
Abstract
Elbow pain is a common complaint that affects a significant proportion of the population and accounts for a high number of consultations within general practice. The cause of elbow pain in some patients may be obvious and localized such as in the case of olecranon bursitis, but in others, this may be presentation of an occult multisystem disorder. We have tried to provide both a comprehensive review of the possible causes of elbow pain as well as useful methods of history taking and examination to help differentiate between causes. Most causes of elbow pain may be effectively treated in General Practice and we have included an update on the practical techniques for injections around the joint.
The GP curriculum and elbow pain
The GP curriculum provides guidance in
Demonstrate complete examination of the elbow Understand the principles of treatment for common conditions managed largely in primary care including the use and monitoring of non-steroidal anti-inflammatory drugs (NSAIDs) and disease-modifying drugs Show knowledge of when joint injections and aspirations are appropriate in general practice and the ability to perform when appropriate, e.g. shoulder and knee joints and injections for tennis and golfer's elbow Understand the roles of allied health professionals (nursing, physiotherapy, occupational therapy, counselling and psychological services) Chronic disease management including systems of care, multidisciplinary teamwork and shared-care arrangements Understand referrals requiring emergency action to save life or prevent serious long-term sequelae Advise regarding appropriate levels of exercise Undertake health promotion regarding accident prevention Demonstrate empathy and compassion towards patients with incurable, disabling or painful musculoskeletal conditions Provide adequate information for informed consent before any procedure is undertaken. Describe the key national guidelines that influence healthcare provision for musculoskeletal problems [e.g. the National Institute for Health and Clinical Excellence (NICE) guidelines, Royal College of General Practitioners (RCGP) low back pain guidelines, Scottish Intercollegiate Guidelines Network (SIGN) guidelines, etc.].
Anatomy
The elbow joint is a complex joint consisting of three articulations. These are the radio-humeral joint, the ulnohumeral joint and the proximal radio-ulnar joint. These allow extension and flexion as well as pronation and supination of the forearm. The function of the elbow is to allow positioning of the hand in space. The functional range is from 30° to 130° of flexion, allowing it to reach the mouth and to allow for perineal hygiene.
Another important function is to allow transmission of force from the hand to the body. Elbow movement is restricted in several planes to allow for greater stability. There is both a radial and an ulnar collateral ligament (UCL) that contribute to stability although in full extension the bony articulation confers the majority of this stability. A number of important structures cross the elbow. The ulnar nerve passes behind the medial epicondyle and is palpable in this position. The median nerve is found medial to the brachial pulse, which in turn is medial to the biceps insertion in the antecubital fossa. Laterally, the radial nerve crosses in front of the elbow as it divides into branches supplying the extensors of the wrist and digits. These structures are at risk with any injury to the elbow and make surgery on this area treacherous. Figure 1 demonstrates important landmarks on the lateral side of the elbow.
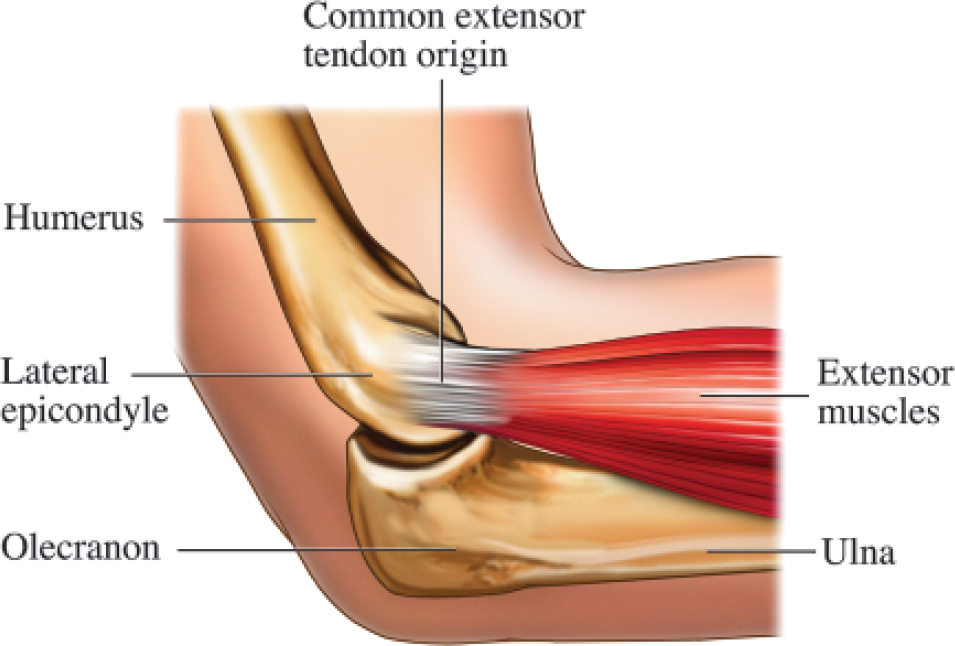
Bony structures of the lateral elbow with illustration of the common extensor origin at the lateral epicondyle. Nucleus Medical Art, Visuals Unlimited/SPL.
History and examination
While there are a number of pathologies that affect the elbow specifically, the clinician must be aware of the possibility of elbow pain presenting as a manifestation of a multisystem disease such as rheumatoid arthritis. Similarly, elbow pain may result from derangement of a different system such as in the case of haemarthrosis in haemophilia. Hence, a thorough general history and examination is essential. This is also important to exclude any emergencies presenting with a painful elbow (see Box 1).
Emergencies
Patients with a history of trauma with elbow pain and bony tenderness or neurological compromise should be sent for urgent radiographs to exclude fracture Any patient with a hot swollen joint who has systemic features of sepsis should be referred to the emergency department for assessment
Specific points to include in the history would be any evidence of fever or malaise as well as any trauma or pain in other joints. Particular note should be made of symptoms suggesting rheumatoid arthritis or gout.
Questions should focus on the speed of onset of the pain and whether it is predominantly medial, lateral or posterior. Careful details of occupation and leisure activities are essential to delineate overuse injuries, which are among the most common causes of pain. Occasionally, there may be a history of locking or snapping that could be caused by a loose body or mobile ulnar nerve. The essential components of the examination of a painful elbow are described in Box 2.
Tennis elbow
Descriptions of lateral epicondylitis have been available since at least 1880 when it was described as lawn tennis elbow. Unfortunately, the term tennis elbow has been used to describe other conditions affecting various areas of the elbow and forearm leading to some confusion as to the nature of the disease. The term epicondylitis is also considered a misnomer as no inflammatory cells are found during histological examination. For the purposes of this article, we will use the term tennis elbow to refer solely to lateral epicondylitis.
Tennis elbow is a well localized pain over the lateral epicondyle that affects around 1 in 10 patients at some point. Those at greatest risk are men between the ages of 30 and 55 years. Although the condition may be brought on by a sudden episode, there is usually a history of chronic repetitive overuse. This may eponymously arise from tennis or be occupational, for example, in mechanics using spanners. The pain often worsens during periods of activity and abates at night. Symptoms are usually well localized to the lateral epicondyle and poorly localized pains in the proximal forearm may be due to other pathologies such as the radial tunnel syndrome where the radial nerve is entrapped between the two heads of the supinator muscle.
Pain results from microtrauma and inadequate repair to the common extensor origin at the lateral epicondyle. This predominantly affects the origin of the extensor carpi radialis brevis (ECRB). The signs of tennis elbow are elicited by stressing the ECRB origin with resisted active extension of the wrist or passive flexion of the wrist with the forearm pronated and the elbow extended. Tenderness is usually found just distal and anterior to the epicondyle. Careful examination may reveal localized swelling and pain that worsens on gripping an object.
Management of tennis elbow
The mainstay of treatment is simple analgesics, NSAIDs and rest from the causative activity. Rest may, however, be difficult or impossible where there is an occupational cause, especially in a self-employed patient. Sometimes adjusting the grip size of a tool that is implicated in causing the problem may alleviate the pain and such patients should be encouraged to experiment with larger and smaller grips.
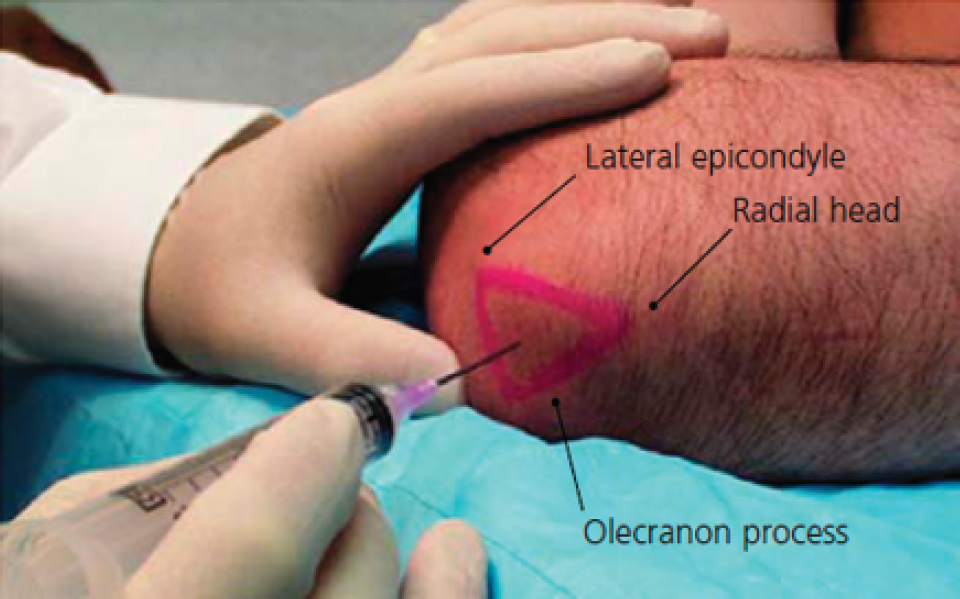
Various other management options are available for tennis elbow. These include steroid injection (see Box 3 and Fig 2), splinting and physical therapy. A recent Cochrane review compared methods of splinting but found no demonstrable benefit. Steroid injection appears to have an excellent early rate of success (92% at 6 weeks in one study) but after 12 months of treatment, patients appear to gain better results from physical therapy. Regardless of the modality of treatment, most patients are pain free by 1 year.

Technique for injection of lateral epicondylitis.
A number of treatments are available for refractory tennis elbow, including surgical procedures and extracorporeal shock wave therapy (ECSWT). Recent NICE guidance on ECSWT (NICE, 2009) suggests that there is likely to be no harm from the technique but that there is inconsistent evidence for its efficacy and NICE recommends its use only in specialized centres. Surgery may be effective in up to 85% of patients and those who have had symptoms for several months despite local anaesthetic and steroid injections, rest and bracing should be referred for surgical opinion.
Examination
Clinical examination should include thorough general examination as well as assessment of the wrist, shoulder and cervical spine. Elbow examination should follow the Look-Feel-Move principle as follows:
The patient should be seated facing the examiner with both arms and ideally the trunk exposed.
Observe the symmetry of the elbow joints. Is there any erythema or swelling over the joint? Look for evidence of elbow effusion, this is apparent from ‘filling-in’ of first the hollows around the olecranon and later the hollows around the radial head Lumps around the elbow may include rheumatoid nodules and gouty tophi that may give clues to the diagnosis. It is also worth inspecting the hands for Heberden's nodes and other changes of osteoarthritis. Look for swelling over the olecranon suggestive of bursitis With the patient's arms fully extended look for a difference in the carrying angle (angle between the long axis of the forearm and that of the humerus). This may indicate new pathology or be residual from an old injury such as a childhood supracondylar fracture.
Compare warmth of the joint with the other side Palpate for tenderness over the medial and lateral epicondyles as well as over the olecranon Palpate the ulnar nerve behind the medial epicondyle. This may feel thickened or be hypermobile Palpate for tenderness over the triceps tendon and to look for tendinopathy or rupture. Attempt to hook the distal biceps tendon from the lateral side with a finger to identify a ruptured tendon. With the elbow flexed palpate the epicondyles and the tip of the olecranon. These should lie in an equilateral triangle. This arrangement is disrupted in elbow dislocations.
Ask the patient to fully extend each elbow. Full extension usually places the elbow in line with the humerus at zero degrees although a few degrees of hyperextension is normal in female patients. Next, ask the patient to flex the elbow as far as possible and to touch both shoulders with their hands. Look for any difference in range of movement. Ask the patient to fix their elbows by their sides to exclude shoulder movement and then to pronate and supinate their hands. The range of movement here may be better appreciated by asking the patient to grip a pencil in each hand while this is done. Finally, flex the elbow to 30° and apply valgus (directing the forearm laterally and the arm medially) then varus (directing the forearm medially and the arm laterally) stresses to look for joint instability.
In those with lateral elbow pain, ask the patient to fully extend their elbow then to extend the wrist against resistance. This causes pain in those with lateral epicondylitis.
For medial elbow pain, Tinel's sign may be assessed. This is where tapping over the ulnar nerve causes pain or paraesthesiae in the hand and indicates irritation of the nerve. Although most commonly used for the median nerve to assess carpal tunnel syndrome, this test is useful in other sites. Evidence of medial epicondylitis should be assessed by asking the patient to pronate the forearm and flex the wrist against resistance. Both signs may coexist in a patient with medial epicondylitis.
Golfers' elbow
Golfers' elbow is a similar overuse injury to tennis elbow but affecting the medial epicondyle. Epicondylitis occurs at a ratio of around 10 lateral cases for every one medial case. The predisposing factors include throwing sports and cricket. Damage to the common flexor origin at the medial epicondyle usually affects the pronator teres and flexor carpi radialis muscles. Histologically, these tend to show a similar pattern of degeneration with partial or complete tendon rupture occasionally a feature. Tenderness is usually found just distal to the medial epicondyle. Examination of the ulnar nerve and the medial collateral ligament is important to exclude ligamentous instability or neurapraxia.
X-rays are useful in excluding some other pathologies although there may be little or no abnormality seen in epicondylitis with the exception of occasional calcification seen within the tendon. Ultrasound scan will show tendinopathy confirming the diagnosis if necessary.
Management of golfers' elbow
Management of golfers' elbow is similar to that of tennis elbow with the mainstay of treatment being activity modification, analgesia, physical therapy and injection. Surgery is reserved for recalcitrant cases. The indications for referral are similar to those for tennis elbow. Patients receiving injections for medial epicondylitis should be warned of the risk of ulnar nerve damage and of paraesthesiae in the ring and little fingers of the hand on the injected side.
Injection technique for medial or lateral epicondylitis
The steroid and anaesthetic used may vary between practices although one suggested regimen is 2–3 ml 0.5% bupivacaine with 1 ml of methylprednisolone (40 mg/ml). For lateral epicondylitis, the elbow should be flexed to 45° and the wrist pronated. Palpation identifies the point of maximum tenderness and the needle (25 g; Orange) is inserted perpendicular to the skin. Once bone is felt on the tip of the needle, it should be pulled back 1–2 mm to avoid injection below the periosteum and around 1 ml of the solution injected slowly. For injecting the medial side, the arm should be abducted with the elbow extended and the hand supinated. Relief should be fairly rapid following injection depending on the type of local anaesthetic used.
Figure 2 illustrates the technique for injection of lateral epicondylitis.
UCL injury
The UCL is the primary stabilizer of the elbow when held in flexion. This may commonly be damaged as a result of severe valgus stress on the forearm, for example, by trauma. However, both a chronic strain and a rupture are possible in patients performing a repetitive throwing action. Professional athletes are able to generate huge forces that stress this ligament, although in some patients even relatively infrequent throwing exercise may cause damage. This occurs during the acceleration phase of throwing, which accelerates the arm ahead of the forearm in a whipping action. The medial (ulnar) side of the joint is distracted, stressing the UCL.
Examination of the elbow reveals medial tenderness that is sometimes accompanied by eccymoses. There may be opening up of the joint space medially or pain on varus and valgus stressing and comparison with the contralateral elbow is advised. X-rays are useful to exclude a fracture, especially in young children where the medial epicondyle may be avulsed in preference to ligamentous rupture.
Management of UCL injury
Management is usually conservative and is commenced with resting of the joint for 3–6 weeks along with symptomatic control using NSAIDs, paracetamol and the RICE protocol (
Ulnar nerve entrapment
Ulnar neuropathy may result from direct trauma, repetitive elbow flexion or arthritis in the elbow as a consequence of osteophyte formation. Nearly 20% of patients have a hypermobile ulnar nerve that can ‘snap’ across the medial epicondyle causing pain, or the condition may develop as a late complication of a supracondylar fracture in patients with an abnormal carrying angle.
Symptoms are occasionally of an intense burning pain on the postero-medial surface of the elbow or forearm but usually the more pronounced features are paraesthesiae in the ring and little fingers as well as weakness or clumsiness of hand movements. Tinel's sign at the elbow is usually positive. While the site of the nerve lesion is usually in the cubital tunnel at the elbow, the nerve is also very superficial at the wrist and may be damaged by repetitive trauma here, the so-called cyclists' palsy. One final consideration is that the lesion may be more proximal and caused by spinal pathology or a thoracic outlet syndrome. Here, careful examination followed by special investigations such as nerve conduction studies or magnetic resonance imaging hold the key to accurate diagnosis.
Management of ulnar nerve entrapment
Initial management consists of analgesia and protecting the elbow from further damage by avoidance of provoking factors. Some patients may find night-time splinting effective. Patients with persistent symptoms and all those with muscle wasting in the hypothenar eminence or well established numbness in the little finger and half of the ring finger should be referred promptly for decompression. Where the nerve is hypermobile, it may be surgically transposed anteriorly and reattached to prevent it snapping over the medial epicondyle and causing further damage.
Olecranon bursitis
This is a common cause of pain and swelling around the elbow. There are in fact two bursae at the olecranon: one superficial bursa, which is most commonly affected, and one deeper bursa between the triceps tendon and the joint capsule. This disorder, known as students' or miners' elbow usually results from trauma to the point of the elbow. This may be very minor and be unnoticed by the patient. Bleeding into the bursal sac causes permanent damage to the epithelial lining that pre disposes recurrent attacks and patients should be warned of this at an early stage. Occasionally, the bursitis may be caused by another disorder such as rheumatoid arthritis or gout.
Examination will reveal a swelling over the olecranon that may be fluctuant. While bursitis is the most common diagnosis here, the examiner should be alert to rarer possibilities such as soft tissue tumours that may occur in this region.
Broadly, there are two presentations of bursitis, septic and non-septic. Classically, the non-septic bursa is painless and not erythematous. These do not need to be routinely aspirated. Septic bursitis may present with mild symptoms such as pain and swelling although if there is marked cellulitis, pyrexia or systemic evidence of sepsis, then the patient should be referred to the local emergency department for assessment. Occasionally, if there is a pointing abscess, or in the case of systemic sepsis, the bursa may be washed out. However, this is generally avoided wherever possible because of the risk of forming a chronic bursal sinus. Aspiration of septic bursae is also controversial although if an attempt to aspirate the bursa is made, then it should be aspirated to dryness.
Staphylococcus aureus is the organism responsible for 90% of septic bursitis, and the majority of the remaining 10% are caused by beta-haemolytic streptococci. These are commonly treated with flucloxacillin or erythromycin that have both been shown to penetrate the bursa well and should be continued for at least 10 days. Both types of bursitis may be helped by NSAIDs, compression and protective elbow dressings. Following commencement of therapy, the discomfort from septic bursitis tends to resolve more quickly while non-septic bursitis may take several weeks to resolve.
Arthritis of the elbow
All the polyarthritides may affect the elbow although it is not a commonly involved joint in any. Only 1–2% of osteoarthritic joints are elbows. These tend to occur in patients who place high demands on their elbows such as labourers and there is a strong male preponderance. Osteoarthritis may be primary or may follow injury to the elbow such as radial head fractures that can cause a secondary osteoarthritis. Osteophyte formation may restrict range of movement at the elbow and those osteophytes that break off can form loose bodies within the joint. These cause pain and intermittent clicking or locking of the joint. Pain may be elicited at the elbow by axial loading combined with gentle supination and pronation. This can be helpful in differentiating arthritis from other conditions such as epicondylitis in which this will not cause pain.
Management of arthritis of the elbow
Osteoarthritis of the elbow may be managed along similar lines to arthritis in other joints with holistic assessment of the patient, self-management strategies such as weight loss and symptom-relieving therapies such as exercise. This may be supplemented by simple analgesics and NSAIDs and physiotherapy with intra-articular steroid injection as an adjunct to treatment.
Only 5% of patients with rheumatoid arthritis will have elbow involvement although these patients do present significant challenges as nearly 90% will have involvement of the shoulder, wrist or contralateral elbow. Hence, while disease control via systemic agents such as steroids and disease-modifying agents must be optimal, consideration of surgery must be made in the context of other affected joints. A further challenge in the rheumatoid patient is the risk of cervical spine involvement. This group of patients presenting with elbow pain should therefore have a careful neurological assessment of the upper limb.
Injection of the elbow may be an effective treatment in arthritis. This is most safely achieved using a lateral approach. The patient's elbow should be flexed to 45° and sterile technique used throughout. Identify the triangle formed by the radial head, lateral epicondyle and the tip of the olecranon. A needle introduced perpendicular to this triangle will reach the joint space for the introduction of a steroid/local anaesthetic mixture (e.g. 1–2 ml methylprednisolone 40 mg/ml with 3–5 ml 0.5% bupivacaine). This technique is illustrated in Fig 3.
Technique for injection or aspiration of the elbow joint.
Surgical options for the management of elbow arthritis range from arthroscopic debridement for mild disease through to total elbow replacement for severe disease. The surgical option must, however, be appropriate to the demands that will be placed on the elbow; debridement could shorten the career of a sportsman while total elbow replacement would be doomed to failure in a self-employed labourer.
Tendinitis
Tendinitis usually affects the large muscles acting on the elbow, the biceps and the triceps. The cause is unclear but may be microtrauma or degeneration of the tendon. The patient may complain of exquisite pain on moving the elbow and there may be tenderness over the triceps tendon posteriorly or the distal biceps tendon in the antecubital fossa. Palpation of the long head of biceps in the deltopectoral groove may also reveal tenderness. Treatment is with analgesics, NSAIDs and the RICE protocol.
Tendon rupture
Rupture of the biceps usually follows a sudden forceful contraction although may also be as a result of chronic inflammation. Patients may complain of the sudden onset of pain during heavy lifting and on examination there will be weakness of flexion and particularly supination. The hook test may be used to assess congruency of the distal tendon. Here, the examiner approaches the antecubital fossa from the lateral side and uses a finger to ‘hook’ under the biceps tendon. In a complete rupture, there is no structure for the finger to hook under. This test has higher sensitivity for distal biceps rupture than either ultrasound scan or magnetic resonance imaging.
Less commonly, the triceps tendon attachment may rupture either partially or completely. This may be accompanied by a small bony avulsion from the olecranon and so X-rays may be helpful in deciding management. Clinically, patients with a complete triceps rupture will not be able to extend their elbow against gravity and tendon will be impalpable on resisted elbow extension.
Partial ruptures of both biceps and triceps may be treated conservatively but complete ruptures are usually treated surgically within a few days of the injury. Some patients who place low demands on elbow flexion opt for conservative management of distal biceps ruptures although these patients must be warned of the resulting weakness, particularly of supination. Where there is suspicion of partial or complete rupture of the biceps or triceps tendon, then urgent referral is recommended.
Tendon ruptures are more common in patients who have a predisposing cause, such as those who abuse anabolic steroids. Careful enquiry on this subject may be helpful in starting discussion on steroid abuse, preventing other side effects and helping to safeguard the long-term health of the patient.
Elbow injuries in children
The pattern of injuries in children varies slightly from that of adults. A fall on the outstretched hand may cause a supracondylar fracture of the humerus. This requires recognition and urgent referral to accident and emergency for radiographs.
In children under the age of 5 years, one common presentation is a pulled elbow. This condition results from a subluxation of the radial head within the annular ligament that surrounds it. There may be a history of mild trauma or a fall although commonly the cause is unclear and the child presents with reluctance to use the affected arm. The arm is classically held with the elbow part-flexed in mid-pronation.
Where there is no other strongly suspected diagnosis, it is reasonable to attempt reduction of these injuries without radiology. Reduction is performed by gentle supination of the forearm with the elbow at 90° flexion and a thumb over the radial head. There is often a palpable click as the radial head relocates.
The child should return to normal play over a few hours and should be reviewed 2 days later to ensure symptoms have resolved. Where there is the suspicion of a more serious injury, the child should be referred for radiographs at the local accident and emergency department.
Finally, it is important to reassure parents that this injury will not affect long-term elbow function and that it may recur in either arm. By the age of 5 years, the annular ligament stiffens sufficiently to prevent subluxation and further episodes.
Many children are involved in throwing sports at school and some, encouraged by parents, coaches and their peers, place great demands on their elbows. During the throwing action, there is, as previously discussed, a large valgus strain placed on the elbow. This causes distraction of the medial joint space, compression of the lateral joint and shearing forces in the posterior compartment around the olecranon tip.
Compression of the radio-capitellar joint may damage the blood supply to the capitellum, over time causing shearing of the cartilage off an area of bone. This is called an osteochondral defect. The capitellum is well supplied with blood up to around the age of 5 years but after this age it is only supplied by one or two vessels that run through the relatively soft cartilage. If not properly rehabilitated, over time a full osteochondral defect may develop causing a bony island and a loose body within the joint. The child may present with medial elbow pain from the ligament sprain or lateral pain from the chondral defect. Examination can reveal reduced extension in the affected arm. Anteroposterior, lateral and oblique radiographs may show irregular ossification around the capitellum, a subchondral crater or loose bodies within the joint.
As with other overuse injuries, the treatment is by activity modification, RICE protocol and splinting. Once pain has subsided, then range of movement exercises may be commenced. There may need to be some attention to throwing technique and indeed frank discussions with parents about the need for activity modification and reduction in the intensity of practice. Only once the child has regained a full pain-free range of movement, should they be allowed to make a graduated return to throwing activities. Those patients who develop clicking or locking from a loose body within the joint may require arthroscopic removal and large osteochondral defects can be treated surgically with drilling or grafting of the osteochondral lesion.
Similar throwing forces may affect the medial elbow at the apophysis of the medial epicondyle. This can cause pain, fragmentation of the apophysis and occasionally avulsion of the epicondyle. This may be demonstrated on plain X-rays. Medial epicondyle avulsions require surgical fixation but most medial epicondyle apophysitis is treated conservatively with rest and analgesics.
Key points
The function of the elbow is to position the hand in space and it therefore has to be considered in the context of shoulder, wrist and hand function All patients with hot swollen joints with any evidence of systemic sepsis should be referred to the emergency department for urgent assessment All patients with bony tenderness and a history of trauma should similarly be referred for urgent radiographs to exclude a fracture Epicondylitis is likely to resolve within a year and physical therapy is as effective as injection for treatment by this time. Surgery is reserved for refractory cases. Recurrence of all overuse injuries may be most effectively prevented by removing the damaging stimulus or improving technique