
Abstract
Unintended pregnancy is a major public health issue with around 53 million abortions being performed worldwide each year. An estimated 40% of all pregnancies are unplanned and 60% of these end in abortion. Rates of unplanned pregnancy and abortion remain high in the UK compared with other European countries and each year around 200 000 pregnancies in the UK end in termination. Use of emergency contraception (EC) has the potential to reduce rates of unwanted pregnancy. With around a third of all EC prescriptions issued in primary care, the GP and primary health care team have a major role in the provision of a sexual health and EC.
The GP curriculum and emergency contraception
Royal College of General Practitioners (RCGP)
Are able to outline prevention strategies relevant to women
Understand the importance of confidentiality and informed consent
Are familiar with legislation relevant to women's health (e.g. consent for minors)
Can describe and implement the key national guidelines that influence health care provision for women's problems
RCGP
Contraception—effectiveness rates, risks, benefits and appropriate selection of patients for all methods, including methods of emergency contraception (EC)
Contraception—the safe provision of all methods of oral contraception (including emergency hormonal contraception)
Reducing rates of unwanted pregnancy and abortion can be by primary prevention with contraception or secondary prevention with an abortion. ‘Emergency contraception’ can be defined as use of a drug or device to prevent pregnancy after intercourse (Glasier, 1997).
Implicit in the term EC is that it is meant as a ‘safety net’ for occasional use rather than for regular contraception. Terms such as postcoital contraception or ‘the morning-after pill’ can cause confusion and are best avoided. A Judicial Review in 2002, which ruled that pregnancy begins with implantation rather than fertilization, meant that EC is considered a method of contraception rather than an abortificient (Department of Health, 2002).
Patients presenting for EC tend to be nulligravid and young. They have often previously used EC and condoms are frequently their main method of contraception. Condom breakage is the most common indication for EC (Tyden et al., 1998).
Risk of pregnancy
The risk of pregnancy depends on several factors. These include:
the age of patient
the number of episodes of unprotected sexual intercourse (UPSI) this cycle and
the point of UPSI within the menstrual cycle
For instance, fertility is minimal during the initial 3 days of the cycle and women are most likely to become pregnant around 7 days before until 2 days after ovulation. The probability of pregnancy following an episode of UPSI is estimated to be around 3% but that rises to around 30% during the fertile period. Importantly, the ‘fertility window’ is highly variable even in patients with regular cycles and there is no point in the cycle that can be considered without risk of pregnancy (Wilcox et al., 2000). Where there are doubts about the risk of pregnancy and need for EC, there is little harm in issuing EC.
Indications for EC
EC is indicated either following unprotected intercourse or where there has been contraceptive failure. The definition of contraceptive failure depends on the type of contraception used and some common examples are outlined in Table 1.
Contraceptive failure and indication for EC

Faculty of Family Planning and Reproductive Health Care Clinical Effectiveness Unit (2005).
Faculty of Sexual and Reproductive Healthcare Clinical Effectiveness Unit (2009).
ABPI Medicines Compendium (2009).
A consultation involving EC should be holistic and patient centred and has the overarching aim of reaching a shared understanding with the patient and an informed decision about EC. Moreover, as part of delivering a holistic sexual health service, the consultation provides an opportunity to explore the woman's needs for regular contraception, the possibility of sexual abuse and provide general sexual health advice about risk and prevention of sexually transmitted infection (STI). As always, there should be a safety net with advice about the possibility of an ectopic pregnancy and how it may present.
Data gathering
Achieving those consultation aims requires basic data gathering initially and some of the important aspects and relevant questions are outlined in Box 1.
Making diagnoses and decisions
Having elicited the relevant data as well as the patient's preferences, it should now be possible to offer a management plan. This may be reassurance that EC is not required and perhaps opportunistic sexual health advice. Where a patient is unsuitable for EC, she should have a pregnancy test 3 weeks after the date of UPSI. If EC is required, there should follow a discussion about the available methods.
Explanation phase
As well as an outline of the available methods of EC, patients should also be aware of their efficacy and the adverse effects associated with their use. Consistent with a patient-centred consultation, there should be an open two-way exchange of information and opinion with the overarching aim of achieving a shared understanding and an informed patient choice. Some of the important components of the explanation phase are outlined in Box 2.
Providing an overview of contraceptive methods
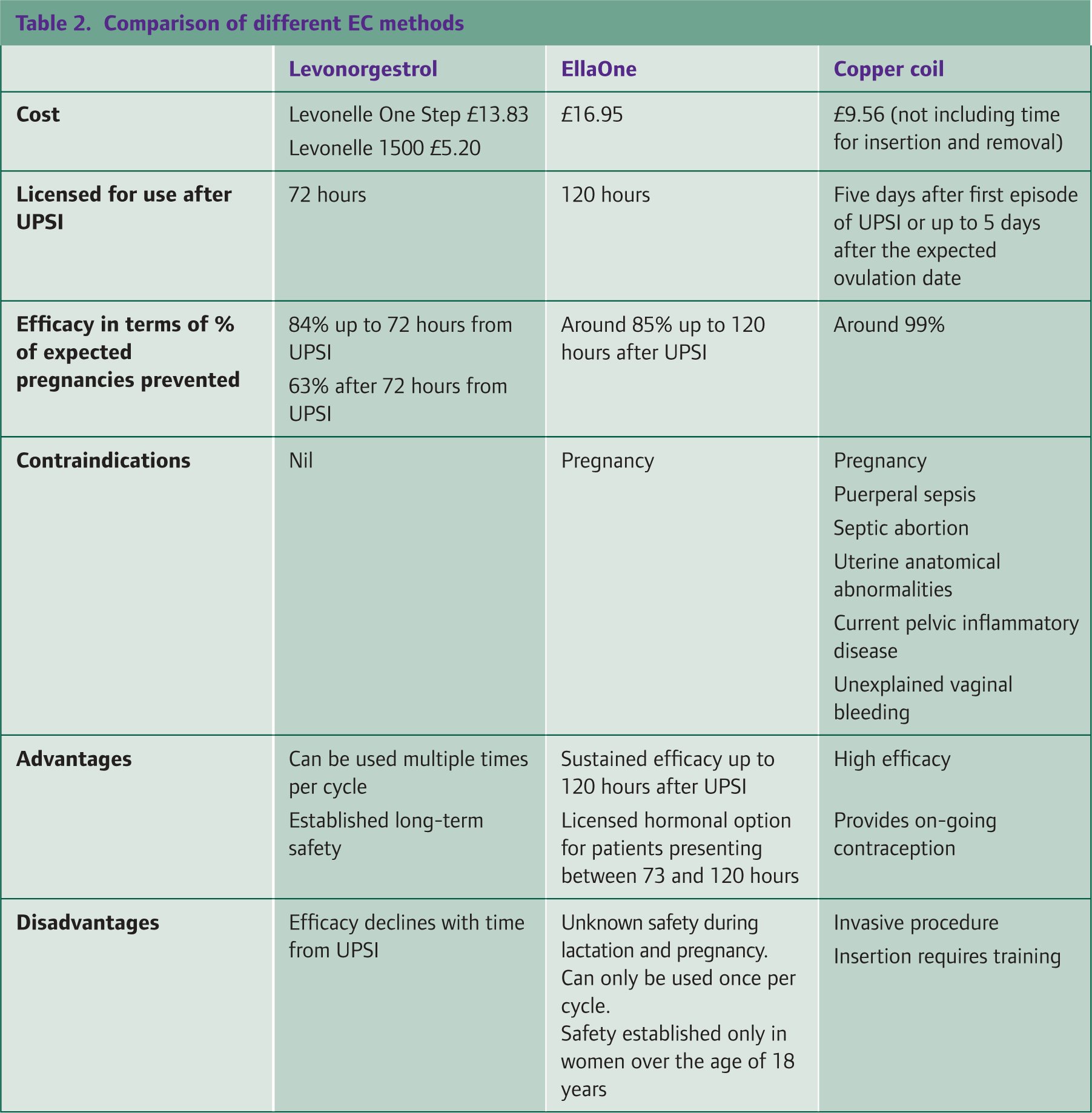
The approaches available for EC fall into the two categories: hormonal and non-hormonal. The type of EC used depends largely on patient preference and the time between presentation and UPSI. Table 2 provides a comparison of the different EC methods. Women should receive both oral and written information as part of contraceptive counselling.
Comparison of different EC methods
Data gathering
Establish indication for EC
Number of episodes of UPSI this cycle
Details of the contraceptive failure
Exclude established pregnancy
Menstrual history
Determine if ovulation* or implantation** is likely to have occurred by enquiring about menstrual history:
When was your last menstrual period?
Was it normal and on time?
What is your usual cycle length?
Timing of UPSI in relation to last menstrual period/ovulation
Past medical history and medication
Previous use of EC this cycle
Current medications particularly liver enzyme inducers
Significant medical history
Establish if any contraindications to EC use
Other issues
STI risk assessment
Determine Fraser competency in patients under 16 years
Determine possibility of abuse
Ovulation occurs around day 14 in a 28 day cycle
To calculate likely date of implantation, add 5 days to the date of ovulation
Explanation phase of the EC consultation
Provide verbal and written information about the available EC, their efficacy/mode of actions and side effects
Explain hormonal EC does not provide contraceptive cover for the remainder of the cycle and need for effective contraception or abstinence
Advise in event of vomiting within 2 hours of taking levonorgestrel or within 3 hours of taking EllaOne
Opportunistic sexual health advice
Safety net in the event of lower abdominal pain or a missed or late period
Hormonal EC: levonorgestrel
Licensed in the UK in 1999, levonorgestrel is available either on prescription as Levonelle 1500 or over the counter as Levonelle One Step. It is taken orally as a 1.5 mg tablet as soon as possible following coitus. Following its deregulation in 2001, levonorgestrol is now widely available to buy from pharmacies or through the National Health Service (NHS) from Patient Group Directives and Family Planning Centres, as well as from the GP. As a pilot scheme, in some parts of the UK, levonorgestrel EC is being offered to under 16s free-of-charge directly through community pharmacies.
Several studies have found the efficacy of levonorgestrol declines with time from UPSI: when taken within 24 hours of UPSI, levonorgestrol avoids 95% of expected pregnancies but only 58% if taken between 49 and 72 hours. Although levonorgestrol may be used between 73 and 120 hours after UPSI, patients should be aware of its limited efficacy. Delay of the luteinizing hormone (LH) surge and thereby ovulation is felt to be the primary mode of action of levonorgestrel (Croxatto et al., 2001).
According to the UK Medical Eligibility Criteria for Contraceptive Use (UKMEC, 2009), there are no absolute contraindications to the use of levonorgestrol. Although it can cause side effects such as abdominal pain, irregular bleeding and nausea, these tend to be minor and short lived (Faculty of Sexual and Reproductive Healthcare (FSRH), 2009). Levonorgestrel can be safely used on multiple occasions in the same menstrual cycle and inadvertent exposure of the developing embryo to levonorgestrel is not known to be harmful.
Patients should be advised that a repeat dose of levonorgestrol is required in the event of vomiting within 2 hours of taking the tablet. Moreover, effective contraception should be used for the remainder of the cycle and if EC is used because of missed oral contraceptive pills, women may resume normal pill taking within 12 hours.
Hormonal EC: ulipristal
In 2009, EllaOne became available for use as EC and is the only licensed hormonal option for patients presenting between 73 and 120 hours after UPSI. EllaOne contains 30 mg ulipristal acetate and is taken orally as soon as possible following UPSI. In the event of vomiting within 3 hours of taking EllaOne, a further dose is recommended. EllaOne is significantly more costly than levonorgestrol (£16.95 vs £5.20) and works both by inhibiting ovulation and reducing the risk of implantation by altering endometrial histology (Stratton et al., 2000).
The results of one double-blind randomized trial found the efficacy of EllaOne to be at least as good as levonorgestrol in patients presenting up to 72 hours following UPSI (Glasier et al., 2010). Unlike levonorgestrol, however, it maintains efficacy for up to 120 hours (Fine et al., 2010).
There are important restrictions and drawbacks to the use of EllaOne though. For example, EllaOne is not licensed for use in patients under 18 years and should be avoided in patients with severe hepatic impairment and women with asthma requiring oral steroids. Contraindications to the use of EllaOne include pregnancy and hypersensitivity to any of its excipients. Moreover, there is limited data on the potential teratogenic effects of EllaOne.
EllaOne is currently available on prescription only and is listed in the British National Formulary (BNF) as a ‘black triangle’ drug. This means that any adverse events should be reported to the Medicines and Healthcare Products Regulatory Agency (MHRA) so that they can be monitored.
Side effects of headache, nausea and abdominal pain are reported in around 1 in 10 EllaOne users. Unlike levonorgestrol, repeated administration of EllaOne in the same menstrual cycle is not recommended and patients should be aware that their next menstrual period may be delayed. A delay in onset of menstruation of 7 days is recommended as the threshold for doing a pregnancy test (Association of the British Pharmaceutical Industry Compendium, 2010).
There are various drug interactions associated with use of EllaOne. For instance, use of EllaOne should be avoided in patients taking antacids or proton pump inhibitors. In vitro data also suggest that drugs such as ketoconazole or rifampicin that affect CYP3A4 may affect efficacy of EllaOne. Another concern is the potential for EllaOne to attenuate the efficacy of hormonal contraception and current guidance recommends using barrier contraception until the following period (Mansour, 2009).
Perhaps, future EC trials will demonstrate that EllaOne is more effective than levonorgestrol, which may mean that the greater cost of EllaOne is offset by the reduction in unwanted pregnancies. Providing no major safety issues are identified, EllaOne may eventually supersede levonorgestrol as the first-line choice of hormonal EC.
Non-hormonal EC
The copper coil was first recognized as a means of EC in 1976. It has been shown to have consistently low failure rates of around 0.1-0.2% when inserted postcoitally (Bastianelli et al., 2008). The emergency intrauterine device (IUD) is licensed for use up to 5 days following UPSI or 5 days after ovulation (day 19 in a 28 day cycle).
The IUD may be inserted at any point in the menstrual cycle and unlike levonorgestrol, its efficacy is maintained up to 5 days following UPSI. The fact that the IUD can provide ongoing regular contraception is a further benefit. Its mechanism of action relies on the copper ions being directly toxic to sperm and also generating an inflammatory reaction in the uterus and fallopian tubes that inhibits implantation (Allen and Goldberg, 2007).
However, the copper IUD is used in only around 3% of patients presenting for EC. Its limited uptake may partly be due to the fact that the copper coil is offered as an option for EC to only a minority of women (Moss et al., 2009). Potential limitations that limit its use (Rickards et al., 2004) include:
Insertion is an invasive procedure and therefore carries risk of secondary bacterial infection
Insertion requires special training that limits the availability of the copper IUD for EC
Insertion may require the patient to make a further appointment
IUDs cannot be used for EC where there have been multiple episodes of UPSI
Use of the IUD is generally safe. However, expulsion occurs in around a fifth of women usually around menstruation and the most common side effect that leads to discontinuation of copper IUDs is bleeding problems. Fortunately, uterine perforation occurs in less than 1 in 1000 procedures (NICE and National Collaborating Centre for Women's and Children's Health, 2005). Lastly, women deemed to be at high risk of STIs require prophylactic antibiotics (e.g. a single 1 g dose of azithromycin) prior to IUD insertion.
Explaining efficacy
Patients should be aware that EC is associated with a failure rate although translating research data on efficacy into patient-friendly language can be difficult. Some example phrases to explain efficacy are given below [Clinical Knowledge Summaries (CKS), ‘How effective is emergency contraception?’].
If 1000 women have unprotected sex in the fertile time of their menstrual cycle and do not use EC, about 80 of these women will become pregnant. Use of levonorgestrel EC will prevent pregnancy in 70 of these 80 women, and use of the copper IUD will prevent pregnancy in 79 of the 80 women.
Alternatively, the effectiveness of levonorgestrol can be expressed as:
the chance of pregnancy is 2% when using Levonorgestrol up to 72 hours after UPSI and 4% for women presenting between 72 and 120 hours.
Similarly, for EllaOne:
two women will fall pregnant if 100 women received EllaOne up to five days after UPSI or the chance of pregnancy is 2.1% when using EllaOne up to 120 hours after UPSI
Lastly, the efficacy of the Copper IUD may be expressed as:
The EC IUD is 99.9% effective
Liver enzyme inducers, breast-feeding and post-partum EC
There are a few important differences in EC choice for patients who are post-partum and those taking liver enzyme inducers. For instance, in the post-partum period, EC is not required in the event of UPSI or contraceptive failure for up to 3 weeks post-partum. Levonorgestrol may be used from day 21 and the copper coil should not be inserted in the first post-partum month. Levonorgestrol can be used safely (UKMEC Category 1) in breast-feeding women after 3 weeks post-partum (Faculty of Family Planning and Reproductive Health Care, 2004).
Co-administration of enzyme inducers reduces the efficacy of hormonal EC and guidance from the FSRH suggests that the copper coil should be first choice for these patients (Faculty of Family Planning and Reproductive Health Care Clinical Effectiveness Unit, 2006). EllaOne is not recommended for use in women taking enzyme inducers. A double dose of levonorgestrel (3 mg) is an option, although outside its licensed use. See Box 3 for examples of common liver enzyme inducers.
Liver enzyme inducers
Phenytoin
Carbamazepine
Barbiturates
Rifampicin
Chronic alcohol use
Sulfapyrazine
St John's wort
Need for future contraception
Determining risk of future unwanted pregnancy can be gauged by enquiring about the woman's use of regular contraception and previous use of EC. Use of a long-acting contraceptive may be helpful in a patient frequently attending for EC and the Quality and Outcomes Framework (QOF) offers a financial incentive for recording that women seeking contraception have been given advice about the use of long-acting reversible contraception (LARC). Sexual Health Indicator 3 is worth three QOF points on a sliding scale with a target range of 40–90% of women seeking EC being given advice. It states that:
The percentage of women prescribed emergency hormonal contraception at least once in the last year by the practice, who have received information from the practice about long-acting reversible methods of contraception at the time of, or within one month of the prescription.
It may be necessary to ask the patient to return for a further appointment for a full discussion about contraceptive options.
Advice regarding STI risk reduction
In addition to risk of pregnancy, the patient may also be vulnerable to STI following UPSI. With around 3% of sexually active women reporting previous Chlamydia infection, the consultation is a chance to provide opportunistic sexual health advice (Fenton et al., 2001) as well as advice on where to attend for STI testing if necessary.
Safety netting and follow-up
Women prescribed EC should be advised to return for a pregnancy test if they have not had a normal period within 3 weeks or within 7 days of the expected menstrual date. Patients should also be advised to seek medical attention promptly if they develop symptoms of an ectopic pregnancy such as lower abdominal pain or vaginal bleeding. Figure 1 summarizes the EC consultation in diagrammatic form.
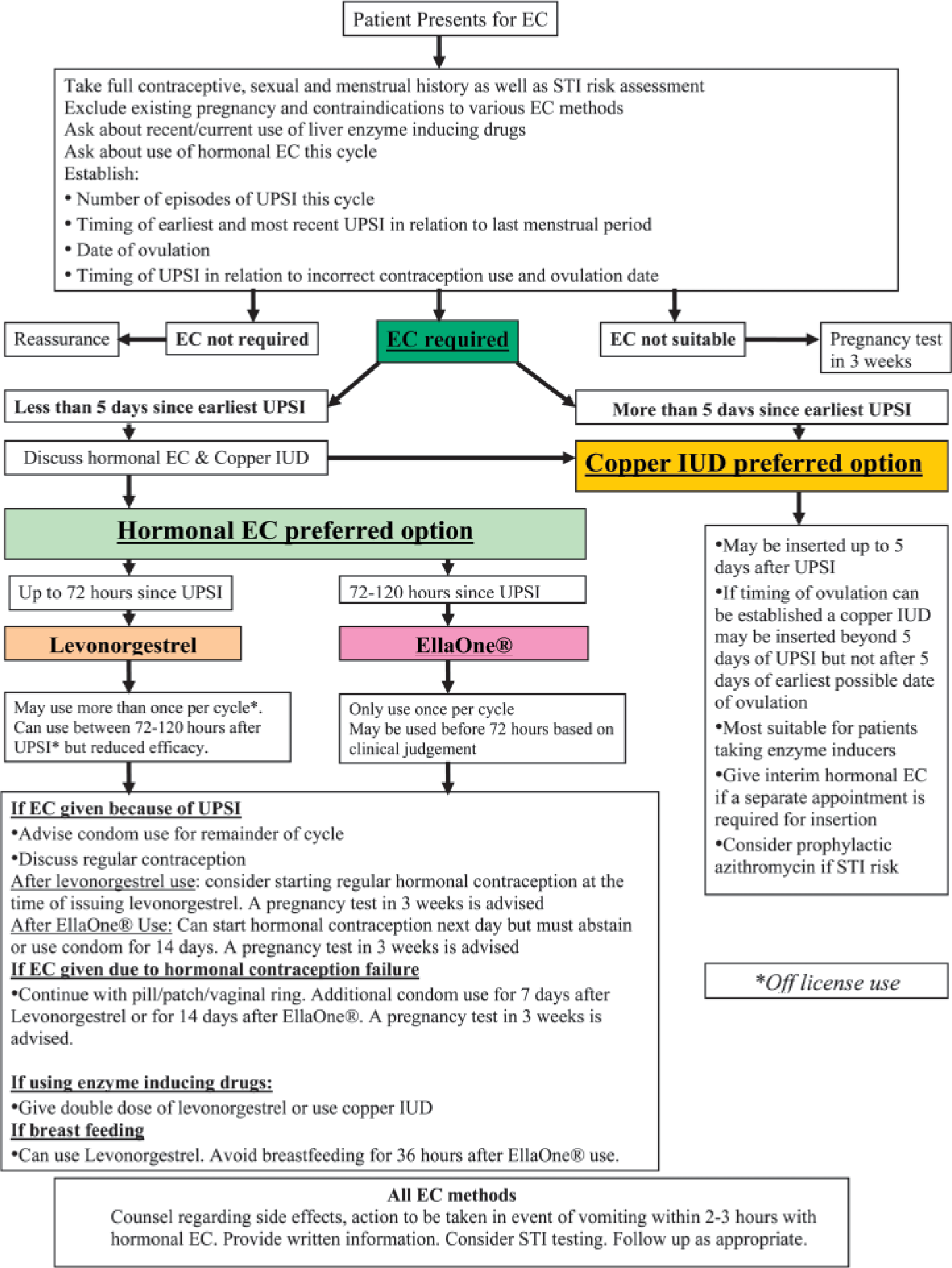
EC consultation summary.
Patients under 16 years
The legal age of consent to sexual activity is 16 years in Scotland, England and Wales and 17 years in Northern Ireland. When providing contraception to those under the legal age of consent, it is important to be sure that the young person is competent and to be alert to the possibility of abuse.
Deciding on whether a young person is competent or not requires reference to the Fraser Guidelines (see Box 4). Providing these criteria are met, a clinician may offer contraceptive advice and treatment to those under 16 years of age without parental consent. However, under the Sexual Offences Act, intercourse with a child under 13 years old is considered rape and in these cases, local child protection protocols should be followed as outlined in Working Together to Safeguard Children (HM Government, 2010).
The Fraser guidelines
The young person understands the health professional's advice
The health professional cannot persuade the young person to inform his or her parent or allow the doctor to inform the parents that he or she is seeking contraceptive advice
The young person is very likely to begin or continue having intercourse with or without contraceptive treatment
Unless he or she receives contraceptive advice or treatment, the young person's physical or mental health or both are likely to suffer
The young person's best interests require the health professional to give contraceptive advice, treatment or both without parental consent
Guidance from the General Medical Council (GMC) makes clear that the safety of children is paramount and concerns about possible child abuse may override that person's right to confidentiality (General Medical Council, 2007). Features suggestive of an abusive relationship include a significant age difference with the partner or use of substances as a disinhibitor. Be particularly vigilant if the partner is known to social services.
EC as a means of preventing abortion and unintended pregnancy
EC can be seen to form part of a wider primary prevention strategy for reducing rates of abortion and unintended pregnancies. The Teenage Pregnancy Strategy in 1999 aimed to halve the under-18 conception rate by 2010, partly through expanding access to EC. Unfortunately, cumulative evidence has not found a correlation between greater access to EC and a reduction in unintended pregnancy or abortion (Trussell et al., 2008).
Similarly, although advanced provision of EC in certain patient groups, suggested in draft National Institute for Health and Clinical Excellence (NICE) guidance (NICE, 2010), has shown to lead to increased and earlier use of EC, a Cochrane review found that it had little impact in stemming rates of unplanned pregnancies (Polis et al., 2007). Moreover, while knowledge of EC in the UK is high, one study found only 11.8% of women presenting for abortion had used EC in the cycle where conception occurred (Lakha and Glasier, 2006).
Perhaps these results indicate that, along with increased EC access, greater effort encouraging EC use and educating women about the need for EC is required if there is to be a significant population level impact on rates of unwanted pregnancy. Methods of LARC are associated with very low failure rates but are used by less than 8% of women in the UK. Ultimately perhaps, greater uptake of such user-independent contraception will have greater impact on reducing rates of unplanned pregnancy and abortion in the UK than EC (Allen and Goldberg, 2007).
Box 5 gives ideas about possible auditable areas of EC management and Box 6 gives links to further reading.
Audit
There are many possible audit topics in relation to EC.
Some examples include:
How many women are offered IUD at initial presentation?
How many women are assessed for STI risk?
Do all women presenting for EC receive written information about EC efficacy/safety/side effects?
Further reading
Faculty of Sexual Reproductive Healthcare: www.ffprhc.org.uk
e-GP. Contains a number of sexual health modules including EC
LARC advice leaflet: http://guidance.nice.org.uk/index.jsp?action=download(o=44129
Patient information leaflet regarding EC: www.patient.co.uk/health/Emergency-Contraception.htm
Key points
Unintended pregnancy is commonly encountered in primary care
Women presenting for EC should be made aware of the different EC methods in order to reach an informed contraceptive choice
Levonorgestrel remains the first choice for hormonal EC in patients presenting within 72 hours of UPSI and EllaOne is a licensed hormonal option in women presenting between 72 and 120 hours after UPSI
The copper coil is possibly the most effective form of EC but is underutilized; it may be used up to 5 days following UPSI
As part of providing a holistic sexual health service in primary care, it is necessary to explore other areas such as STI risk and the need for regular contraceptive