (e.g. due to Sjögren's syndrome or xerogenic medication) and those with a radiation-induced mucositis following treatment for cancer may present with an erythematous oral mucosa. This is usually sore and may cause difficulty with eating and drinking.
Localized and persistent red lesions in the mouth should be regarded as suspicious as they may be due to erythroplakia, which may prove to be cancerous (see Suspicious Oral Lesions—this journal). The main causes of localized and generalized red areas in the mouth are shown in Box 1.
Dark pigmented areas in the mouth
Widespread brown pigmentation is usually racial in origin and due to melanin but may be caused by drugs such as minocycline. Addison's disease should also be considered, particularly if the patient has any other clinical features to suggest this. A number of rare conditions, such as Peutz—Jeghers syndrome, have oral manifestations and present with widespread oral (and perioral) melanotic pigmentation; the nails can also be affected by pigmentation.
Red areas in the mouth: main causes

Suspicious oral lesion
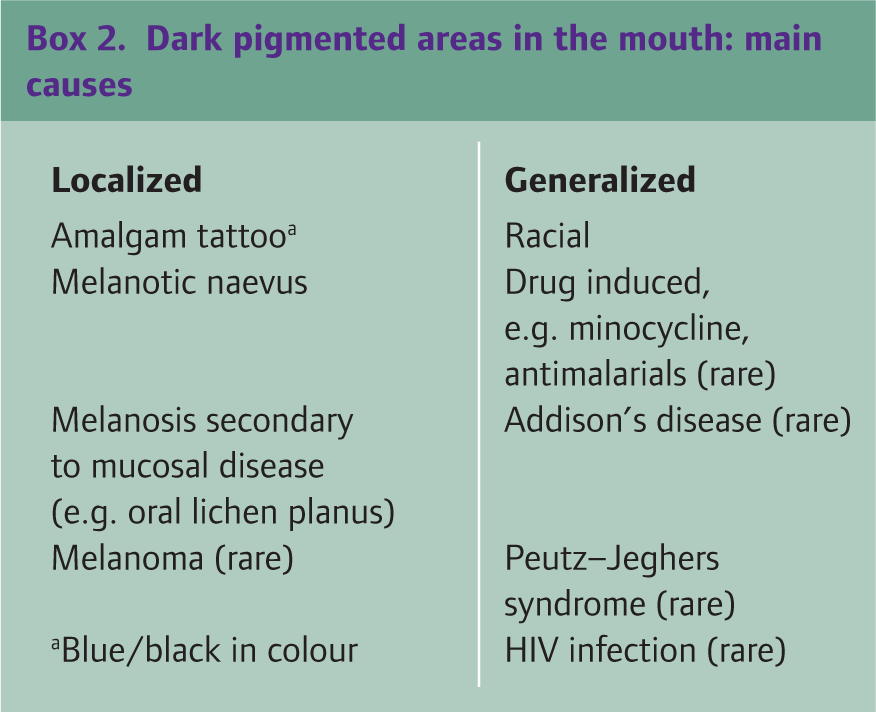
The most common causes of solitary areas of dark pigmentation in the mouth are amalgam tattoos and pigmented oral naevi; these both are benign lesions. Malignant melanomas and Kaposi's sarcomas are rare but should be included in the differential diagnosis (see Suspicious Oral Lesions—this journal). The localized and generalized causes of dark, pigmented oral patches are summarized in Box 2.
Dark pigmented areas in the mouth: main causes
Blue/black in colour
Oral dysaesthesia and burning mouth syndrome
Oral dysaesthesia is a term used to denote disturbances of oral sensation and includes conditions such as burning mouth syndrome (BMS) and complaints about an altered taste or a dry mouth (xerostomia), where there are no clinical signs or a discernible cause.
Patients with BMS complain of a generalized oral soreness of burning sensation, which typically affects the tongue, although other parts of the mouth can also be involved. On examination, there is no recognizable abnormality and the oral mucosa appears normal. It is important to exclude any underlying systemic condition in these patients; as in the early stages of a haematinic deficiency or undiagnosed diabetes, there may be a complaint of a burning or sore mouth that appears normal. Oral candidiasis or a dry mouth are other possible causes and should be investigated. If the patient wears a denture (full or part), then these should be checked by a dentist, in case these are ill-fitting and causing trauma. Patients with BMS may attribute this to an allergy to their denture material but this is extremely uncommon; it is much more likely that they are intolerant to dentures, however well constructed. If no identifiable condition is found for the patient's ‘burning’ mouth, there may be an underlying psychogenic cause, such as chronic anxiety and depression, which need to be addressed and appropriately managed. Some patients with BMS have friends or relatives who have suffered from mouth cancer and they have developed a cancer phobia. The management of BMS is summarized in Box 3.
Management of BMS
Eliminate: Systemic disease Local causes (e.g. candidiasis) Counselling Cognitive behavioural therapy (refer to a clinical psychologist) Antidepressant therapy
Management in general practice
Reassurance for patients with normal anatomical structures or recognizable developmental lesions in the mouth is usually sufficient. Candidal infections should be appropriately managed with topical and/or systemic antifungal agents and the underlying cause identified or investigated. Patients with persistent soreness and erythema of the oral mucosa should undergo investigations for haematinic deficiencies and to check for undiagnosed diabetes.
Referral
Dentists have considerable training in diagnosing oral lesions and conditions; their opinion can therefore be sought in the first instance, provided this does not delay the referral of a suspicious oral lesion to secondary care. Swellings associated with teeth or gingivae may be due to dental infection (e.g. abscess) or associated cysts and the patient should be referred to their dentist. All persistent swellings on the oral mucosa should be referred for specialist assessment as biopsy is usually required to check that there is no histopathological evidence of a malignant neoplasm. Referral to a specialist in oral medicine or oral and maxillofacial surgery is also advisable if there is evidence of an oral mucosal condition (e.g. oral lichen planus) or if oral symptoms persist and there is no identifiable cause. Suspicious oral lesions should be referred on an urgent basis (see Suspicious Oral Lesions—this journal).
Key points
Some patients are concerned about the appearance of structures within their mouth that are normal or variants of normal Swellings on the oral mucosa should be referred to an oral specialist for assessment, including biopsy. The majority of oral mucosal lesions are benign Patients who present with a generalized sore mouth may have a candidal infection and/or underlying haematinic deficiency Patients with BMS complain of a sore or ‘burning’ sensation but the oral mucosa appears normal.