
Abstract
Dizziness is a common complaint in general practice and is used by patients to describe many different sensations. The key to making the diagnosis is to qualify exactly what the patient means by ‘dizzy’ in order to establish whether this represents true vertigo. This article aims to provide an overview of common causes of vertigo encountered in general practice.
The GP curriculum and vertigo
Vertigo and specifically Ménière's disease feature as common and/or important conditions in the knowledge base of
Vertigo/dizziness (neurological, otological, psychological and cardiovascular causes) also features as a common or important symptom in the knowledge base of
Does the patient have vertigo?
Definition
Vertigo is an illusion of movement of the patient or his surroundings. It is most often a spinning sensation, but it may also be a side-to-side, to-and-fro or up-and-down sensation. Associated symptoms may include unsteadiness, nausea, vomiting, pallor or sweating.
Which dizzy patients do not have vertigo?
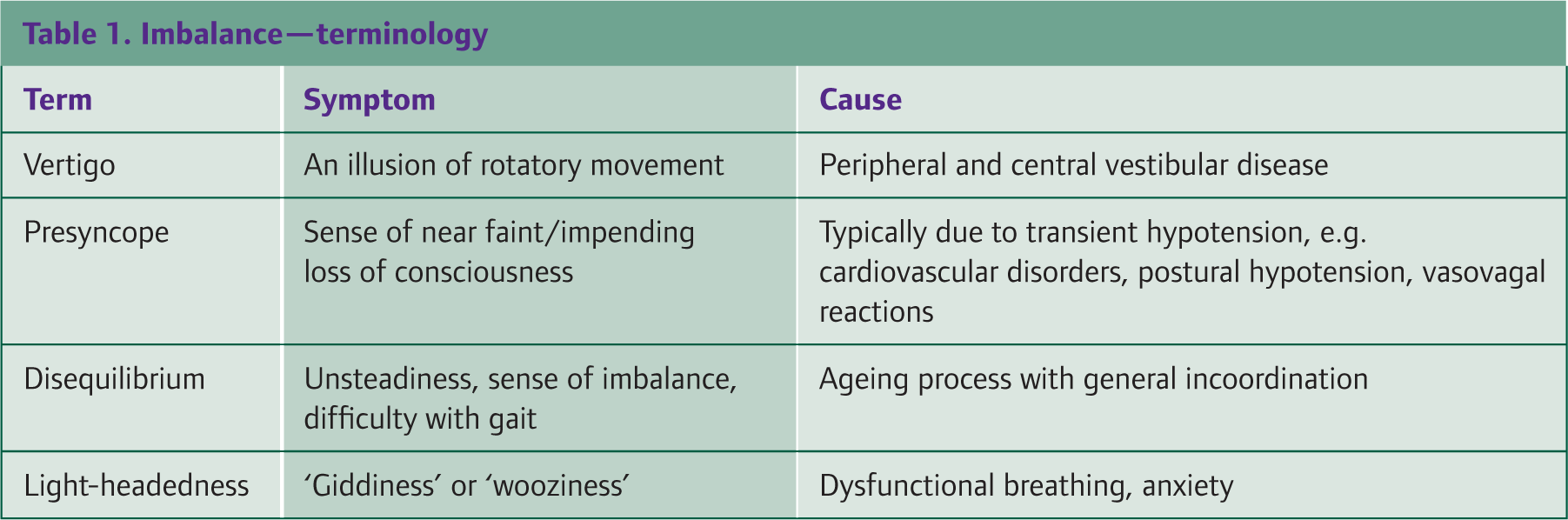
Light-headedness, disequilibrium and presyncope may be described as dizziness by patients (see Table 1). In all these, there is no illusion of movement or typical associated symptoms. These patients do not have vertigo.
Imbalance—terminology
Causes of vertigo
The causes of vertigo are summarized in Box 1. Vertigo may be classified as:
peripheral—resulting from a disorder of the inner ear or eighth cranial nerve or central—resulting from a disorder of the central nervous system
The duration of the episodes (Box 2) and the presence or absence of auditory symptoms help to make a diagnosis. Deafness or tinnitus associated with vertigo indicates that its origin is probably from the ear or the eighth cranial nerve. Features that would increase the suspicion of a central cause include prolonged or severe vertigo, new-onset headache, focal neurological signs or symptoms, central-type nystagmus (e.g. vertical nystagmus) or prolonged and severe imbalance.
Assessment
History
The history is the most important part of the consultation when assessing a patient with vertigo. Patients may find their symptoms hard to describe and will often use ambiguous terms such as ‘dizziness’, ‘feeling drunk’, ‘wooziness’ or ‘unsteadiness’ to describe their symptoms; the precise meaning of their words must be clarified. People with vertigo usually describe a sensation of the outside world moving relative to themselves, often with rotatory or spinning symptoms. A question such as ‘Did you just feel light headed or did you see the world spin around as though you had just got off a playground roundabout?’ may be useful to clarify what patients mean once a history has been given in the patient's own words. Once you have established that the patient has vertigo (and not pre-syncope, disequilibrium or light-headedness), try to determine the cause of the vertigo. Salient points in the history are summarized in Box 3.
Causes of vertigo
Benign paroxysmal positional vertigo (BPPV)
Acute labyrinthitis/vestibular neuronitis
Ménière's disease
Ototoxicity (e.g. secondary to aminoglycosides)
Middle ear disease, e.g. cholesteotoma, acute otitis media
Herpes zoster oticus (Ramsay Hunt syndrome)
Brainstem and cerebellum, e.g. multiple sclerosis, stroke or transient ischaemic attack
Cerebral pontine angle, e.g. acoustic neuroma (rarely—usually presents with hearing loss)
Cerebral cortex, e.g. vertiginous epilepsy (vertigo as the aura of a temporal lobe seizure)
Migraine-related balance disorders
Psychological—anxiety, mood, somatization or personality disorders
Cervical spondylosis (vertebro-basilar insufficiency)
Drugs
Alcohol
Duration of symptoms
Episodic vertigo lasting seconds to minutes: BPPV Episodic vertigo lasting minutes to hours: Ménière's disease Prolonged vertigo (greater than 24 hours): peripheral lesion (e.g. viral labyrinthitis) or central lesion (usually associated with other signs, e.g. migraine, multiple sclerosis, stroke, tumour).
If peripheral vertigo is suspected, use the history and examination finding to differentiate between conditions. There are two main deterministic factors that separate BPPV and vestibulitis attacks from those of Ménière's disease. These are as follows:
Questions to ask to help identify the cause of vertigo
Timing of symptoms—duration, onset, frequency, severity Aggravating factors (such as movement of the head) Effect on daily activities (such as walking)
Otological—such as hearing loss, ear discharge, a feeling of fullness in the ear or tinnitus (unilateral or bilateral) Neurological—such as headache, diplopia, visual disturbance, dysarthria or dysphagia, paraesthesia, muscle weakness or ataxia General autonomic symptoms—nausea and vomiting, sweating or palpitations
Recent upper respiratory tract infection or ear infection—suggestive of vestibular neuronitis or labyrinthitis Migraine—increases the likelihood of the vertigo being migrainous Head trauma or recent labyrinthitis—suggests BPPV Direct trauma to the ear—consider perilymph fistula Anxiety or depression—can exacerbate dizziness or vertigo. Rarely, anxiety or depression may manifest as dizziness or vertigo, especially if the person hyperventilates. Cardiovascular risk factors (such as previous angina or myocardial infarction, diabetes, hypertension, smoking or atrial fbrillation)—increase the likelihood of stroke as the cause of vertigo Drugs, e.g. aminoglycosides, furosemide, antidepressants, antipsychotics, anticonvulsants (carbamazepine and phenytoin)—may cause vertigo Acute intoxication with alcohol—may cause vertigo O Family history of migraine or Ménière's disease—may increase the likelihood of these conditions
the duration of attacks—episodic vertigo lasting a few seconds or minutes is commonly due to benign positional vertigo; episodic vertigo lasting minutes to hours, consider Ménière's disease; prolonged vertigo (in excess of 24 hours), consider a peripheral lesion, e.g. viral labyrinthitis or trauma, or a central lesion (usually associated with other signs), e.g. multiple sclerosis, stroke or tumour the presence of associated auditory symptoms, e.g. tinnitus, a sensation of aural fullness and hearing loss—in BPPV, there are no associated auditory symptoms; Ménière's disease is associated with hearing loss, aural fullness and tinnitus; hearing loss is a feature of labyrinthitis, and tinnitus can be a feature; in vestibular neuronitis there are no associated auditory symptoms.
Examination
The examination will to some extent be determined by the history. Box 4 summarizes the main points of examination that should be covered in a patient presenting with vertigo.
Examination
Test cranial nerves and cerebellar function Examine the eyes for nystagmus: note its direction and whether it is affected by changing the direction of gaze or fixing the eyes on an object. Suppression of nystagmus with visual fixation suggests a peripheral cause. Pure vertical nystagmus suggests a central cause. Examine gait and ability to stand unaided
Check for postural hypotension if suggested by history Check for arrhythmias and carotid bruits in the elderly
Romberg's test—to identify instability of either peripheral or central cause (although it is not a sensitive test for differentiating between them). Ask the patient to stand still with feet together. If able to do that ask the patient to close his eyes and see what happens—Romberg's sign is positive if the patient loses balance with his/her eyes closed. Unterberger's test—to identify damage to one of the labyrinths. Patients are asked to walk on the spot with their eyes closed. If the patient rotates to one side, there is a labyrinthine lesion on that side. Dix—Hallpike manoeuvre (Figure 2)—to help make a diagnosis of BPPV Head thrust test — ask the patient to fix his/her eyes on your nose. Place your hands on the patient's head and rapidly turn it 10–15 degrees to one side. If the vestibular apparatus is working correctly, the patient will be able to maintain focus on your nose. If there is a problem with the vestibular apparatus (e.g. labyrinthitis or vestibular neuritis), the patient's eyes will deviate to the side and then jerk back to look at your nose (a positive head thrust test).
Investigations
If there is associated hearing loss, an audiogram should be obtained. This helps in the diagnosis of Ménière's disease. However, direct access audiology is often not available for patients with vertigo associated with deafness, and an ENT referral may be necessary.
Otological and peripheral causes
For the purpose of this article, we are focusing on common otological causes of vertigo encountered in general practice and referred to ENT or audio-vestibular medicine clinics.
The balance organs
Each inner ear consists of a labyrinth (balance organ) and cochlea (organ of hearing)—see (Fig. 1).
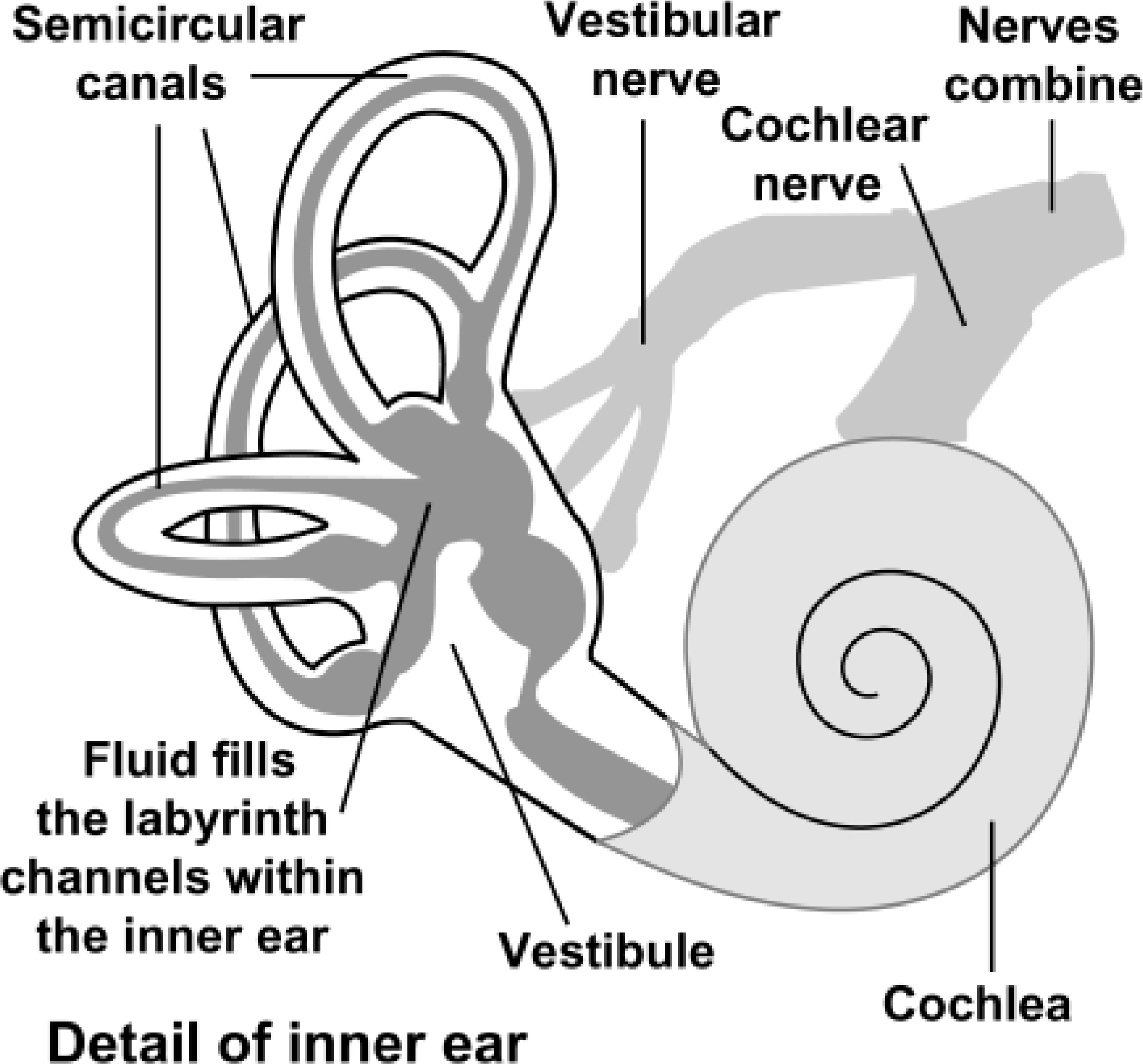
Inner ear structure.
Benign paroxysmal positional vertigo
BPPV is the most common cause of peripheral vertigo, affecting between 11 and 64 people/100 000/year. Women are affected almost twice as often as men with a peak incidence at 50–70 years of age. It is believed to be caused by otoconia, which are normally fixed firmly on the otolithic membrane. One theory is that they become loose and float into the semicircular canals causing movement of the fluid of the inner ear after certain head movements. Accordingly, head trauma is a common cause for BPPV, although most cases are idiopathic. BPPV may also follow vestibular neuronitis.
Patients experience brief (from seconds to a minute at most) episodes of rotatory vertigo precipitated by head movements. They have no vertigo in between attacks but may feel nauseated. The most common precipitating movement is rolling over in bed or on tilting the head to upwards. The condition causes no tinnitus or hearing loss.
Diagnosis of BPPV can be confirmed using the Dix—Hallpike manoeuvre (Fig. 2). This is a simple positioning test that reproduces vertiginous symptoms and provides the examiner with objective findings. The test is positive if vertigo and nystagmus are induced. The nystagmus occurs after a latent period of 2–6 seconds and is typically torsional (rotatory) and fatiguable.

Dix-Hallpike manoeuvre. Dix-Hallpike manoeuvre (used to diagnose BPPV). This test consists of a series of two manoeuvres: with the patient sitting on the examination couch, facing forward, eyes open, the examiner turns the patient's head 45 degrees to the right. The examiner supports the patient's head as the patient lies back quickly from a sitting to supine position, ending with the head hanging 20 degrees off the end of the examination table. The patient remains in this position for 30 seconds. Then the patient returns to the upright position and is observed for 30 seconds. Next, the manoeuvre is repeated with the patient's head turned to the left. The test is positive if any of these manoeuvres produce vertigo with or without nystagmus.
Usually, BPPV is self-limiting lasting a few weeks, although it may continue intermittently for years. Reassure the patient. Labyrinthine sedatives are not helpful. Teach the patient to minimize symptoms by sitting and lying in stages. Habituation may occur by maintaining the trigger position until the vertigo settles.
If symptoms are not settling and are distressing the patient, refer to ENT for an Epley's manoeuvre (or perform an Epley manoeuvre in the GP surgery if you have the appropriate training) and/or refer to physiotherapy for balance retraining exercises.
The Epley manoeuvre (Fig. 3) aims to remove otoconia from the semicircular canals and repositions them into the utricle, where hair cells are not stimulated. It is effective for symptoms relief in the short term for up to 90% of patients. A repeat treatment can be performed after 1 week if there is no improvement. The Epley manoeuvre involves a series of four movements of the head and body from sitting to lying, rolling over and back to sitting. After the procedure, patients should be advised not to lie flat for 48 hours, to avoid aggravating movements and not to lie on the affected side for 1 week.
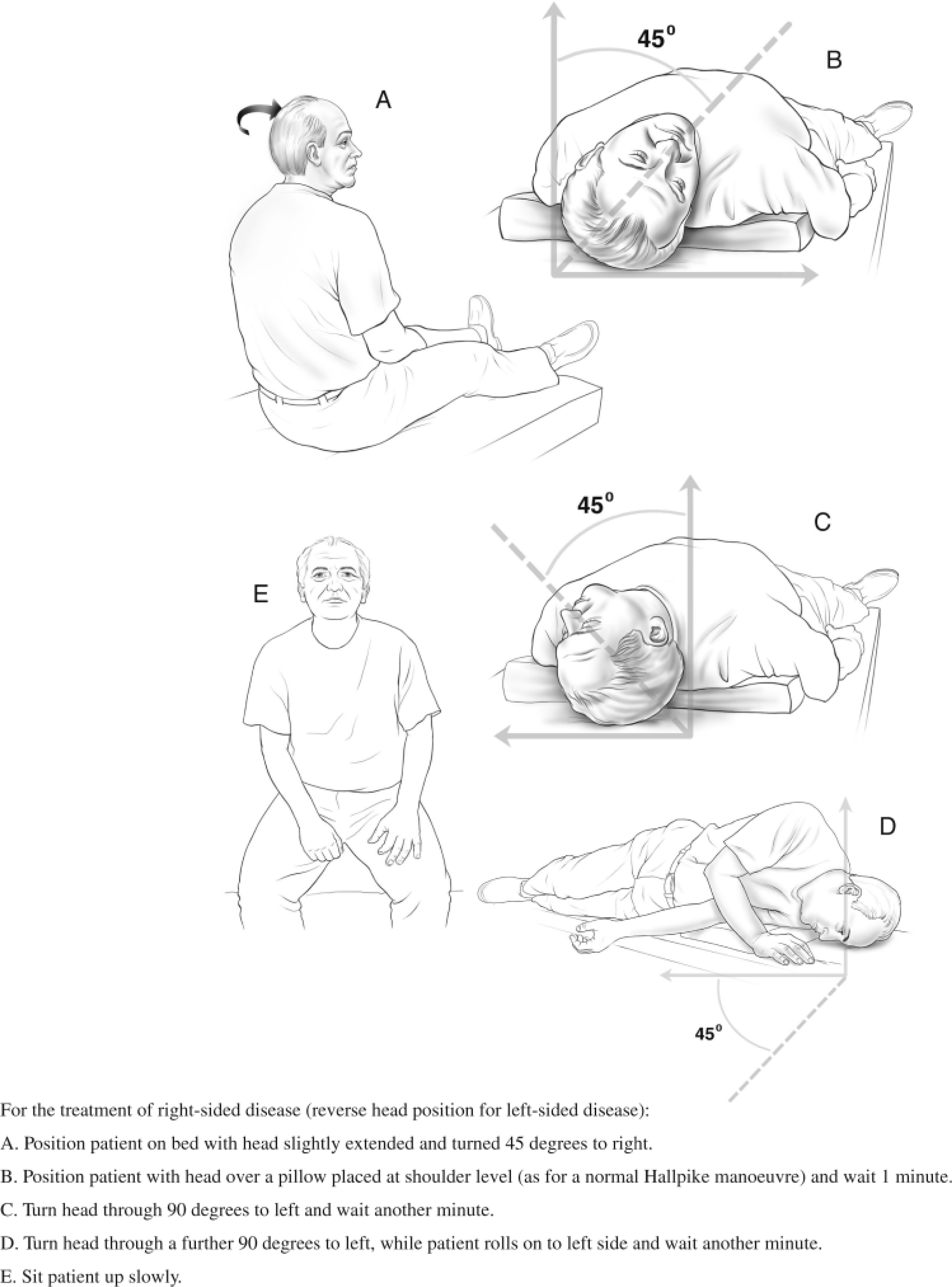
Epley manoeuvre.
Review all patients 6 weeks after the Epley manoeuvre. If dizziness continues at that time, an ENT referral is advisable to exclude other causes of dizziness. There are surgical treatments for BPPV but these are rarely used.
Ménière's disease
Ménière's disease is over-diagnosed. It occurs in approximately 50 people/100 000, usually affecting young to middle-aged adults. Ménière's disease is characterized by recurrent acute episodes of vertigo, tinnitus, hearing loss and a sense of pressure in the ear (aural fullness). Symptoms usually start in one ear, but 30–50% people have bilateral symptoms within 3 years of presentation. Ménière's disease is associated with endolymphatic hydrops (raised endolymph pressure in the membranous labyrinth of the inner ear). The cause is unknown but suggested factors include allergy, autoimmunity, genetic susceptibility, metabolic disturbances involving the balance of sodium and potassium in the fluid of the inner ear and viral infection.
Acute attacks typically last more than 20 minutes and most commonly 2–4 hours. Vertigo is associated with nausea, vomiting and autonomic effects. Nystagmus is always present during an attack and is usually mixed horizontal-torsional (rotatory). The patient may experience disequilibrium after an attack for several days.
Attacks tend to occur in clusters with quiescent periods in between. A fluctuating low-frequency sensorineural hearing loss is found in the early stages of the disease, later becoming permanent and the vertigo ‘burns out’. To confirm the diagnosis of Ménière's disease, refer the patient to an ENT consultant or a consultant in audio-vestibular medicine/neuro-otologist. The management of Ménière's disease is summarized in Box 5.
Vestibular neuronitis and labyrinthitis
The terms vestibular neuronitis and labyrinthitis have been used interchangeably in the past but specific terminology is now recommended. Vestibular neuronitis (more common) is thought to be due to inflammation of the vestibular nerve and labyrinthitis involves more widespread inflammation of the labyrinth and the vestibular nerve. Both typically affect previously well, young or middle-aged adults and commonly occur following a viral upper respiratory tract infection. Both present with sudden onset of severe vertigo that may be accompanied by nausea and vomiting. Hearing loss is a feature of labyrinthitis, but hearing is not affected in vestibular neuronitis. Nystagmus is usually present, which is unidirectional (fast phase away from the affected side) and horizontal.
Severe vertigo subsides after 1–2 days due to vestibular compensation, but unsteadiness may last for 2–3 months. Treatment is symptomatic with labyrinthine sedatives, e.g. cyclizine or prochlorperazine. These can be taken regularly for 3 days, then only on an as-required basis. They should be taken for the minimum time possible and not for longer than 1 week in total, as they may delay recovery by affecting the body's compensatory mechanisms. Prolonged courses sedating the vestibular organs result in an iatrogenic state of unsteadiness and episodic vertigo.
Patients with symptoms persisting for more than 6 weeks should be referred for ENT review. Vestibular rehabilitation may help once other causes of vertigo have been excluded.
Middle ear disease
Acute otitis media can produce a spectrum of symptoms of imbalance ranging from mild unsteadiness to disabling vertigo. Vertigo settles with resolution of the acute infection, so treatment is mainly symptomatic.
Chronic suppurative otitis media may be a sign of underlying errosive cholesteatoma. This can errode the bony covering of the labyrinth to produce a fistula connecting the middle and inner ear. This is uncommon in the developed world and a detailed history should arouse suspicion of this diagnosis. If cholesteatoma is suspected, urgent referral to ENT is indicated.
Treatment of Ménière's disease
Treat acute attacks with labyrinthine sedatives, e.g. cyclizine (50 mg three times daily) or prochlorperazine (5 mg up to six times daily). Consider buccal or rectal routes of administration if the patient is vomiting. Do not use labyrinthine sedatives long term. Encourage patients to mobilize after an acute attack
smoking cessation cutting out caffeine and alcohol and a low salt diet.
Provide information and advice about support organizations Vestibular rehabilitation, tinnitus maskers and/or hearing aids may be helpful There is some indication that stress may precipitate attacks. Look out for and treat concurrent anxiety and depression and consider relaxation tapes or referral for relaxation techniques
Vertebro-basilar insufficiency
With increasing age, the cervical spine becomes progressively arthritic, with osteophyte formation. On extension and rotation of the neck, these osteophytes can constrict the vertebral artery, causing fleeting imbalance as a result of cerebral ischaemia. Other significant neurology may occur: dysphagia, dysarthria, transient focal motor or sensory deficit, blurring of vision (secondary to diplopia) and drop attacks. The patient may have associated cervical spondylosis and neck pain.
If the cause of the patient's symptoms is uncertain, refer to secondary care for confirmation of the diagnosis. Treatment is usually with lifestyle advice (avoidance of the movements that provoke the symptoms). Neck physiotherapy may help in a few cases. Some consultants advocate the use of a cervical collar to support the neck and prevent provoking movements but this is controversial.
Vestibular rehabilitation
Vestibular rehabilitation therapy (VRT) is an exercise-based programme designed to promote central nervous system compensation for inner ear deficits. VRT can help with a variety of vestibular problems, including BPPV and unilateral or bilateral vestibular hypofunction associated with Ménière's disease, labyrinthitis and vestibular neuritis.
Specialist therapists are usually accessed via ENT and/or physiotherapy departments. Although exercises should ideally be tailored to the individual, access to specialist help can be difficult to obtain and there is often a significant delay. A widely used intervention for patients with vestibular problems are the Cawthorne-Cooksey exercises. These are home-based exercises that can be undertaken by the patient (if tolerated) while awaiting review by a specialist therapist. A modified version of these exercises is included in Box 6.
Central causes
Migraine is the most common cause of central vertigo. The vertigo may not follow the normal time course of other migrainous ‘auras’; it may occur before, during or after the characteristic headache and vomiting. The symptoms may last from seconds up to 72 hours rather than the usual 5–60 minutes of a typical migrainous aura. A careful history should reveal such information as a personal or family history of migraine, trigger foods and associated aura features. Pure tone audiograms fail to demonstrate a sensory neural hearing loss.
Patients with new onset headache and clear vertigo need admission to hospital, unless there is a history of recurrent similar episodes. Brainstem vascular events can present in a similar way to migrainous vertigo; therefore, vestibular migraine is a diagnosis of exclusion.
Uncommon causes of central vertigo are stroke and transient ischaemic attack, cerebellar tumour, acoustic neuroma and multiple sclerosis. In these cases, there are normally associated ‘red flag’ symptoms (Box 7).
Psychogenic vertigo
Anxiety can be a cause of vertigo, but this is a diagnosis that should only be made once other organic causes have been excluded. Frequency and duration of symptoms are good discriminators when diagnosing the cause of vertigo. Suspicion should be aroused if the history sounds atypical, for example, if the patient consistently complains of dizziness of significant variability in duration.
Episodes often continue for several years, and presentations can alter over this time. During an attack, patients can become extremely distressed and disorientated, and as a result, they may have difficulty recalling events precisely. One should go on to ascertain whether head movement has any bearing on symptoms; organic vestibular causes are usually intensified by head movement, whereas non-organic causes are not normally. Ataxia is usually a prominent feature during a true peripherally mediated attack and absent in psychogenic causes.
Some advocate supervised hyperventilation in the consultation as a way of replicating dizziness related to anxiety. With the cessation of hyperventilation and of vertiginous symptoms, a link is made on which to build patients' awareness of their ability to help themselves. Treatment is then arranged to address underlying anxiety disorders. However, there is rarely time to do this in a standard 10 minute GP consultation.
Self-help balance exercises for patients with vestibular causes of vertigo
Sit on the edge of the bed Turn your head to one side and rapidly lie down on the same side After the vertigo subsides, return to the upright position Repeat turning your head to the other side Repeat once more on each side
Week 1: In bed
Perform the following eye movements—at first slow and then quick:
Gazing up and down Gazing from side to side Focusing on one finger moving from 30 to 10 cm away from your face
Week 2: Sitting
Head and eye movements as for week 1 Shoulder shrugging and circling Bending forwards and picking up objects from the ground
Week 3: Standing
Head and eye movements, shoulder shrugging and circling as for week 2 Change from sitting to standing position with eyes open and closed Throw a ball from hand to hand under one knee Change from sitting to standing position, turning around in between
Week 4: Moving about
Head and eye movements, shoulder shrugging and circling as for week 2 Walk across the room with eyes open then closed Walk up and down a slope with eyes open then closed Pick a ball up from the floor, hold it up as high as you can stretch and throw it at a target
If any of these exercises cause excessive discomfort, stop and go back a stage for another week.
‘Red flags’ for urgent referral in a patient with acute vertigo
Any central neurological symptoms or signs New type of headache (especially occipital) Acute deafness Vertical nystagmus
Urgent referral to secondary care
The NHS Clinical Knowledge Summary on vertigo (2010) suggests the following admission and urgent referral criteria for patients with acute vertigo:
Admit to hospital if the person has severe nausea and vomiting and is unable to tolerate oral fluids Admit or urgently refer to a neurologist if the person has very sudden onset of vertigo (within seconds) that persists or acute vertigo associated with neurological symptoms or signs such as new type of headache (especially occipital), gait disturbance, truncal ataxia, numbness, dysarthria, or weakness, which may suggest stroke, transient ischaemic attack or multiple sclerosis Admit or refer as an emergency to an ENT specialist or audio-vestibular physician if the person has acute deafness without other typical features of Ménière's disease (tinnitus and a sensation of fullness in the ear)—sudden-onset unilateral deafness suggests acute ischaemia of the labyrinth or brainstem (but can also occur with infection or inflammation). Emergency treatment may restore hearing. The person should be seen within 12 hours of the onset of symptoms.
Practical aspects
Vertigo is a very distressing condition that often has a huge impact on the patient's life. In elderly people, it can cause loss of confidence and limit their ability to get out and about and even to self-care. It may be a cause of falls too. For younger people, vertigo may prevent work. Use of the new Med3 to specify amended duties is very relevant here for people in occupations requiring bending, work at heights etc. For all these reasons, vertigo increases the likelihood of anxiety and depression. For people with chronic vertigo, the Ménière's Disease Society (website: www.menieres.co.uk; telephone: 0845 120 2975) can be a source of help and support. Lucy Yardley's book on the effects of vertigo (available free to download from the Ménière's Disease Society website) is very helpful in this respect.
Vertigo and driving
Advise patients not to drive when they are dizzy or if they are likely to experience an attack of vertigo while driving. Inform drivers liable to ‘sudden attacks of unprovoked or unprecipitated disabling giddiness’ that they are responsible for informing the Driver and Vehicle Licensing Agency (DVLA) of their condition. For people with an ordinary licence, driving must cease on diagnosis and will be permitted when satisfactory control of symptoms is achieved. The driving licence will be restored until a person is 70 years of age if he or she remains symptom free. For people with a vocational licence, the licence will be refused or revoked if the condition is sudden and disabling. The underlying diagnosis should be considered and if it is likely to cause recurrent attacks, a person must be symptom free and controlled for at least 1 year before reapplication.
Key points
A structured and detailed history is key to diagnosing the cause of dizziness - patients often complain of dizziness but mean something else Once it is determined that a patient has vertigo, the next task is to assess whether the patient has a peripheral or central cause of vertigo The duration and frequency of episodes, and the presence of associated auditory symptoms are helpful in determining the diagnosis Most cases of true vertigo result from BPPV, acute labyrinthitis or Ménière's disease All patients with vertigo should have an otoscopic examination to exclude middle ear pathology Prolonged use of vestibular sedatives may cause imbalance due to labyrinthine suppression: these drugs should be used for a few days at most.
Footnotes
Acknowledgement
With thanks to Dr S.S. Surenthiran, FRCP, FRCS, MSc, DIC Consultant, Neuro-otologist, Balance & Hearing Centre, Fitzroy Square and Blackheath Hospitals London, Medway Maritime Hospital Kent, for his expert review of this article.