
Abstract
Our population is getting larger and older and with this, the burden of disease is predicted to increase. In addition, the issue of age discrimination is becoming increasingly relevant. This article provides an overview of how our population is changing, the effect this is likely to have and an overview of age discrimination. In addition, it aims to highlight the significant issues that will directly affect general practice and how these may be addressed.
The GP curriculum and the ageing population
Issues of the ageing population are addressed in multiple curriculum statements, primarily the objectives in
Knowledge of preventative strategies required in the care of older people The role of the GP in health promotion activities for older people in the community Awareness of inequalities in health care provision relating to older people Understanding of the interrelationships between health and social care for older people An understanding of legal issues that may arise with older people Mastering an approach that allows easy access to the primary health care team for older people, appropriate timing of appointments and an organization approach to the management of chronic conditions and co-morbidities
In addition, elements of the following curriculum statements are also considered:
The determinants of population ageing
The UK population had grown to 61.2 million by mid-2008. This growth has been most affected by changes in mortality and fertility, although movement and migration also affect population growth.
Mortality
Economic development, health care standards and social services have reduced mortality rates at all ages. Mortality is no longer significantly impacted by acute and infectious diseases but by chronic conditions that predominantly affect our ageing population. Thus, the mortality rate (the percentage of deaths in a given population in a given time) is declining resulting in more people living for longer.
Fertility, movement and migration
Fertility (in conjunction with mortality) has historically been a very potent factor in changing and controlling population shapes. Today, reduced fertility rates mean a reduction in the numbers of births and thus, with the ageing ‘Baby Boom’ generation, a change in the population shape as seen in Figure 1. Movement and migration on the other hand have a relatively low impact. While young immigrants have children increasing the fertility rate, previous generations of immigrants are ageing at the same time, so any effect is negligible.
The changing shape of the UK population—increasing numbers of older people.
Population ageing
The UK population is getting older as well as larger, impacted by reduced mortality and increased life expectancy. Data from the Office of National Statistics show that the median age in the UK has increased from 35 years in 1984 to 39 years in 2009 and those over 65 years account for 16% of the population and an increase of 1.7 million from 15% in 1983. In addition, the number of people over 85 years has increased two and a half times from 1984 to 2009, and over the same period, the number of 16-year-olds has dropped from 21% in 1984 to 19% in 2008.
This change is expected to continue with the median age estimated to rise to 42 years and those aged over 65 years accounting for 23% of the population by 2034 (Figure 1). The UK is not alone in this; the median age of the world's population is experiencing a similar increase.
What is old age?
In 2008, the Health Secretary, Alan Johnson, gave a speech entitled ‘Old age is the new middle age’. In this, he said ‘Health and social care services need to adapt to the changing needs of today's older people … to promote health in old age and help older people to maintain independence and quality of life’ (Johnson, 2008).
Alan Johnson placed healthy independent ageing at the centre of his vision for the future, a priority shared with other policy thinkers. In 2001, the Department of Health (DH) set out to develop ‘a comprehensive strategy for fair, high quality, integrated health and social care services for older people’ through the National Service Framework (NSF) for older people. This identified that while retirement still marks the entry into old age, there are in fact three distinct phases, each with differing health and social care needs. These are
entering old age the transitional phase between healthy and frail living the frail elderly
Clearly, the needs of a 65-year-old will normally be very different to those of an 85-year-old. Thus, treating older people is not one single challenge but is many, incorporating health promotion, chronic disease management and palliation to name but a few. However, the needs of older people cannot be determined by chronological age alone. The concepts of frailty and healthy life expectancy are crucial.
Frailty
Frailty has been defined differently by different authors. Gilleard and Higgs (2010) defined frailty as ‘those individuals whose “aged” state is seen to put them at risk of adverse outcomes’. Drey et al. (2011) highlight the importance of identifying those who are frail, with correlations between frailty and increased general practice consultations, polypharmacy, co-morbidities and cardiovascular disease.
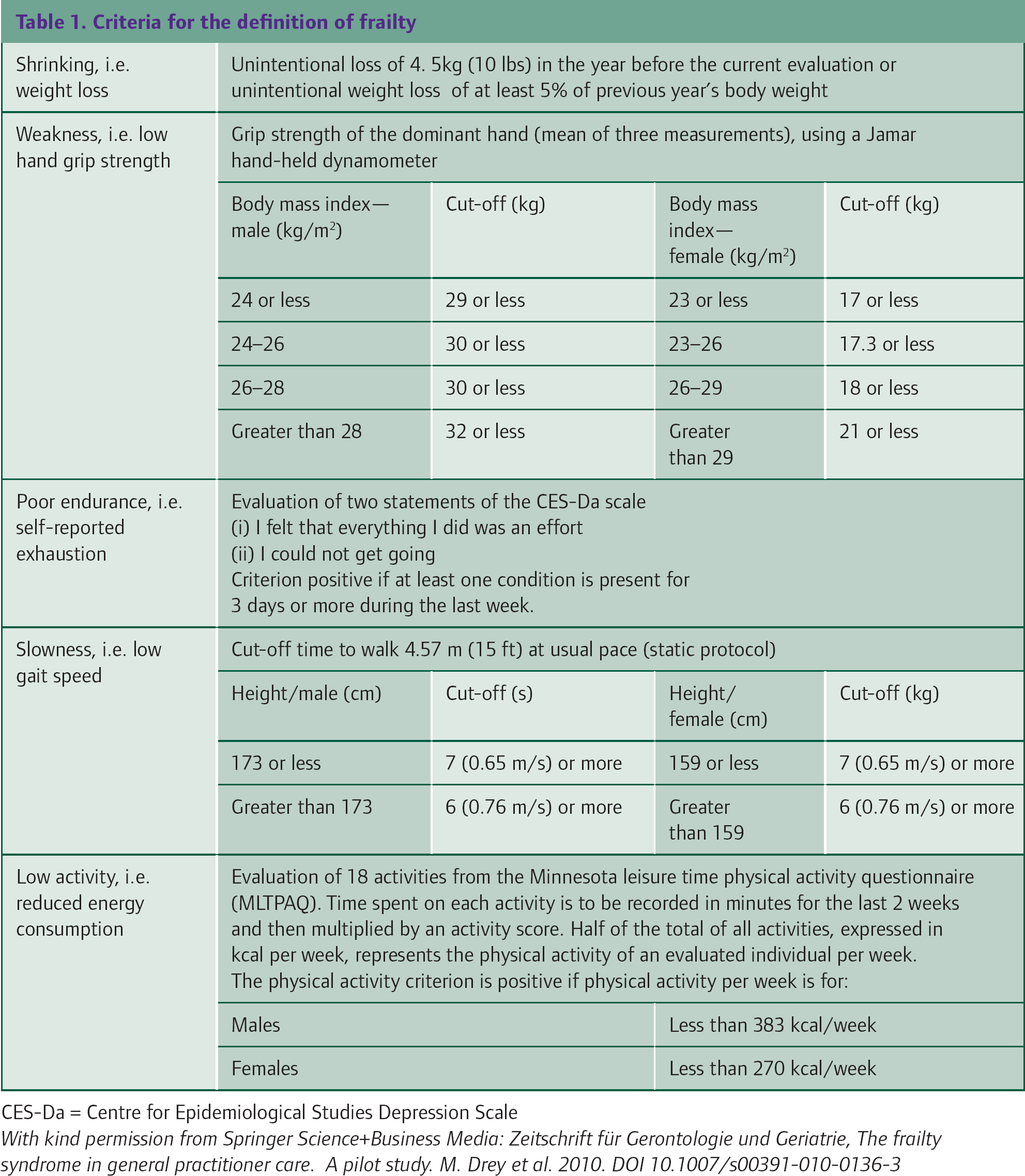
Fried et al. (2004) developed the most clinically accepted criteria for defining frailty (Table 1). These have been validated by Drey et al. (2011) as a 10 minute assessment useful in general practice for screening for frail patients to identify those at highest risk of deteriorating functionality and adverse health outcomes. This allows the implementation of preventative and therapeutic measures.
Healthy life expectancy
The distinction between life expectancy and healthy life expectancy is also important. Life expectancy estimates are calculated considering total mortality (and the causes), health data, biological, lifestyle and environmental factors. Life expectancy at birth has increased by approximately 30 years in the UK over the last 110 years—it was estimated at 77.5 years for males and 81.7 years for females between 2006 and 2008.
Within the UK, there is also significant geographical and socio-economic variation in life expectancy. Wanless (2004) showed that people living in Manchester had the lowest life expectancy in the UK. These differences exist due to increased rates of circulatory disease and cancer in lower socio-economic classes, hypothesized to be as a result of psychological, educational and lifestyle factors.
However, measurement of healthy life expectancy (the period of life which is spent in good health) is more informative given that most health and social care expenditure occurs in the last few years of life. Between 2005 and 2007, males in the UK could expect to live in ‘good’ or ‘fairly good’ health for 68.4 years at birth and 12.9 years at age 65 years; for females, the equivalent figures were 70.4 years and 14.5 years, respectively. Further improvements in both life expectancy and healthy life expectancy, and reductions in health disabilities, are expected in the future, but despite this, there will be an overall increase in the burden of disease.
Our population is ageing and, although many older people remain healthy for years after retirement, there is an overall increased burden of disease through frailty and chronic illness in this age group. Ultimately, as a society, we must consider how we are going to provide the health and social care needed to support the increasing numbers of elderly people with complex needs and also the rising public expectations about the care that will be available. This will put unprecedented pressures on our health and social care services, and economy as a whole, in the years to come.
Criteria for the definition of frailty
The effect of our ageing population
Older people are the main users of health and social care, with health care aimed at rehabilitation and the treatment of medical conditions and social care at providing practical support to enable people to lead independent lives.
The health service
People older than 65 years currently use 60% of hospital bed days (Oliver, 2009). With more older people, greater demands on services, and more expensive technology, the burden of health care is likely to increase.
Providing health care for older people relies on a multidisciplinary effort, often with the GP and primary care at the centre of the team, but liaising with secondary care and social care providers, and unpaid family carers as required. Interactions with older people may be particularly challenging because of difficulties in access, communication (for example due to hearing problems) and cognitive deficit.
The NSF for Older People (2001) states that the ageing of our population will be matched with increased physical dependence and disability as people survive longer with ongoing long-term conditions. It summarizes health care aims in treating older people in three key principles:
to reduce mortality, for example, the focus on stroke and cardiovascular disease prevention to reduce morbidity, especially in treating mental health and musculoskeletal diseases and managing polypharmacy to promote good health for as long as possible
Social care services
The government's Green Paper ‘Shaping the Future of Care Together’ (2009) estimates that by 2026, there will be 1.7 million more adults needing care. Many of these additional people will require care as a result of conditions like dementia. The Green Paper also identified that the rising expectations of our older population and demand for a high-quality system of care tailored to individual needs will put further strain and financial pressure on a system which already has major weaknesses. In addition, it highlighted that social care is currently provided by an apparent postcode lottery. There is poor use of resources and a focus on caring for those with the greatest needs rather than providing preventative care and rehabilitation.
Social care aims to assist patients in living the most independent life that they can and involves patient choice, maintaining dignity and high quality care. In ‘Shaping the Future of Care Together’ (2010), the Coalition Government set out its aim to have national consistency with local flexibility thus removing the postcode lottery but allowing individual choice within the system used.
There is a new emphasis on social care reform with a priority to provide more control to patients and their carers and to ease the burden of social care. The newly created Care Quality Commission (CQC) has said in its first annual report (2010) that we need joined up and person-centred care and must break down the barriers between health and social care services.
Solutions
The demographic shift in the ratio of retired to working people and multiple competing demands on health and social care services and local government make this a challenging time. Health and social care services need to work together providing rehabilitation and care with the aim of maintaining as much independence as possible for an ever-expanding and increasingly demanding consumer.
Intermediate care
‘Intermediate care—halfway home’ (DH, 2009) provides guidance on the use of intermediate care to meet the health and social care needs of patients outside the acute setting. It aims ‘to prevent unnecessary admission, expedite appropriate hospital discharge and avoid long-term admission to care homes’.
Brophy (2008) illustrates intermediate care as a continuum between health and social care (see Figure 2) ultimately to maintain independence. It hinges on effective multidisciplinary working and flexibility especially for older people who are particularly vulnerable during the transfer of care, e.g. when being discharged from hospital. There are a number of models of intermediate care, including rapid response teams to prevent avoidable admissions, acute care at home, residential rehabilitation, supported discharge and daily outpatient rehabilitation. Local arrangements vary enormously from area to area within the UK.
The continuum of intermediate care.
Increasingly, the GP plays a crucial role in intermediate care. GPs maintain clinical responsibility for most patients treated in the community and may have extended roles, for example leading rapid response teams.
Preventive medicine and health promotion
Ultimately, there must be a shift in the focus of our health and social care services with a priority on health promotion to maintain independence and good health in a cost-effective manner. The NSF for Older People (DH, 2001) emphasizes the benefits for both the individual and the society of health promotion to extend the life expectancy of older people. Examples of measures to delay the onset of disease and prevent untimely death include vaccination (primary prevention) and reducing cardiovascular risk, e.g. by reducing cholesterol through statins and weight reduction (secondary prevention) (Mangin et al., 2007).
Modifying risk factors for disease in older people has been shown to prevent disease, extend life, increase and maintain functional ability and give an improved sense of well-being. Budgen (2005) highlights that successful health promotion activities for older people should focus on positive activities and take a holistic approach accounting for the needs of the individual. For example, the DH's Prevention Package for Older People Resources are designed to promote health, well-being and independence for older people within their own homes and communities thus preventing or delaying the need for more expensive high intensity or institutional care. Clearly, this makes both health and economic sense.
Economic measures
In the current climate of economic constraint, providing high quality health and social care are not a cheap task and the cost-effective use of public funds is paramount. With fewer people working and paying taxes and more people post-retirement, the ratio of retired to working people is increasing. Therefore, there is a growing problem with the way in which services are funded.
To begin counteracting this deficit, the age at which a state pension can be claimed will increase in line with life expectancy. From 2010, the state pension age will rise from 60 to 65 years for women and is likely to rise from 65 to 66 years for men in 2016 and to 68 years by 2046. In addition, plans have been announced to remove the default retirement age entirely which would allow people to continue working beyond the state pension age should they wish to, thus increasing National Insurance contributions.
Attitudes to ageing and age discrimination
With increasing numbers of older people and the raising of the retirement age, the topic of age discrimination is at the forefront of public scrutiny. As such, GPs need to understand age discrimination and the legislative framework in which age discrimination is being addressed.
Attitudes to ageing
The main users of health care will continue to be older people, many of whom are frail with long-term conditions. Many people see the health services as inherently ageist. Common conditions of old age are often less well recognized, managed and resourced than those affecting younger people and symptoms may be investigated less frequently in this group. The Centre for Policy on Ageing (2010) briefing identified that ‘meeting individual needs should be based on their individual circumstances and not on arbitrary assumptions about their age’.
What is age discrimination?
Age discrimination has been distinguished from ageism (an attitude of mind) as discriminatory action, which is inherently measurable (for detailed definitions, see Box 1). Discrimination is rarely an active process but instead an inadvertent series of actions that lead to an older person being disadvantaged. The Equality Act (2010) identifies a number of different mechanisms of age discrimination:
Direct discrimination—in which a person is treated differently to another person because of a particular characteristic such as age
Discrimination by association or perception—in which individuals are treated differently, not because they have a particular characteristic, but because they are associated with someone else who has that characteristic
Indirect discrimination—in which there is a rule or policy that applies to everyone but that disadvantages a particular group
Harassment—violation of a person's dignity or creation of an intimidating, hostile or offensive environment for an individual because of a particular characteristic, in this case age
Victimization—occurs when a service provider treats an individual less favourably because the individual has made a complaint, or supported a claim made, for discrimination or harassment
In health and social care, age discrimination can happen in many ways, from refusal of specific treatment or services because of age or inappropriate comments about a persons' age to the inappropriate attribution of symptoms of disease to age resulting in under-treatment or the provision of inappropriate social care.
Key definitions related to age discrimination
Definitions taken from the Centre for Policy on Ageing briefings (January 2010).
The Equality Act 2010
Many elements of the Equality Act came into force on the 1 October 2010 as a single piece of legislation replacing the existing anti-discrimination laws, removing inconsistencies and making it easier for people to understand the Law and comply. It covers eight distinct groups relating to disability, gender reassignment, pregnancy and maternity, race, religion or belief, sex and sexual orientation.
The Act makes it unlawful to discriminate against any of these groups in any form. Thus, it has been agreed nationally by professional bodies and the Government that health, mental health and social care services should be organized and provided on the basis of need rather than age, thus ensuring that, for example, older people with disability do not fail to get the treatment or support required because they are older.
A further commitment to implement the ban on age discrimination was made by the Government in July 2010: ‘we are committed to promoting equality and will implement the ban on age discrimination in National Health Service (NHS) and social care to take effect from 2012’. In stamping out age discrimination, the legislative power of the Equality Act (2010) has been described as a ‘key bulwark against age discrimination’ (Oliver, 2009).
Age discrimination versus differentiation
Despite the necessity to ensure non-discriminatory service provision, it is undeniable that ageing does change disease processes and the prognostic benefits of treatments. These changes along with the need to use resources most effectively make age differentiation a key concept. Rather than discrimination where unjustifiable actions are made because of age, age differentiation is the treatment of people differently where there are justifiable reasons to do so, for example, in the provision of free flu vaccinations and bus passes for older people.
This extends into the work of the National Institute for Clinical Excellence (NICE), where overall cost-effectiveness of treatments must be assessed. It is in the analysis of quality-adjusted life years (QALYs—a measure of disease burden, looking both at the quality and at the quantity of life) that some feel NICE is treading a fine line between differentiation and discrimination.
There is concern that assessing the relative cost-effectiveness of treatments inherently disadvantages older people. In a population with significant co-morbidities, the successful treatment of one disease may be less effective in terms of overall health benefit but it may result in an improvement of quality of life. This is particularly relevant when considering diseases such as osteoarthritis and Alzheimer's disease which particularly affect older people and where treatment is focused at reducing morbidity and not mortality.
What this means for GPs
With an ageing population, GPs must consider the associated changes in the services that they will need to provide, how and with what intention patients are treated, and the possible legal ramifications of the Equality Act (2010).
The consultation
The RCGP published its 2010 manifesto ‘Leading the way—high quality care for all through general practice’, presenting strategies for coping with and adapting to increased demand. With older people making up a larger percentage of our population than ever before, the work of GPs together with the wider primary health care team, will increasingly involve the care of older people. The manifesto sets out an aim for
High quality GP care for all—GPs to have more time with their patients, GP-patient relationships to be maintained and improved … and better services for socially excluded groups (RCGP, 2010).
The RCGP clearly recognizes the difficulty in communicating with some older people and the increased complexities of their consultations, resulting in the need for increased consultation times. The statement also recognizes the importance of continuity of care and the need to actively address services for those in lower socio-economic classes to improve life expectancy in this group.
Wider determinants of health and health promotion
GPs are in a unique position to understand the wider determinants of health and how positively to change these. The challenge for individual GPs is to ensure that they stay up to date and in contact with other primary care providers and then use this knowledge to provide effective health promotion, continuing chronic disease management and palliative care.
In addition, GPs are likely to become more involved with intermediate care services, not only in maintaining clinical responsibility for their patients but also in working to prevent unnecessary hospital admissions.
Assessment of frailty
Drey et al. (2011) found strong correlations between frailty and mortality and adverse life outcomes. Assessment of frailty through use of Field et al's criteria (Table 1) in general practice has been shown to help GPs identify frail patients and thus provide earlier interventions to support them.
Implications of the Equality Act
The implications of the Equality Act (2010) inevitably mean that GPs must make reasonable adjustments to ensure that a person with a medical condition or disability is not disadvantaged. Reasonable adjustments depend on factors, such as the nature of the service offered, its size, the practicality of the adjustments and its cost. These adjustments may include the introduction of induction loops, ramps and accessible patient information in GP surgeries. GPs may well be advised to review their practice in terms of the Equality Act and ensure that they are compliant.
Conclusions
GPs are at the forefront of treating the older population. In order to do this effectively, GPs must be educated in the needs of older people, the discrimination they may face and make reasonable adjustments to their practice to accommodate elderly people. GPs will continue to be crucial in ensuring older people are valued and supported to live as healthy and independent a life as is possible.
Key points
The median age of the population is increasing with increased life expectancy and with this, there are significant health and social care and economic demands Intermediate care is crucial in supporting older people through transitions in their care Health promotion and maintaining independence are key priorities in dealing with the increased burden of disease The Equality Act has made age discrimination illegal Treating older people may take more time with increasingly complex needs and possibly challenging communication