
Abstract
Patients frequently present to their GP complaining of soreness or ulceration inside their mouth. Some will have noticed signs such as white or red patches; others will be concerned they may have mouth cancer. The majority of lesions that appear on the oral mucosa are benign; however, oral cancer or potentially malignant lesions may present with a similar clinical appearance and therefore a high level of suspicion is required. Late diagnosis of oral cancer results in a lower survival rate and a compromised functional and cosmetic outcome. Early detection and referral of any suspicious oral lesions are therefore essential to improve the outcome following treatment. This article describes the clinical presentation of malignant and potentially malignant oral lesions and reinforces National Institute for Health and Clinical Excellence (NICE) guidelines concerning specialist referral.
The GP curriculum and oral health
Manage primary contact with patients who have an ear, nose and throat (ENT) or facial problem Be aware of National Institute for Health and Clinical Excellence (NICE) Clinical Guideline concerning referral for suspected head and neck cancer
Oral cancer
Pathology
Squamous cell carcinoma is by far the most common oral malignancy in terms of numbers and worldwide distribution. A wide range of other malignant neoplasms, both primary and secondary, may appear in the mouth but these are relatively uncommon (Box 1).
Malignant neoplasms affecting the oral mucosa
Squamous cell carcinoma (most common) Lymphoma Kaposi's sarcoma Malignant salivary gland tumours Malignant melanoma Malignant neoplasms affecting jaws with spread to oral mucosa (e.g. antral carcinoma, osteosarcoma) Metastatic neoplasms (e.g. lungs, breast, gastrointestinal)
Epidemiology of oral cancer
There were over 5500 new cases of oral cancer (lip, mouth, tongue and oropharynx) diagnosed in the UK in 2004, thus outnumbering cervical cancer. Although this represents only a small percentage (2%) of all UK cancers, the number of new cases is increasing with a trend for a greater proportion of younger people and women being affected. Oral cancer is more common in men than women and the majority of cases in the UK occur in people aged 50 years or over.
The most important aetiological factors for oral cancer are tobacco usage and excessive consumption of alcohol, the two acting separately and synergistically. Other factors linked to increased risk of oral cancer are as follows:
Chewing betel quid (or paan), particularly that containing tobacco. This is common among Asian communities in the UK. A deficient diet—this is of particular relevance in developing countries Immunosuppression, for example, in renal transplant patients and patients with human immunodeficiency virus (HIV) infection Oral lichen planus Exposure to ultraviolet light from solar radiation—this increases the risk of developing cancer of the lower lip
The survival rate for patients with oral cancer depends on the staging of the disease at presentation and the site of the lesion. The prognosis is poor for those with advanced disease, who present at a late stage; those surviving have to cope with the functional and cosmetic consequences of radical treatment. Cancer of the lip has the best outcome with 90% of patients surviving 5 years and most being completely cured. In 2006, there were about 1800 deaths from oral cancer in the UK.
The main forms of curative treatment for oral cancer are surgery and radiotherapy. Patients who have previously been diagnosed with oral cancer are at increased risk of a second primary cancer in the mouth and also elsewhere in the aerodigestive tract.
Other cancers affecting the oral mucosa
Salivary gland carcinomas, affecting the minor glands, may appear as a swelling on the oral mucosa. Some are slow growing, but others can be quite aggressive with rapid growth (e.g. adenoid cystic carcinoma). Malignant tumours of the minor salivary gland predominantly affect the palate and usually present as a swelling that can ulcerate through the mucosa.
Malignant melanomas of the mouth are extremely rare but may occur in a pre-existing area of oral pigmentation. Oral melanomas tend to be fast growing with early metastatic spread and a poor prognosis. Oral lymphomas and Kaposi's sarcoma are uncommon but may occur in immunocompromised patients, particularly those with HIV infection.
Secondary lesions from cancers elsewhere in the body, including the lungs, breast and gastrointestinal tract, are rare; their diagnosis following biopsy of a suspicious oral lesion is usually not predicted. Oral signs and symptoms of acute and chronic leukaemia in their early stages are important to recognize, so that blood tests can be arranged for early diagnosis and prompt treatment.
Suspicious clinical features
Solitary oral ulcer
Oral cancer may present as a persistent oral ulcer with no obvious cause, such as trauma from a tooth or dental restoration. Suspicious features are summarized in Box 2 and include:
a rolled ulcer margin thickening or fixation of the ulcer to the underlying mucosal tissue a proliferative growth adjacent to the ulcer a colour change of the surrounding tissues, i.e. a red, white or speckled appearance
The submental, submandibular and cervical lymph nodes may be involved and have a firm, rubbery or hard texture. Malignant ulcers may be painless, particularly in the early stages. If these develop at the back of the tongue, palate or throat, this may lead to difficulty in swallowing and/or speaking.
Oral carcinoma—suspicious clinical features
Persistent, solitary oral ulcer Rolled margin Fixation to underlying tissue Induration Red, white or speckled oral lesion Oral swelling or proliferative growth Cervical lymphadenopathy Persistent pain—may be referred to ear Difficulty speaking or swallowing Unexplained or sudden mobility of teeth
Although oral cancers can present anywhere in the oral cavity, the posterior and lateral borders of the tongue and the floor of the mouth (known as the ‘coffin’ or ‘graveyard’ area) are suspicious sites and more difficult to examine. Figure 1 shows an early carcinoma on the oral mucosa in the retromolar region of the mouth. Advanced lesions become severely ulcerated, often with swelling of the adjacent mucosa and destruction of adjacent bone (Fig. 2).

Early carcinoma presenting as ulcer in retromolar region of mouth.

Advanced carcinoma of alveolar mucosa with ulceration and bone destruction.
Red, white and speckled lesions
Oral cancer and potentially malignant lesions may present as discrete, fixed white, red or speckled lesions in the mouth. All these clinical appearances should be regarded as suspicious.
A precancerous lesion is defined as a morphologically altered tissue in which cancer is more likely to occur than in its apparently normal counterpart, examples include oral leukoplakia and erythroplakia. The term ‘potentially malignant’ lesion is often preferred because not all precancerous lesions undergo malignant change. Erythroplakia (also known as erythoplasia) and leukoplakia are both potentially malignant oral lesions.
‘Leukoplakia’ is currently defined as a predominantly white lesion of the oral mucosa that cannot be characterized as any other definable lesion. It is a clinical term describing a fixed white patch that may (or may not) have histological features indicative of dysplastic changes or a carcinoma. White patches in the mouth may represent a simple frictional keratosis (e.g. due to cheek biting) or an inherited condition (e.g. white sponge naevus) and have an entirely benign histology. However, all fixed white patches should be regarded with suspicion, until proven otherwise, usually after biopsy. The differential diagnosis of fixed white patches in the mouth is shown in Box 3.
Differential diagnosis of fixed white patches in the mouth
Carcinoma Leukoplakia Frictional keratosis Tobacco-induced keratosis Oral lichen planus Aspirin burn (transient) Discoid lupus erythematosus (rare) White sponge naevus and other inherited conditions (rare)
Leukoplakias on the floor of the mouth (Fig. 3) tend to have a greater potential for malignant transformation than in other sites, particularly if associated with areas of erythroplakia.
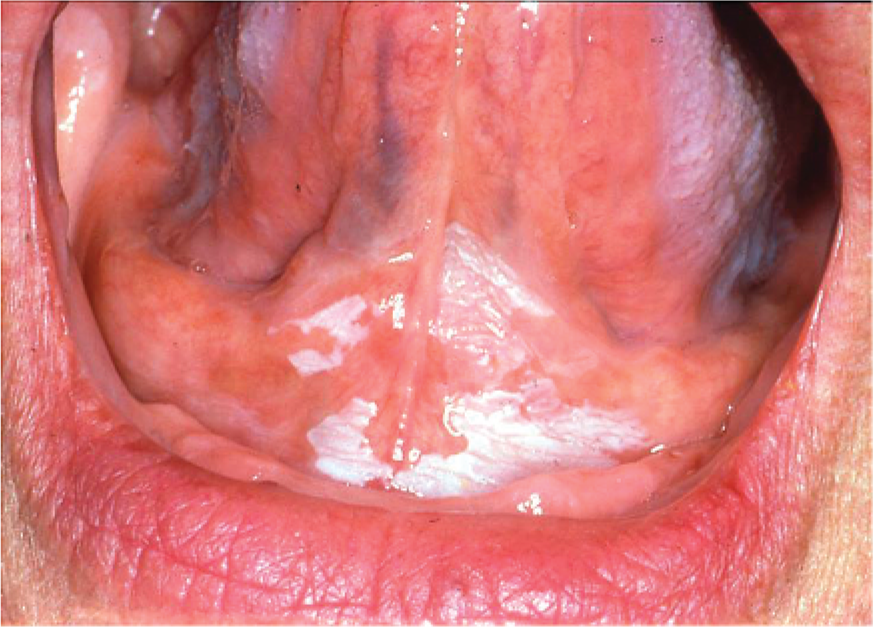
Leukoplakia on floor of mouth with some areas of erythroplakia.
Isolated red patches with a velvety texture and bright red appearance are suggestive of an erythroplakia and highly suspicious, particularly if affecting the floor of the mouth. Biopsy of these lesions frequently shows severe epithelial dysplasia of frank carcinoma.
Speckled leukoplakias are considered to be a variant of either leukoplakia or erythroplakia. They are generally considered to be potentially malignant. White lesions occurring inside the angles (commissures) of the mouth frequently have a speckled appearance (Fig. 4) and are usually associated with chronic candidal infection particularly in patients who smoke tobacco.

Speckled leukoplakia at commissure of mouth.
Pigmented lesions
Most pigmented lesions in the mouth are benign; however, biopsy is often required to exclude sinister pathology. Isolated patches of oral mucosal pigmentation with a black or brown colour, particularly if growing in size, should be regarded with suspicion, although melanoma in this site is extremely rare.
Kaposi's sarcoma is also rare but may present intra-orally as red, purple or brown patches that then develop into a swelling and may ulcerate. These tend to occur on the gingiva or palate and there may be other oral manifestations of HIV infection such as persistent candidal infection.
Oral lichen planus
A number of other oral conditions have been associated with an increased risk of developing oral cancer including oral lichen planus. The malignant potential of oral lichen planus remains controversial but is reported as 0.5 to 2% over a five year period. Oral lichen planus affects about 1% of individuals and is generally a disease of the middle aged or elderly with a female predilection.
Oral lichen planus has many clinical variants and can present as ulcerative, red or white patches (Fig. 5) with or without a typical reticular or ‘lace-like’ appearance. The patient may also have skin or genital involvement that can assist in the diagnosis of oral lichen planus. Oral lichen planus may be asymptomatic and noticed by the patient's dentist during a routine check-up. Ulcerative and atrophic (red) lesions of oral lichen planus are usually painful and may cause difficulty eating.
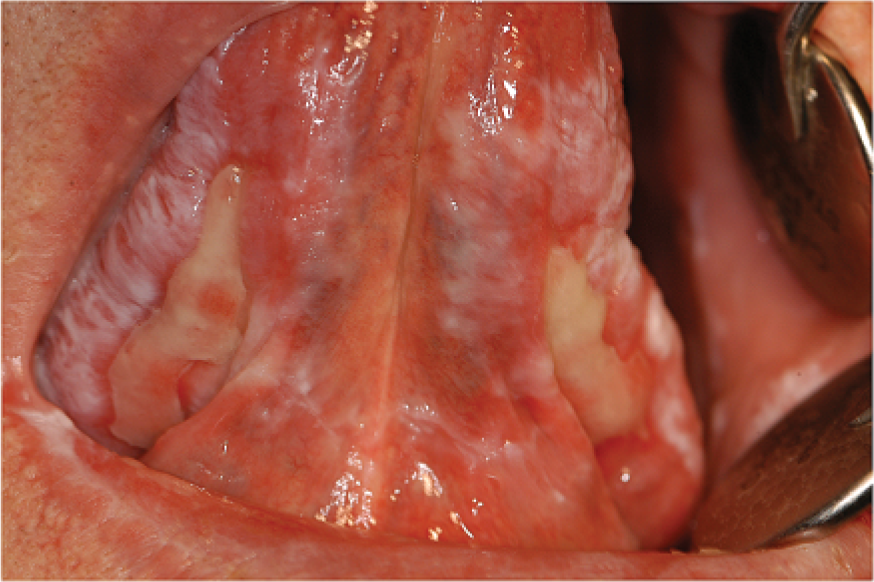
Oral lichen planus on ventral surface of tongue, with white, red and ulcerative lesions.
Swellings
The majority of swellings in the mouth are inflammatory or due to benign neoplasms or developmental lesions; however, a number of primary and secondary malignant lesions can appear as swellings on the oral mucosa and should be regarded with suspicion, particularly if they have recently appeared or there is no obvious explanation such as a dental infection or trauma from a tooth. Soft tissue swellings that are associated with ulceration and/or red or white patches are of particular concern.
Lip lesions
Cancer of the lip is usually slow growing and nearly always affects the lower lip. Patients may attend with a ‘cold sore’ that does not heal. Persistent shallow ulcers of the lip and/or red or white patches are suspicious.
Other clinical manifestations
Sudden unexplained loosening of the teeth may indicate spread of oral cancer to the adjacent bone or a metastatic deposit in the jaw from malignancy elsewhere.
Oral signs and symptoms may be the first indication of the presence of leukaemia, particularly of the acute types. Oral manifestations of acute leukaemia include:
spontaneous or excessive bleeding from the gums gingival overgrowth recurrent oral infections a sudden onset of generalized oral soreness or severe ulceration
Evaluation and referral
History and examination
A detailed history of the patient's oral symptoms is essential and should include enquiry about the duration of the oral lesion and associated symptoms, such as pain or discomfort. A history of skin or genital lichen planus is particularly relevant. Patients should be asked whether they have regular dental check-ups and when they last saw a dentist. A social history is important as tobacco and a high alcohol consumption are risk factors for oral cancer.
Examine the patient methodically starting with the lymph nodes, lips and then all surfaces inside the mouth. A good examination light or a small torch is needed and patients should be asked to remove their dentures. Note the site, size and appearance of any oral lesion together with any clinical features suggestive of possible malignancy (Box 2). Solitary mouth ulcers lasting more than 3 weeks with no obvious cause and red or white patches including lesions of oral lichen planus should be considered suspicious.
Patients who have no discrete oral lesions but who present with unexplained symptoms such as persistent soreness of the mouth, excessive or spontaneous bleeding of the gums or sudden onset of mouth ulcers may have an underlying systemic illness and require appropriate investigations including blood tests. If a diagnosis cannot be made and the symptoms persist, or become worse, then prompt referral is needed. Patients with unexplained tooth mobility, particularly if sudden, should be advised to see a dentist as soon as possible. Patients who have been diagnosed as having oral lichen planus should have regular monitoring of their oral mucosa, as part of their dental check-up.
Referral
Urgent referrals for oral lesions should be made to a specialist in oral medicine or oral and maxillofacial surgery, depending on local arrangements within secondary care. If you are unsure about the degree of urgency for the referral of an oral lesion, then telephone your local specialist unit or discuss with the patient's dentist, if available at the time. Investigations for suspicious oral lesions should not be undertaken in primary care as they may delay diagnosis and treatment of a potential oral cancer. Box 4 summarizes the NICE referral guidelines for suspected head and neck cancer including suspicious oral lesions. There may be suspicious oral lesions that do not exactly fit into these guidelines (e.g. white patch with speckled appearance). If in doubt, refer urgently.
GP support for oral cancer patients
The GP has a pivotal role in supporting and counselling patients and their families, once the diagnosis of oral cancer has been confirmed and then throughout treatment, which can be an extremely debilitating and protracted period of time.
The management of oral cancer is complex and requires input from a multidisciplinary team, including maxillofacial surgeons, oncologists, radiotherapists, speech therapists, specialist nurses and clinical psychologists. Specialists in palliative care will also be involved for patients who are terminal, either as a consequence of advanced disease or following failed treatment. The majority of oral cancer patients require surgery, radiotherapy or a combination of both. Over the last two to three decades, there have been great advances in the reconstruction of patients who have undergone ablative surgery for oral cancer and this has led to a greatly improved cosmetic and functional result, with a significantly better quality of life. Reconstruction of both hard and soft tissues, lost as a result of tumour resection, is now routinely undertaken at the time of surgery and in many cases dental implants can be placed so that patients can have their dentition replaced by a prosthesis.
Patients who receive radiotherapy for oral cancer develop an oral mucositis, which is extremely sore and difficult to treat. The patient's oncology team will, however, have a protocol for managing this. Other complications include a dry mouth, altered taste and oral candidosis. In the longer term, patients are more susceptible to dental decay and may develop osteoradionecrosis of the jaws, although modern methods of radiotherapy have reduced this complication. A dental check-up should be undertaken prior to radiotherapy. The patient's dentist will also have a significant role to play in the monitoring and maintenance of oral and dental health in patients with oral cancer, following completion of treatment, and will keep in touch with the multidisciplinary oncology team.
Summary of NICE guidelines for referral of head and neck cancer
Mouth ulcer(s) persisting for more than 3 weeks Lumps in the mouth persisting for more than 3 weeks Red or white patches in the mouth—including suspected lichen planus—that are painful, swollen or bleeding.
Note: For patients with persistent symptoms/signs related to the oral cavity in whom a definitive diagnosis of a benign lesion cannot be made, refer or follow up until the symptoms and signs disappear. If the symptoms/signs have not disappeared within 6 weeks, make an urgent referral.
Unexplained lump in the neck, of recent onset Previously undiagnosed lump that has changed over a period of 3–6 weeks Unexplained persistent swelling in the parotid or submandibular gland Unexplained persistent sore or painful throat Unilateral unexplained pain in the head and neck area for greater than 4 weeks associated with otalgia (ear ache) but a normal otoscopy
If there is a POSITIVE finding on chest X-ray: Refer urgently to a team specializing in the management of lung cancer (to be seen within 2 weeks).
If there is a NEGATIVE finding on chest X-ray: Refer urgently to a team specializing in the management of head and neck cancer (to be seen within 2 weeks).
Patient education concerning smoking cessation and moderation of alcohol intake is crucial for this group of patients, who are particularly at risk from developing either a recurrence or another primary oral cancer.
Thankfully, the majority of patients treated for oral cancer nowadays will not suffer facial disfigurement, which often resulted from surgical procedures in the past. However, reconstruction may not be feasible or successful in all cases, particularly for those with advanced or recurrent disease. Patients with any form of facial disfigurement frequently suffer from self-image problems and may become depressed or socially isolated. Long-term support from their GP will therefore be required with input from a clinical psychologist if appropriate.
Macmillan Cancer Support and the Mouth Cancer Foundation can provide excellent information and support, post-diagnosis and during treatment and rehabilitation. ‘Changing Faces’ is a UK charity that supports and represents people who have disfigurements to the face, hand or body from any cause and has an experienced team that can provide advice and guidance.
Patients with oral cancer may be eligible for the disability living allowance (DLA) or attendance allowance (AA) depending on the care they require during and after treatment. Those who are terminally ill as a result of oral cancer, i.e. those with a progressive illness who are not expected to live more than 6 months, can claim AA and DLA straightaway. Patients receiving treatment for oral cancer in England are entitled to free prescriptions for all their medications and will require a Medical Exemption Certificate.
Prevention of oral cancer
Patients should be made aware of the increased risk of oral cancer associated with tobacco use, alcohol consumption and chewing of betel quid.
All patients, including those with full dentures, should have regular oral and dental check-ups, so any suspicious lesions can be detected early and a referral made for a specialist opinion.
Key points
Oral cancer, benign and potentially malignant lesions in the mouth may have a similar clinical appearance A solitary mouth ulcer that does not heal after 3 weeks should be urgently referred to an oral specialist for biopsy Red, white and pigmented lesions in the mouth should be regarded as suspicious Investigations for possible oral cancer should not be undertaken in primary care as this delays diagnosis and treatment Tobacco use and excessive alcohol consumption are the principal risk factors for developing oral cancer All patients should have regular dental check-ups, including an examination of their oral mucosa
Footnotes
Appendix
Oral Medicine is a small dental specialty with units attached to dental hospitals throughout the UK. Specialists in Oral Medicine undergo dental and medical training and have expertise in the diagnosis and management of oral mucosal conditions and other orofacial conditions. For further details, please see link to the British Society for Oral Medicine website www.bsom.org.uk