
Abstract
Low back pain is an extremely common presentation in general practice. Most episodes are simple and self-limiting, but the ability to recognize serious underlying pathology is crucial for GPs. Symptoms of low back pain can be a major cause of physical and psychological disability, placing huge demands on society through the loss of working days and demands placed on medical resources.
The GP curriculum and low back pain
Royal College of General Practitioners (RCGP)
Recognize that musculoskeletal problems, including low back pain, are common, often chronic and potentially disabling
Identify a logical approach to the diagnosis of musculoskeletal problems, using history (including mechanism of injury), examination, appropriate investigations and timely referral
Develop an awareness of the roles of both the patient and the multidisciplinary team in the management of the condition
Appreciate the psychological aspects of musculoskeletal symptoms
Engage in effective communication of health information to promote best possible outcomes for those with musculoskeletal problems
Facts and figures
Back pain is one of the most common reasons for primary care visits in the UK: over a 12 month period, 7% of the adult population consults their GPs with back pain (McCormick et al., 1995). The lifetime prevalence of low back pain in industrialized countries is reported as over 70%, with peak prevalence between the ages of 35 and 55 years (COST B13 Working Group, 2004a). Back pain is the number one cause of long-term absence among manual workers and a common cause of short-term absence. Patients with musculoskeletal problems are recognized as the second largest group in the UK to receive incapacity benefits (Maniadaki and Gray, 2000; Department of Health, 2006).
Low back pain is defined as pain localized to the area below the costal margin and above the inferior gluteal folds, with or without leg pain. In the absence of known specific pathology (such as cauda equina syndrome, an inflammatory process, infection, tumour, osteoporosis, ankylosing spondylitis (AS), fracture or a radicular syndrome), the term non-specific low back pain is used. Fewer than 15% of patients with back patient have any specific underlying pathology (COST B13 Working Group, 2004b).
Symptoms which persist for 6–12 weeks are defined as acute episodes of low back pain, while symptoms that continue beyond 12 weeks are classified as chronic. Acute episodes are usually self-limiting. According to the literature, the recovery rate is 90% in 6 weeks. However, it has been suggested that these figures are falsely optimistic and that patients often continue to have symptoms in the community but opt not to consult their doctor again (Croft et al., 1998). Chronic back pain develops in 2–7% of people which can lead to severe disability and may be associated with psychosocial barriers to recovery (COST B13 Working Group, 2004b).
Aims of assessment
The key aims of back pain assessment are to recognize serious pathology, to relieve pain and to improve function. It is also important to recognize the level of disability caused by the back pain and to identify any potential barriers to recovery, while working to prevent recurrence and persistence of symptoms (COST B13 Working Group, 2004b).
For most patients, a thorough history accompanied by a brief clinical examination is sufficient, with a more targeted examination if any neurological signs or suggestive history are elicited. A suspicion of underlying pathology can then be confirmed by further investigation (COST B13 Working Group, 2004a).
A practical approach is to use a ‘diagnostic triage’ and divide back pain into three categories:
Serious spinal pathology
Nerve root/radicular pain
Non-specific low back pain
Figure 1 illustrates this approach.

Flow chart summarizing the diagnosis and management of low back pain. Adapted from Waddell et al. (1999).
History
A focused history and examination can identify patients at high risk for serious conditions. Ask the patient about any recent trauma, which may raise the possibility of a fracture, especially in patients with osteoporosis. Pain due to a fracture is sudden in onset, affected by movement and gradually improves over time. The pain associated with cancer or infection is often gradual and progressive with an unremitting quality, is worse at night and should be considered in patients who are systemically unwell or immunosuppressed. Patients with an underlying inflammatory condition often complain of generalized pain and early morning stiffness.
To identify those patients at increased risk of serious pathology, it is important to screen the history and presenting symptoms for the presence of ‘red flags’ (see Box 1). Red flags are often indicators of an underlying condition and are associated with a greater risk of serious pathology compared with patients without these features. Further investigation and referral should always be considered if one or more red flags are present. Remember that not all patients under 20 or over 55 years of age with back pain will have a specific condition, although these age groups are more at risk.
Red flags
Age of onset under 20 years or over 50 years
Bladder or bowel dysfunction
Progressive neurological deficit
Saddle anaesthesia
Thoracic pain
History of cancer, drug abuse, immunosuppression (including human immunodeficiency virus) and prolonged corticosteroid use
Fever
Unexplained weight loss
Structural deformity
Recent history of violent trauma (or minor trauma in patients with osteoporosis)
Constant, progressive non-mechanical pain unrelieved by postural modification
Accompanied by severe morning stiffness (suspicion of rheumatoid arthritis/AS)
Yellow flags
Yellow flags are psychosocial factors that appear to increase the risk of developing chronic pain and long-term disability. Current guidelines focus on identification of these potential barriers to rehabilitation, so that behaviour can be challenged in a positive way. Yellow flags are listed in Box 2.
At present, there is insufficient evidence available to recommend a specific psychosocial screening tool for use in daily practice when assessing back pain. The risk factors listed in Box 2 have been identified from a range of evidence-based guidelines [(NZGG, 2003), National Institute for Health and Clinical Excellence (NICE, 2008), National Health Service (NHS) Clinical Knowledge Summaries (CKS, 2009a)]. Screening people with chronic musculoskeletal pain for these ‘yellow flags’ can identify those with a poor prognosis for return to work. Yellow flags may also help to decide who should be offered low-, moderate- or high-intensity treatment (Haldorsen et al., 2002).
Examination
More than 85% of patients who present to primary care have back pain that cannot be reliably attributed to a specific spinal pathology or underlying disease. Identification of specific anatomical sources of musculoskeletal pain in these patients is difficult, due to conflicting schemes of classifications and the multitude of structures in the area that can potentially contribute to symptoms. Furthermore, there is no evidence that such anatomical labelling improves patient outcomes (Chou et al., 2007).
Yellow flags for developing chronic back pain
Inappropriate pain behaviours such as:
A belief that pain and activity are harmful leading to fear avoidance behaviours (i.e. fear of movement)
The belief that the pain should disappear entirely before attempting to return to work or normal activity
A passive attitude to rehabilitation
Sickness behaviour—such as extended rest
Work-related problems
prolonged periods off work
dissatisfaction at work
pessimistic expectations on ability to return to work
lack of support from co-workers/employers
Overprotective family, social withdrawal and lack of support
Emotional problems, such as negative mood, depression, anxiety or feeling under stress
Problems with claims for compensation or applications for social benefits
Inappropriate expectations of treatment, such as low expectations of active participation in treatment
A well performed and documented examination, with consistent findings from one visit to the next, is important. The following paragraphs review the important points to cover in the search for red flags.
General observation
Ensure that the patient is systemically well and there are no features suggestive of infection, underlying malignancy or inflammatory conditions. Check weight and temperature. Any suspicions should prompt examination of the relevant system (e.g. breast examination if bony metastases are suspected). Remember not to overlook other potential causes of back pain. Examine surrounding structures if indicated, including the abdomen, pelvis and pulses.
Gait can be observed as the patient walks into the room. Patients who are unable to walk on their toes, their heels and are unable to squat may have an underlying muscle weakness due to nerve root compression.
Regional back examination
Look for any structural deformity when examining the spine. Attempt to pinpoint the source of the patient's pain if possible. Vertebral point tenderness to palpation may be suggestive of a fracture or infection, especially if the patient is reluctant to tolerate any degree of lumbar motion testing. Soft tissue tenderness is a common and non-specific finding.
Neurological examination
A basic neurological examination can pick up obvious deficits. Search for signs of significant muscle wasting and rule out major motor weakness by testing power during knee extension, ankle eversion and foot dorsiflexion. Sensation and reflexes should be tested: any loss of tendon reflex suggests a high risk of permanent damage to a compressed nerve (CKS, 2009a).
Red flags should be actively sought. Any evidence in the history of incontinence or saddle anaesthesia (often present in cauda equina syndrome) should prompt a rectal examination to check for sensory loss or unexpected laxity of the anal sphincter. Disc herniation causing radiculopathy usually occurs at the L4–L5 or L5–S1 level. Figure 2 illustrates the clinical features of nerve root compression.
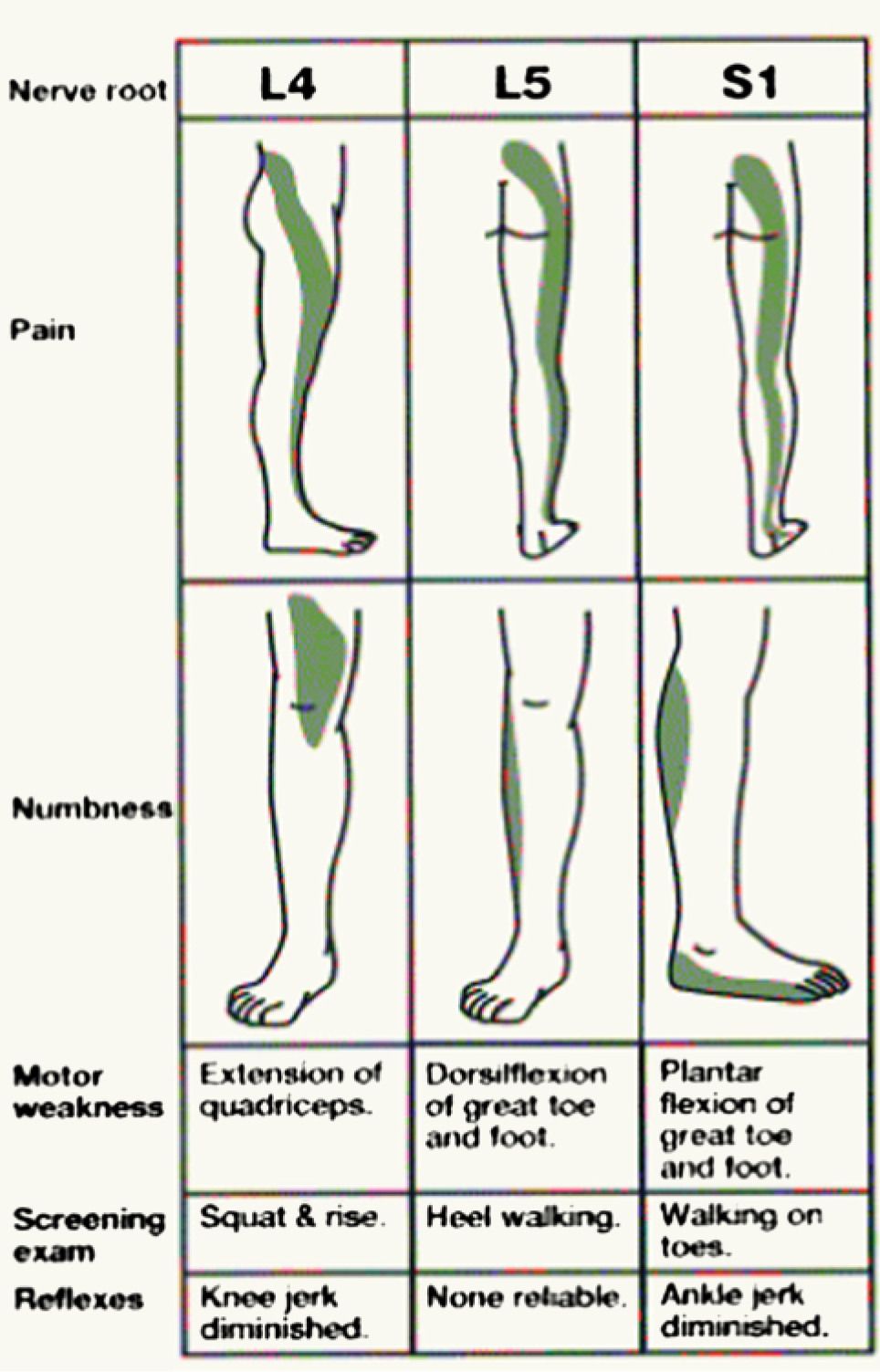
Nerve root compression.
The straight leg raising test can detect tension on the L5/S1 nerve root and testing often reproduces the pain by stretching the nerve roots irritated by a herniated disc. To perform the test, the patient should be supine and the leg raised, with the knee kept in extension. True sciatic tension should elicit complaints of pain before the hamstrings are stretched enough to move the pelvis. Dorsiflexion of the ankle at the limit of straight leg raising can also exacerbate the pain.
The reliability of testing reflexes can be affected by concurrent joint or muscle problems. The ankle jerk reflex tests mainly the S1 nerve root, while the knee jerk reflex tests mostly the L4 nerve root (neither tests the L5 nerve root). The Babinski or plantar response (up going toes in response to stroking the plantar aspect of the foot) can indicate upper motor neuron abnormalities, such as myelopathy or demyelinating disease.
Investigations
For those patients with red flags or a suspected underlying cause of their back pain (Box 3), investigations should be directed at finding the cause. Possible investigations include:
Full blood count (FBC), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) to help exclude inflammatory conditions and malignancy
Liver function tests (LFTs) and serum calcium levels to exclude hypercalcaemia, malignancy and bone disorders, such as Paget's disease
Urinalysis—nephrolithiasis may produce red cells in the urine; urinary hydroxyproline is elevated in Paget's disease of bone
Chest X-ray to help exclude lung cancer or tuberculosis
Causes of back pain
85% of patients presenting with back pain have no specific underlying cause. Specific causes of back pain include:
Secondary deposits in bone
Myeloma or (more rarely) other primary cancer
AS
Polymyalgia rheumatica
Coccydynia
Spondylosis—spinal osteoarthritis with osteophytes (bony overgrowths at the margins of vertebrae) and degenerative spinal facets and discs
Spondylolisthesis—forward displacement of one vertebra on its lower neighbour, often with a stress fracture in the pars interarticularis
Gross scoliosis or kyphosis
Osteoporosis with vertebral collapse
Osteomalacia
Paget's disease
Shingles (pain often occurs before the rash has developed) or post-herpetic neuralgia
Discitis
Osteomyelitis—bacterial or tuberculous
Epidural abscess
Thoracic spine
Hip
Abdomen, e.g. abdominal aortic aneurysm, peptic ulcer, upper gastrointestinal malignancy, pancreatic cancer
Kidney, e.g. renal stones
Ovary, e.g. ovarian cancer
Pelvis, e.g. endometriosis
Bladder
Endoscopy if a posterior peptic ulcer or upper gastrointestinal malignancy is of concern
Ultrasound to detect renal stones, pancreatic tumours or abdominal aortic aneurysm
In primary care, for patients with no red flags presenting with acute non-specific back pain, investigations in the first 4–6 weeks have not been shown to provide clinical benefit. In some areas, FBC, LFTs, serum calcium and ESR measurement are required before specialist referral for those with persistent symptoms.
Diagnostic imaging in non-specific low back pain
During the 1980s, radiography of the lumbar spine was the most commonly requested investigation for back pain in primary care, accounting for 5% of all radiographic investigations in the NHS. Such investigations occurred despite the fact that few findings altered clinical management (Kendrick et al., 2001). Although there is no evidence of a clinical benefit in terms of pain and disability from performing an X-ray, high levels of patient satisfaction have been reported after radiography (Kendrick et al., 2001; National Collaborating Centre for Primary Care/NICE, 2009). However, lumbar spine imaging does expose patients to a significant dose of radiation; a single lumbar film (0.7 mSv) is equivalent to around 35 chest X-rays (0.02 mSv) (Wall and Hart, 1997).
A magnetic resonance imaging (MRI) provides even greater rates of reassurance but is associated with greater costs and is often not directly accessible to GPs. Current NICE guidelines advise against lumbar spine X-ray for the management of non-specific low back pain, while MRI is only recommended in those patients who either have red flag symptoms or may have benefit from spinal surgery after completing a course of physical and psychological therapy (COST B13 Working Group, 2004b; National Collaborating Centre for Primary Care/NICE, 2009). More comprehensive guidance on imaging in low back pain can be found in a previous issue of InnovAiT (Evans, 2011).
Cauda equina syndrome
The cauda equina is formed by nerve roots caudal to the termination of the spinal cord (Figs. 3 and 4). Cauda equina syndrome is the term for any lesion that compresses these nerve roots. Characteristic symptoms are low back pain, unilateral or bilateral sciatica, saddle sensory disturbances, bladder and bowel dysfunction and variable lower limb neurological symptoms. Immediate referral for imaging and consideration of surgical decompression should be made if cauda equine syndrome is suspected, followed by treatment of the underlying cause.
Ankylosing spondylitis
AS is a chronic condition characterized by inflammation of the sacroiliac joints (sacroiliitis) causing pain in the lower back and buttocks. Progressive spinal fusion will ultimately result in a fixed kyphotic spine, which is prone to fracture following injury. In the early stages, onset is insidious and associated with fatigue and morning stiffness which improves with exercise. Diagnosis is based on detection of inflammation of the sacroiliac joints. Early diagnosis requires a high index of suspicion. Raised inflammatory markers may support the diagnosis but inflammatory markers may be within normal limits. A referral to a rheumatologist should be arranged if the condition is suspected for long-term advice and management.
Back pain in cancer patients
Back pain in a cancer patient requires urgent assessment. Spinal cord compression is a medical emergency and often occurs in cancers with a tendency to metastasize to bone, such as prostate, breast and kidney cancers. Symptoms suggestive of spinal metastases include:
Pain in the thoracic or cervical spine
Progressive, severe unremitting lumbar spinal pain
Pain aggravated by straining, with localized spinal tenderness
Nocturnal pain preventing sleep
Presence of neurological symptoms
A MRI scan should be performed within 24 hours if cord compression is suspected and within 1 week in patients with symptoms suggestive of spinal metastases. Referral should be made for definitive treatment, which may vary depending on the condition and preferences of the patient (NICE, 2008).
Sciatica
Radicular pain, nerve root pain and sciatica are all interchangeable names for the symptoms of pain, tingling and numbness that arise as a result of nerve root compression or irritation in the lumbosacral spine. Symptoms are felt along the distribution of the nerve root and typically across the back, buttocks, thigh, outer calf and often to the foot and toes (Koes et al., 2007). Nerve root compression is caused by a herniated disc in 90% of cases, although rarer causes to consider include spinal stenosis (narrowing of the spinal canal), spondylolisthesis (anterior displacement of a vertebra), infection, injury or a tumour arising within the spine (Koes et al., 2007). Treatment is, at least initially, as for non-specific back pain.
Management of non-specific back pain
An active approach is the best treatment for low back pain. Management should focus on reassuring the patient that low back pain is not usually a serious condition and that a full recovery is expected. Patients should be encouraged to keep moving and return to work and normal activities as soon as possible. Sufficient analgesia should be provided alongside advice and written information regarding the diagnosis. Diagnosis should also be kept under review (National Collaborating Centre for Primary Care/NICE, 2009). Figure 3 provides a useful flow chart to direct management.

Flow chart for the primary care management of non-specific back pain.
The presence of lumbar radiculopathy (sciatica) is initially treated in the same way as non-specific low back pain unless there is a progressive persistent neurological deficit or red flags, in which case these patients warrant an urgent referral. If symptoms of sciatica remain disabling after 8 weeks of treatment, then further referral is recommended (CKS, 2009b).
Analgesia
Drug treatments can be used to manage pain to allow people to keep as active as possible. Regular paracetamol is the first-line treatment. If this is insufficient, then non-steroidal anti-inflammatory drugs (NSAIDs) and/or weak opioids may be offered, taking into account individual risk of side effects and patient preferences. When prescribing NSAIDs, co-prescribing a proton pump inhibitor (PPI) should be considered for people over the age of 45 years or with risk factors for peptic ulcerations, such as co-prescription of steroids, selective serotonin reuptake inhibitors and iron or aspirin.
Weak opioids such as codeine and dihydrocodeine carry a risk of dependence. A laxative is sometimes required to counteract their constipating effects so that straining does not exacerbate the back pain symptoms. A strong opioid (such as standard release morphine) is rarely required, but if it is to be used, then it should be prescribed for short periods, alongside a laxative and an antiemetic, with a plan to step down to a weak opioid in due course. Prolonged use of strong opioids should be managed in a pain clinic or via other specialist services.
The use of benzodiazepines is controversial due to the risks of adverse effects and the danger of dependence. International guidelines differ in their viewpoint, with many advising against their use due to the risk of dependency. The current NICE guidelines make no recommendations. UK guidelines published by the RCGP (Waddell et al., 1999) recommend the consideration of muscle relaxants if other forms of analgesia have been ineffective. If they are prescribed, it should only be for a short course (2–5 days) during an acute episode. There is evidence that muscle relaxants relieve the muscle spasm associated with low back pain. Diazepam is most commonly used for this indication since it is longer acting and less likely to result in withdrawal symptoms than other benzodiazepines (COST B13 Working Group, 2004a; CKS, 2009a).
For chronic pain, not responding to other treatment, tricyclic antidepressants can be considered. They should be started at a low dose and increased up to the maximum antidepressant dosage until therapeutic effect is obtained or until unacceptable side effects prevent a further increase (National Collaborating Centre for Primary Care/NICE, 2009).
Information and advice
Providing adequate information to encourage a positive approach and to encourage self-management is essential. There are several sources of excellent written information for patients with back pain available online at Patient UK (see further reading). Key messages are that recovery is helped by keeping active and that pain control is provided as a temporary measure to assist with this process. Acknowledging that non-specific back pain has a real physical cause can help patients to manage their symptoms. Explaining that it is a mechanical problem and rarely a disease in itself can offer reassurance that symptoms are not being disregarded, which in turn may encourage a positive attitude towards coping with the problem. Progress should be recognized and reinforced.
Physical activity
Since the 19th century, bed rest was considered to be the standard treatment for back pain. There is now strong evidence to suggest that bed rest is associated with increased pain intensity, increased disability and more days off from work (Wilkes, 2000). During an acute episode of back pain, normal activity should be resumed as soon as possible. Normal movements are likely to precipitate pain so should be reintroduced slowly, with patients encouraged to do a little more every day. Care should be taken with lifting and twisting activities. A return to work should be encouraged.
For patients identified to have yellow flag symptoms, at risk of developing chronic pain, it may be beneficial to intervene early by offering a structured exercise programme with up to eight sessions over a 3 month period. These sessions can be undertaken as part of a group or on an individual basis and incorporate aerobic activity, muscle strengthening exercises and instructions on movement control, stretching and posture improvement (National Collaborating Centre for Primary Care/NICE, 2009).
Further treatment options
Manual therapy is a collective term which includes spinal manipulation, spinal mobilization and massage. These are procedures which can be carried out by chiropractors and osteopaths, as well as by doctors and physiotherapists who have undertaken specialist training in manipulation. NICE recommends consideration of manual therapy over a 3 month period for those patients who have not shown satisfactory improvement with first-line therapies.
Injection of therapeutic substances into the back is not advised in the treatment of low back pain. However, a 12 week course of acupuncture can be considered if available locally (National Collaborating Centre for Primary Care/NICE, 2009).
If the above options are unsuccessful and patients continue to have significant psychological distress and high levels of disability, then referral for a combined physical and psychological treatment programme should be considered, which comprises around 100 hours of cognitive behavioural therapy and exercise over a period of 8 weeks (National Collaborating Centre for Primary Care/NICE, 2009).
Surgery
Spinal fusion surgery is a technique originally designed to treat spinal instability. Surgical intervention for non-specific low back pain should only be considered after completing an optimal package of care, which included a structured exercise program with combined physical and psychological therapy. If the patient still has severe symptoms after this and would consider surgery, then referral for an opinion on spinal fusion through a specialist spinal surgical service is appropriate (National Collaborating Centre for Primary Care/NICE, 2009). Referral for consideration of other procedures such as intradiscal electrothermal therapy, percutaneous intradiscal radiofrequency thermocoagulation or radiofrequency facet joint denervation is not recommended (National Collaborating Centre for Primary Care/NICE, 2009).
Prevention of non-specific back pain
Some of the key recommendations in the prevention of back pain are summarized below and are readily accessible to patients in leaflet form from Patient UK.
Exercise—regular activity with stretching before and after helps to maintain the strength of lower back muscles, which can prevent disc degeneration
Lifting—correct techniques should be used for lifting. Most manual jobs will incorporate an induction to reinforce correct techniques
Seating—ensure seating at work or when driving for prolonged periods is comfortable and take regular breaks to stretch
Weight—excessive weight puts further strain upon the back. Encourage weight reduction to reduce this strain
Smoking—smoking has been associated with chronic back pain, so smoking cessation should be promoted
Posture—good posture can prevent back pain
Mattress—sleeping on a mattress that supports the natural curves of the spine can help avoid back pain
Key points
Evidence of red flags in the history should prompt immediate investigation
Be mindful of yellow flags which may promote ‘illness behaviour’
Encourage positive lifestyle changes (exercise, smoking cessation and weight loss)
Promote self-management using appropriate analgesia, physical activity and persistence with normal activities as far as possible
Do not offer X-ray of the lumbar spine for the management of non-specific low back pain
Review patient progress and utilize resources such as an exercise programme, manual therapy or acupuncture