
Abstract
If you find yourself in a position where you have to give feedback to a colleague, this can often be a daunting prospect. This article will give you some practical tips and guidance, along with relevant theory, so that you can approach such a task with confidence. Primary care is a multidisciplinary speciality in which there is often little hierarchy. This means that you could find yourself getting feedback to a colleague from a different background to yourself or find yourself giving feedback to someone whom you see as a senior clinician.
The GP curriculum and giving effective feedback
Demonstrate the ability to give effective feedback to a colleague
The context
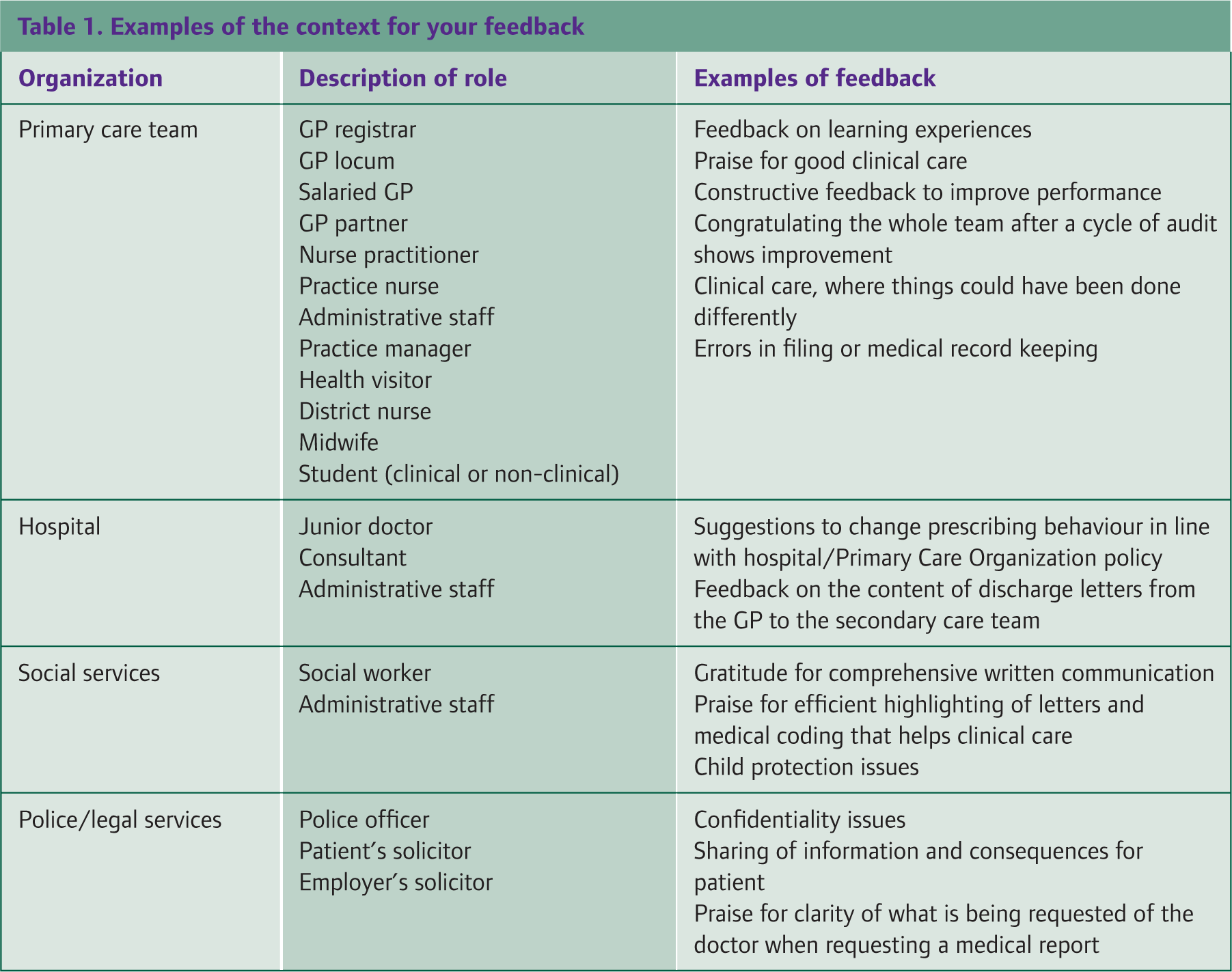
Although GPs normally work in a GP surgery, their situation is unique among all the specialities because their work ties in with many different services. This means that you could find yourself giving feedback either face to face or at a distance (Table 1). One of the reasons we give feedback could be when someone is unhappy, when there has been a complaint or when we have noticed that something could be done differently. However, feedback is not always negative and positive feedback to compliment someone who has done well is equally important.
Examples of the context for your feedback
Individual feedback
The most usual scenario for giving feedback to a colleague will be to an individual with whom you work or supervise. This is usually a one-to-one event. As doctors, we have often had a history of both giving and receiving feedback like this. Medical students start clinical experience in a practical way and rely on other more senior colleagues telling them what they are doing well and what they can change in their practice. Unfortunately, this is not always done as a structured process, so the feedback becomes ineffective.
Before giving any feedback, it is important that you spend some time reflecting on the reasons for giving feedback. For example, feedback might fall into the following categories:
‘corrective’ feedback because something has not gone to plan
positive or congratulatory feedback, which may serve as a morale booster
uninvited feedback, which may cause you the most anxiety and the recipient some concern
requested feedback, where you and the recipient are aware that feedback will be required (for example, in a teaching scenario)
Ideally, you should involve the recipient in the preparation for receipt of feedback. A common way to do this is to set ground rules. In a teaching scenario this can be easy because part of the icebreaker work at the beginning can be to set ground rules. In practice, this may not be possible. Be wary of colleagues who say ‘Just cut to the point’ because this might turn out to be a mistake that affects your working relationships detrimentally. One way to avoid this is to be more recipient centred. Some phrases that may come in handy are as follows:
How do you normally like to receive feedback?
Would you like some feedback?
I usually ask … so you might like to try to do things differently and see if it helps you
The barriers to giving good feedback are similar to the barriers to effective communication generally. Your prior relationship with the colleague and any ‘history’ you share together will undoubtedly influence your feelings and the behaviour of your colleague. If you get on well and already have a good rapport, then the feedback is more likely to be taken positively. If you have no relationship, then it will be more important to try to establish a rapport prior to delivery of the feedback. If there are language barriers (e.g. English as a second language), you may choose to use your words carefully and explain any misunderstanding. Cultural barriers may mean that you or your colleague have certain expectations of when ‘criticism’ is appropriate and this may link into age differences, differences in your levels of experience or expertise. The gender of your colleague and the nature of your feedback may alter how you deliver your feedback.
A good framework to use in giving feedback is the Pendleton guidelines, which are described in the book by Pendleton et al. (1984) An adaptation of these is presented here:
Clarify any points of information regarding the situation
Let the recipient of the feedback state their comments on the events first
Present the good things to the recipient first so they feel supported
Make recommendations rather than being critical to the recipient. I usually find that stating what could have been done differently, rather than better, is less judgemental and does not assume only one correct way of doing things.
Giving feedback that is effective, well received and enhances your professional relationships is akin to having good consultation skills with your patients. Done badly, giving feedback in a way that burns your bridges could find you are adversely affecting professional relationships with colleagues you may rely on for help in the future.
There are often scenarios in medicine when it is inappropriate to spend a long time planning and delivering feedback. For example, it is unlikely that a vascular surgeon will stop to discuss the right and wrong way to stop an artery from bleeding in theatre. Emergencies are a good example of when feedback might need to be swift and to the point. If this is the case, it is helpful to have a debrief later when the situation has resolved. This scenario is, however, unusual in primary care.
Multi-source feedback
This process describes feedback that usually comes from a number of other colleagues. Often there will be a standard questionnaire that the doctor or learner asks other colleagues to fill in about him or herself. The questionnaires may be completed anonymously and sent back to the mentor or trainer to collate and give to the learner in a face-to-face meeting (such as an appraisal). This is an involved and more formal process but if around 10 or more responses are received, this can give a good degree of feedback that is helpful to inform a doctor's practice. The process can be time-consuming for all involved and following the guidelines of Pendleton et al. in delivering the final feedback could be useful. If you find yourself giving the final multi-source feedback results, then it is important that you spend time preparing the physical and emotional environments (e.g. ensure you will not be disturbed, ensure confidentiality and set the scene for the meeting at the outset).
Feedback to others outside your immediate practice team
If your feedback is intended for an individual, then the route for communication is more likely to be face to face, telephone or a personal letter. Should you be trying to give feedback to an organization, it is more likely that your feedback will be by letter. At this point it is always worth trying to find the name and job title of the most appropriate person. Some examples of feedback and appropriate options are given in the four scenarios.
Feedback to the Primary Care Organization about a referral pathway
A 32-year-old woman has a body mass index of 34. She has tried many treatments in order to reduce her weight. You would like her to be referred for gastric banding (an operation that is available in a neighbouring Primary Care Organization but not in your own). She comes to see you and is unhappy about the fact that her Primary Care Organization does not fund this operation. You agree to provide feedback to the Primary Care Organization.
One solution to this might be to ask the practice manager for the name of the person responsible for commissioning decisions in your Primary Care Organization. You could then write to this person outlining the gap in provision of service for your patient. It will be important to obtain consent from the patient prior to sharing any patient identifiable information.
Feedback to the hospital trust about the organization of an outpatient clinic
A number of patients have complained to you about the lack of reasonable car parking adjacent to the fracture clinic. This is a clinic that serves patients who are generally on crutches. Over a period of time, you build up a picture that you are not sure the hospital trust is aware of. Therefore, you feel a professional responsibility to feed this back to the trust management.
Once again a solution could be to write to the hospital trust. However, you may choose to start with an informal telephone call to a consultant colleague to see whether anything is being done about this already.
Showing gratitude to the wider health care team for handling a case of terminal illness well
Recently, a 50-year-old man died at home after a short period on a syringe driver with lung cancer. His wife wanted you to know that she was very grateful for the excellent care and interprofessional communication that she witnessed between the district nurses, Macmillan nurses, GPs and palliative care teams during the last few days.
You choose to write a letter to all the professionals involved highlighting this case and present it at a Primary Care Organization-funded learning event to celebrate success.
Feedback to a commissioning group about the lack of service for people with difficult venepuncture
Recently, a private company, including some local GP partners, has provided a local venepuncture service for your patients. A few patients have complained that the phlebotomist has told them to go to the local hospital because they have difficult veins. Previously, when venepuncture was provided at your surgery, the phlebotomist would have called a more experienced health professional to use a butterfly needle to obtain blood. You are unsure whether the owners of the company are aware that this is going on. Equally, you do not want to appear unsupportive to the commissioning body.
Once again, you may choose to address this informally with local GPs who own the company. However, it may also be important to record your feedback in writing so that the feedback can be taken into account as part of their complaints/feedback critical incident review processes.
When feedback goes well
Once you have given your feedback, if things go well, you should feel a sense of reward. Giving feedback to colleagues is similar to learning consultation skills for use with patients. Once you have tried certain phrases that work for you, you will find yourself using them again in the future. Particularly, if an episode of feedback has caused you some anxiety during the preparation phase, and it subsequently goes well, you may end up feeling safer and more secure about giving feedback again in the future.
What to do when feedback goes wrong—an example
A GP was growing progressively frustrated at the long waits that his patients were suffering when he referred them for primary care counselling. Eventually, a patient who repeatedly attended at the surgery expressed his annoyance at the fact that counselling was taking so long to obtain. The patient felt ‘fobbed off’ by the secretarial staff at the primary care counselling service. The cumulative effect of patients complaining about the long waits made the GP sufficiently frustrated to ring the local mental health team and complain about this. The consultant in charge was consulting, so he left a brief message with the secretary saying that the system was inadequate and not serving patients at all. Owing to the way in which the message was relayed to the consultant, she felt hurt and offended. She subsequently wrote a letter to the GP expressing her surprise at the abrupt message that the GP left with the secretary about the poor referral pathways available to patients.
The GP later spoke to this consultant personally and found that the consultant was already aware of the same problems and was working with the Primary Care Organization to try to increase capacity. She was able to express her eagerness to help primary care mental health patients and the GP was able to feel reassured.
This story serves to show that sometimes when GPs or other colleagues are stressed or frustrated with the service, they can end up giving feedback in an inappropriate way. Spending time preparing how to give the feedback and in the correct way can save embarrassment and enhance working relationships later. GPs are an embedded feature of our health service and rely heavily on being part of a multidisciplinary team.
Summary
Take the opportunity to give feedback as often as possible because it will be good practice for a future career of working in a multidisciplinary team where more and more work is being done by telephone, computer referral systems and e-mail. Remember to keep a record in your own learning log or diary so that this can be discussed in appraisal and you are prompted to follow up the results of your feedback, where appropriate. Your feedback may result in a direct change, for example, a change in policy within your own practice or in secondary care. Feedback is an important component of professional honesty. Without the environment and organizational structures for us to give feedback to colleagues as individuals, colleagues within organizations and colleagues as managers/commissioners of services, we are in danger of serving the needs of our patients poorly. Often GPs are the first to notice issues with individual patients' care and in the care of specific groups of patients because of their unique position in the UK health care system. This perspective comes with the responsibility to be able to give honest and effective feedback.
Key points
Spend time reflecting on your context (in what regard are you giving feedback to a colleague)
Where possible, try to ascertain in what format the recipient would like to receive feedback
Consider contacting the colleague by telephone in the first instance
If your feedback is likely to affect health care systems or pathways, consider backing up your feedback in writing
Consider feedback as an ongoing cycle that, if done well, can enhance professional relationships