
Abstract

This competence is about the doctor's awareness of when his/her own performance, conduct or health or that of others might put patients at risk and the action taken to protect patients.
In this article, we complete our overview of the ‘fitness to practise’ performance area of the MRCGP competence framework. The fourth competence progression (Fig. 1) concerns the action taken when performance, health or conduct become issues in patient care.

The fourth competence progression of fitness to practise.
During the training period, educators keep trainees' performance under review and therefore performance issues are noticed. In independent practice, there is a need for us to monitor our own performance and inform colleagues if significant problems arise that they may not be aware of.
Reporting the performance of colleagues raises other issues. We may be reluctant to report concerns for a variety of reasons including fear that we might have got it wrong, that reporting will cause problems for colleagues, adversely affect working relationships, have a negative impact on careers or result in a complaint. The General Medical Council (GMC) reminds us that ‘if you are hesitating about reporting a concern for these reasons, you should bear in mind that your duty to put patients’ interests first and act to protect them must override personal and professional loyalties'.
The types of behaviour that might trigger action include:
Our duty is not to conduct an investigation but to obtain more information on which to base a decision as to whether further investigation is needed. We should then discuss this information with an appropriate colleague.
In practice, this may mean undertaking some simple checks:
What are the facts (rather than the rumour)? This may involve looking at the medical records and possibly talking through relevant cases/issues with doctors involved. How significant (i.e. serious) is the problem? One way to gauge this is to look at the impact on patient care, particularly patient safety. Has patient harm already occurred or is it imminent? Does this appear to be a one-off or is there evidence that there have been a number of other events that suggest a pattern? Is the problem confined to one area of performance, or might there be problems elsewhere? For example, poor interpersonal skills with patients may be mirrored by poor relationships with staff.
The competence is partly about providing emotional support and showing compassion. This may be inferred from team working abilities and from feedback from colleagues.
In addition, we should be capable of helping a colleague to develop a plan of action, provide support with implementing it and provide feedback on the changes that the colleague tries to make.
Assessor's corner: how do we assess whether the doctor is likely to take the appropriate action?
There are three important elements. Firstly, does the doctor understand what action is being expected of him/her? Secondly, how alert is the doctor to the performance, health and conduct of colleagues? For example, does the doctor (either spontaneously or when asked) comment on the part other doctors have played in the patient's management? Can the doctor give constructive feedback on the performance of others?
Thirdly, how appropriate are, or would be, the doctor's actions? For example, where is the doctor's threshold for looking at performance issues in more detail? Do they understand the risks of doing so as well of not doing so? Do they demonstrate the ability to be discreet, impartial and collaborative when discussing this sensitive area? Is their action proportionate to the problem?
The final competence progression (Fig. 2) concerns complaints, what they say or do not say about performance and how the team can learn from them.
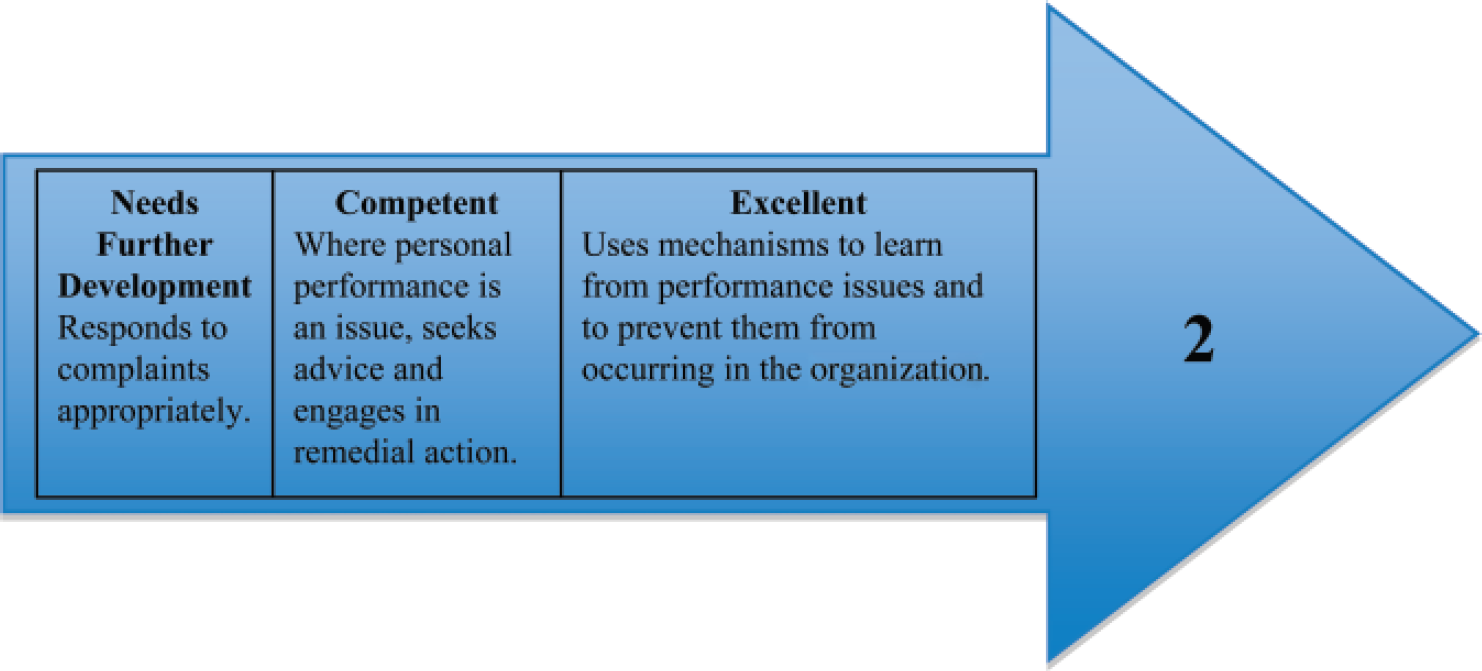
The fifth competence progression of fitness to practise.
Sadly, no matter how well we and our practices function, complaints are inevitable in professional life. Patient education and expectations are increasing and the media widely publicize the (rare) examples of serious issues. These are some of the factors leading to the increase in complaints.
Despite being commonplace, complaints are frequently a source of upset to ourselves as well as those who feel aggrieved. It is best not to take criticism personally as this can adversely affect the response that should be made. For example, we could become defensive or angry, both of which could lead to inappropriate reactions.
Most complaints are dealt with successfully at local level and an appropriate response to a complaint involves a number of steps that you can learn about through discussion with the practice manager.
Assessor's corner: is the doctor responding to complaints appropriately?
Trainees may not receive any complaints during the training period because of limited patient contact and responsibility, close supervision and perhaps a more forgiving attitude form patients towards students. However, trainees could talk about how they would respond should complaints arise. What is the doctor's attitude? Is it appropriately constructive? How would s/he conduct a meeting with the complainant? Role play could help to disclose this and is good practice for the real thing!
Complaints are an important opportunity to look at performance. The pattern of complaints may indicate a specific weakness, for example, in a clinical area. Communication skills are known to be vital in helping to resolve complaints, but poor communication is itself a frequent source of complaints. When complaints occur more frequently than might be expected, this might point to problems with communication but may also be indicative of poor health or poor decision making.
As so often with the descriptors of excellence, the distinguishing feature is that we move beyond our own performance and think about the organization that we are a part of.
Assessor's corner: is the organization learning from performance issues?
Does the trainee note performance issues and bring them for discussion as significant events? Are the lessons that are learned through group discussion then shared with the team? Is there evidence of change in practice behaviour and performance? Does auditing contribute to this process? How much of a part in this process does the trainee play?