
Abstract
Chronic kidney disease (CKD) is a term that describes any form of chronic kidney damage and also the circumstance where a patient's estimated glomerular filtration rate (eGFR) is less than 60 ml/min/1.73 m2. The aims of this article are to explain this definition, including its limitations, describe the epidemiology of CKD and discuss the pros and cons of labelling patients as having CKD.
The GP curriculum and chronic kidney disease
Searching the Royal College of General Practitioners (RCGP) Curriculum Map with the keyword ‘kidney’ reveals only a single item, which refers to adult polycystic kidney disease. This is surprising but indicative—among other things—of the low profile of chronic kidney disease (CKD) before UK guidelines were published in 2005 and CKD was introduced as a clinical domain in the general practice Quality and Outcomes Framework (QOF) in 2006.
CKD—definition and classification
Definition
A patient has CKD if he or she has
any significant structural abnormality of the kidneys, e.g. demonstrated on ultrasound scanning or by other radiological imaging persistent proteinuria or haematuria (after exclusion of other causes such as urological disease) or an estimated glomerular filtration rate (eGFR) of less than 60 ml/min/1.73 m2
Classification
CKD is classified into five stages depending on the patient's eGFR (Table 1). It is important to recognize that patients should not be classified as having CKD stages 1 or 2 purely on the basis of their eGFR.
Classification of CKD

Notes The suffix ‘P’ can be applied to the stage of CKD if the patient has significant proteinuria, defined as a urinary albumin:creatinine ratio (ACR) greater than 65 mg/mmol or protein:creatinine ratio (PCR) greater than 100 mg/mmol.
What is the eGFR, and why is it useful?
The best overall measure of kidney function is the glomerular filtration rate (GFR), but it is difficult to measure this directly or to estimate it, these requiring either injections of a marker substance with repeated blood sampling or a single blood sample with analysis of a 24 hour urinary collection. The routine laboratory measurement that best reflects the GFR is the serum creatinine, but this is affected by things other than the GFR, most importantly—because creatinine is a product of muscle metabolism—the patient's muscle mass. If two patients have the same GFR, then the one with greater muscle mass will have higher serum creatinine. Similarly, if two patients have the same serum creatinine, then the one with the greater muscle mass will have higher GFR. This effect can be substantial: if an elderly woman has the same serum creatinine as a young man, then she has a GFR of about half as much.
The reason that the eGFR gives a truer picture of the patient's renal function than the serum creatinine is because it makes allowance for differences in muscle bulk between patients. It is calculated from the serum creatinine using a formula that was first developed in a US study of Modification of Diet in Renal Disease (hence ‘MDRD formula’) that takes account of three variables that affect the patient's likely muscle mass, these being:
age—on average, younger adults have more muscle than older adults sex—on average, men have more muscle than women and race—on average, Afro-Caribbeans have more muscle than whites
All biochemistry laboratories now provide the eGFR with any measurement of serum creatinine originating from primary care, taking account of the patient's age and sex, both of which are always known because they are used for sample identification purposes, and with a caveat added to the results' display to say that the eGFR should be multiplied by a factor of 1.2 to obtain a correct value if the patient is Afro-Caribbean.
Limitations of the eGFR
In some circumstances, the eGFR is unreliable. Its calculation, as explained above, is based on the assumption that patients are of average muscle bulk for their age and sex; hence, it is obviously inaccurate for those who depart markedly from this average. The eGFR will be an overestimate of true renal function in any patient who is underweight and wasted and an underestimate in any patient with greater than average muscle bulk, most dramatically in the ‘body builder’.
It is also important to recognize that the eGFR cannot be used in all circumstances that the serum creatinine is measured. It depends on renal function being stable; hence, it can never be applied to any patient with acute kidney injury (acute renal failure), and for this reason some biochemistry laboratories do not report eGFR on blood samples taken from hospital inpatients. It cannot be used in children (aged less than 18 years) or pregnant women, and it has not been validated for ethnic groups other than Caucasians and Afro-Caribbeans. Another important issue is that very few patients over the age of 80 years were included in the population whose data were used as the basis for the MDRD formula; hence, the reporting of eGFR in the elderly is much less secure than in younger adults, and it is in the elderly that most of the problems associated with determination of CKD arise.
Epidemiology of CKD
CKD, in particular CKD stage 3, is very common. Table 2 shows the age-related prevalence of CKD stages 3–5, with that for CKD stage 3 rising from 1.4% in those aged less than 65 years to about 30% in those aged 75 years or more. Figure 1 shows prevalence of the different stages of CKD in a typical general practice population.
Prevalence of CKD (percentage of the population affected)

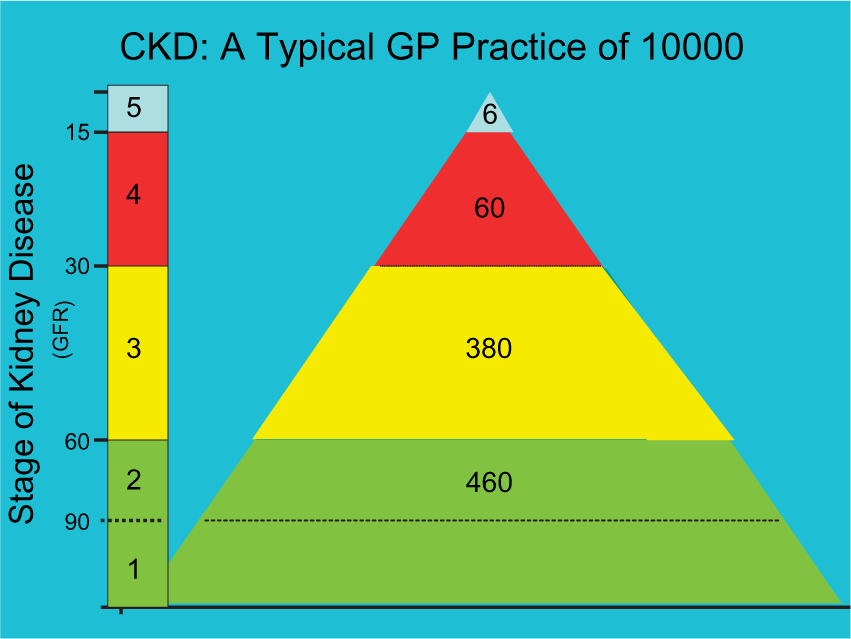
Prevalence of different stages of CKD in a typical GP practice of 10 000 patients.
What is the cause of CKD stage 3? The vast majority of patients are elderly and do not have any discrete, recognizable renal pathology. Most nephrologists regard them as having age-related decline in renal function that may be more pronounced than average. They do not require renal investigation unless eGFR is declining rapidly or there is reason to suspect a renal inflammatory cause (most typically suggested by significant proteinuria and/or haematuria).
The clinical significance of CKD
The definition of CKD and its appearance in the QOF have led GPs to determine whether or not their patients have the condition, which has revealed many cases—often referred to as an ‘epidemic’—of CKD stage 3. Is this good or bad? Opinion within the renal community is divided. Some argue that anything that raises the general profile of kidney disease is likely to be beneficial to kidney patients and therefore a good thing. However, aside from this ‘political’ viewpoint, there are significant arguments both for and against.
The arguments ‘for’ CKD stage 3
Patients with CKD stage 3 are at increased risk of death, particularly cardiovascular (Fig. 2). Many of these will already be known to be at increased cardiovascular risk because they have other recognized risk factors such as hypertension or diabetes, but increased risk on account of CKD is present even after allowance for these co-morbidities, and this risk is modifiable. The Heart Outcomes and Prevention Evaluation (HOPE) study of patients with pre-existing vascular disease or diabetes found that the frequency of cardiovascular death was almost twice as high in the 10% who had a serum creatinine of over 124 micromol/l (which equates to an eGFR of about 52 ml/min/1.73 m2 in a 70-year-old man and about 40 ml/min/1.73 m2 in a 70-year-old woman), compared to the 90% who had a serum creatinine below this level. This effect was independent of known cardiovascular risks and treatment and could be substantially reduced by the angiotensin converting enzyme inhibitor (ACEi), ramipril.

Five year risk of death in a typical GP practice of 10 000 patients depending on CKD stage. The risk is displayed as a percentage and (in brackets) as the number of patients.
A further argument that it might be beneficial to detect patients with CKD stage 3 arises from the observation that the GFR of many patients with known renal disease tends to fall inexorably with time, and the rate of this decline can be reduced by achieving good control of blood pressure. It is therefore tempting to think that detection of CKD at an early stage could allow intervention that would slow down progression and thereby restrain the number of patients whose renal function deteriorates to the point that renal replacement therapy is required, which is increasing in the UK by about 5% year-on-year and a very considerable burden both to the individuals concerned and to the health service finances.
Inducing GPs to screen the population for CKD stage 3 might therefore allow cardiovascular interventions to be targeted at a high-risk group and also reduce the number of patients who develop advanced CKD and the requirement for renal replacement therapy. It has not, however, been proven that such a strategy is effective in achieving either of these aims.
The arguments ‘against’ CKD stage 3
The data showing that having an eGFR that is modestly lower than average is associated with increased cardiovascular risk are strong and also that such risk can be modified by treatment with an ACEi, but is it sensible to describe patients with slightly low eGFR as having CKD? Many patients given this label will naturally assume that this means that they have something significantly wrong with their kidneys, and if the label CKD is qualified by ‘stage 3’, they will be convinced that things must be bad. Some may be concerned that the need for dialysis is imminent, as may their families and friends. More than one patient with CKD stage 3 has arrived in my clinic accompanied by someone who declared that they were prepared to give them a kidney and wanting to know how long it would take to organize this: death or dialysis was surely just around the corner. Figure 3 shows that the chance of a patient with CKD stage 3 requiring renal replacement therapy in the next 5 years is 1.3%.
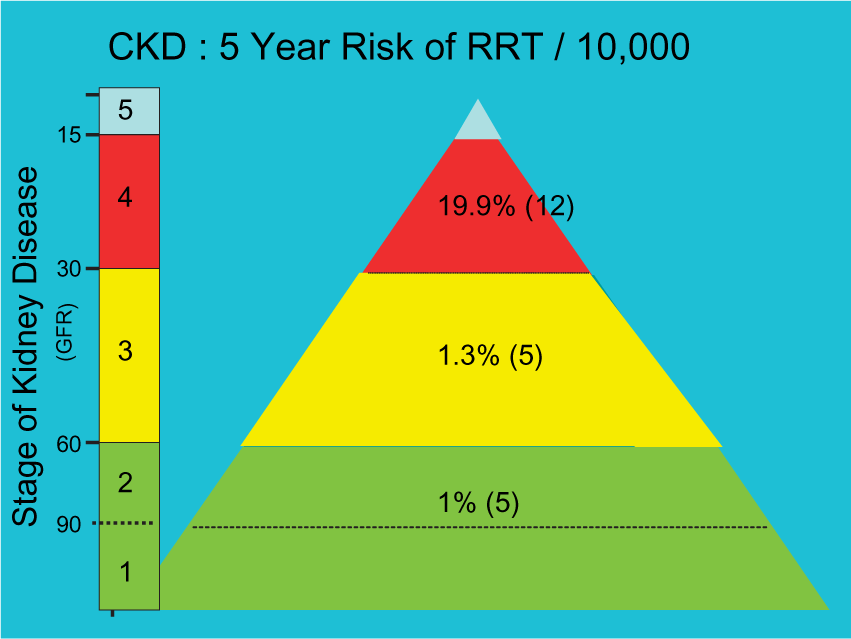
Five year risk of requiring renal replacement therapy (RRT) in a typical GP practice of 10 000 patients depending on CKD stage. The risk is displayed as a percentage and (in brackets) as the number of patients.
The repercussions of giving a patient a label can be extreme, and those against the business of classifying many elderly people as having CKD stage 3 emphasize that we should not apply labels that can lead reasonable people to make incorrect assumptions about their health. Doctors who tell a patient that they have CKD stage 3 must explain what this means and/or provide access to reliable sources of information, which should not leave the patient thinking that they have some terrible kidney problem but that there is particularly good reason to try to get good control of their blood pressure and that they need a kidney check-up once per year.
Key points
A patient has CKD if he/she has any significant structural abnormality of his/her kidneys, persistent proteinuria or renal haematuria, or an eGFR of less than 60 ml/min/1.73 m2
eGFR is calculated from the serum creatinine by a formula that takes account of the patient's age, sex and race CKD stage 3 is defined by an eGFR in the range 30–59 ml/min/1.73 m2 and is very common, affecting about 30% of people aged over 75 years Patients with CKD stage 3 are at increased cardiovascular risk, which can be reduced by ACEis, but they are at very low risk of their renal function deteriorating to the point that renal replacement therapy is required Much unnecessary anxiety can be created by labelling patients as having CKD stage 3: doctors using this term must explain what it means and/or provide access to reliable sources of information to emphasize that the patient (i) does not have a terrible kidney problem, (ii) does need to have their blood pressure well controlled and (iii) does need an annual renal check-up