
Abstract
Testicular and scrotal pain are common presenting complaints in the GP surgery. Often, men present after acute onset of pain, but more commonly male patients attend after a gradual progression of more vague testicular symptoms or when discomfort begins to impact upon normal activities of daily living. Testicular symptoms can be a cause of great anxiety among patients, particularly as men (most notably younger men) are often embarrassed or reluctant to consult, which GPs need to be sensitive to. This article discusses some of the common and important testicular pathologies and emphasizes how a structured approach to the history and examination helps in making a clinical diagnosis.
The GP curriculum and testicular pain
Have knowledge of the acute management of testicular torsion Have knowledge of the symptoms of testicular lumps and testicular pain Have knowledge of the common/important conditions of testicular cancer, varicocele, haematocele, epididymitis, epididymo-orchitis and cryptorchidism Intervene urgently when patients present with a testicular emergency Be competent in undertaking testicular examination Demonstrate a non-judgemental, caring and professional consulting style to minimize embarrassment of male patients Describe the particular difficulties adolescent males have when accessing primary care services
In addition,
Testicular structure and anatomy
An understanding of the anatomy of the testicle and associated structures is vital to making an accurate diagnosis and for explaining to patients the causes of their symptoms. It is important to understand that the testicles descend through the inguinal canal during foetal development and should be fully descended by the first year of life. Figure 1 shows the structure of a normal testicle and associated anatomy.

Structure of testis.: Akbar, S. A., Sayyed, T. A., Jafri, S. Z. H. et al. Multimodality imaging of paratesticular neoplasms and their rare mimics. Radiographics 2003) 23: p. 1461–76. Reprinted with permission from the Radiological Society of North America.
The spermatic cord is the cord-like structure that encloses the testicular and associated neurovascular structures and descends from the abdomen to the scrotum. It is composed of three layers of fascia, which are continuous with the abdominal muscles and facia. It contains arteries, the vas deferens, the venous pampiniform plexus, cremasteric and testicular nerves, lymphatic vessels and the tunica vaginalis (the serous ‘covering’ of the testis, derived from peritoneum). Due to the neurovascular origins, pain originating from testicular pathology can be perceived focally in the testicle, as a vague ache or heaviness inguino-pubically or sometimes as a pain in the T10 distribution.
Structured approach to assessment
Having a structured approach to the history and examination of the testicle and scrotum is essential to making a diagnosis as the vast majority of testicular complaints can be diagnosed clinically from the history and examination alone.
History
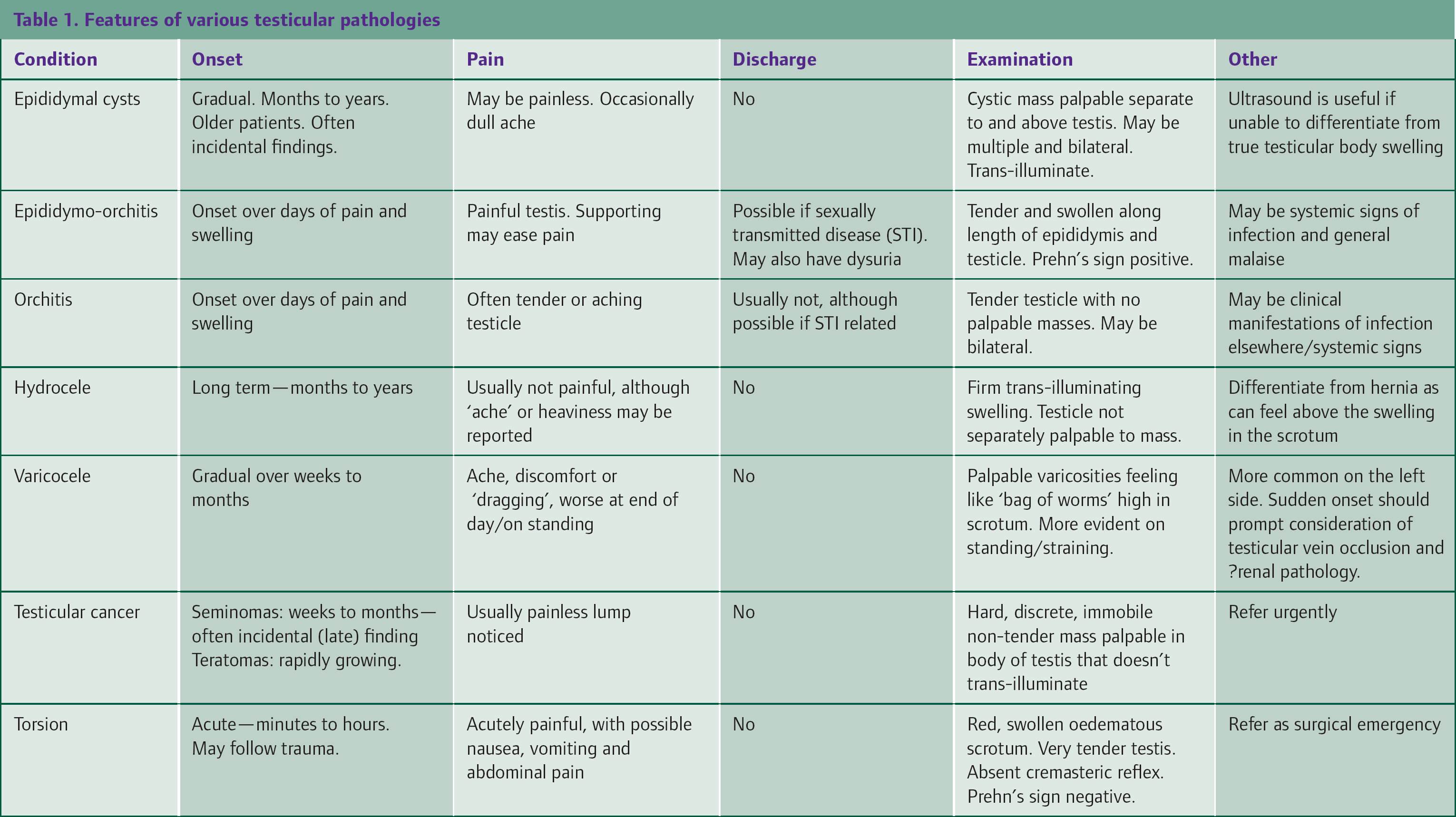
As Table 1 summarizes, the duration of symptoms and their progression over time are very useful in determining the cause of testicular pain and related symptoms. An abrupt onset of testicular pain over minutes or hours (particularly following trauma) suggests a hyperacute pathology, such as torsion, and requires a similarly speedy response from the GP. An acute onset over days suggests an infective pathology, such as an epididymo-orchitis. A gradual onset of testicular symptoms over weeks to months suggests a more chronic pathology, such as a varicocele or hydrocele.
Features of various testicular pathologies
It is important for the GP to elicit from the history whether there has been any trauma, the nature of the pain or swelling and whether the patient is sexually active. A more detailed sexual history is indicated if there is any suspicion of an infective cause, such as an epididymo-orchitis. It is also important to ascertain how the symptoms are affecting daily activities, participation in sport and sexual function: whether intervention is considered in the more ‘benign’ conditions will be guided by these factors.
Examination
As with any intimate examination, testicular examination (or the fear of it) can be the source of much anxiety among patients, especially if the patient is young or the person doing the examination is of the opposite sex. Some good practice points for the GP include a careful explanation of why the examination is necessary and what will be involved, along with ensuring adequate privacy and the offer of a chaperone. A warm examination room, as well as warm hands, will ensure that the examination is as informative as possible. Informed consent should be sought and documented.
Careful initial inspection of the scrotal skin and groin will reveal any dermatological causes of pain and may be helpful in the diagnosis. While it is normal for the testicles to rest at different levels and be slightly differently sized, any gross asymmetry caused by hemi-scrotal swelling, oedema or erythema should be evident. The presence of the ‘bell-clapper’ testis, which rests high and slightly more horizontal in the scrotum, is associated with increased risk of torsion.
The presence of both testes in the scrotum should be confirmed. In younger boys with an active cremasteric reflex—the so-called ‘retractile testicle’—it may be necessary to ‘milk’ the testicle down into the scrotum. If it is not possible to palpate the testicle, it should be assumed undescended. While local guidelines vary slightly, a testicle is exceptionally unlikely to spontaneously descend beyond 1 year of age, and so referral for surgical fixation at this point is usually recommended to minimize the chance of future subfertility and malignancy.
Each testicle should then be separately palpated gently between thumb and forefinger, paying attention to the structures shown in Fig. 1. The location of any tender points or masses should be noted, and in particular, whether one can feel ‘above’ the mass and feel a separate distinct testicle. If any masses are identified, a pen torch or other suitable light source can be used to determine trans-illuminance. The following sections of this article detail how the common testicular pathologies usually manifest.
Testicular trauma
Men of all ages can present to the GP following direct testicular or scrotal trauma. However, it is most commonly seen in adolescents and younger men and is commonly related to sporting injuries or physical assaults. Before assessment of any testicular or scrotal injury, it is important to ascertain the mechanism as this will not only guide examination but may also highlight important social issues, including child protection or vulnerable adult concerns.
The European Association of Urology (2009) describes a spectrum of scrotal and testicular pathology secondary to trauma. At the minor end of the spectrum is simple scrotal contusion or superficial subcutaneous haematoma not involving the testicle. Such injuries can usually be managed conservatively in primary care, with adequate simple analgesia and advice about wearing supportive underwear.
More serious trauma, notably where any testicular haematocele is clinically evident, or any degree of focal testicular tenderness is clinically apparent should raise the suspicion of testicular injury. Damage may range from laceration of the tunica albuginea right up to complete testicular avulsion and parenchymal loss. These injuries warrant emergency referral for urological opinion and surgical exploration. The same is true for any penetrating scrotal trauma as surgical exploration is mandatory to ensure testicular preservation.
Often, following an acute recent trauma, examination of the testicles can be difficult due to local swelling or discomfort. As testicular torsion (described below) is a recognized complication of injury, GPs should have a low threshold for referral for same-day surgical exploration of injuries where there is any clinical doubt as the consequences of missing testicular torsion are life-changing.
Testicular torsion
A testicular torsion is a true urological emergency. It occurs when the body of the testis twists around on the spermatic cord and occludes the blood supply. Most common in 10- to 25-year-olds, it can occur in younger children and older adults and may follow very negligible testicular trauma or occur spontaneously. Either way symptoms are fairly rapidly progressive, usually developing over the course of a couple of hours. The may be a history of previous more minor self-limiting episodes, due to subtotal torsion events.
The clinical history is one of a discomfort developing acutely to often quite severe testicular pain. There may be vomiting and associated abdominal pain as a result of the anatomical origins of testicular innervations. The scrotum may become erythematous, swollen and oedematous, and the testicle is often lying higher and more horizontally than normal and may be exquisitely tender to palpate. The cremasteric reflex (where the testicle will usually retract slightly up towards the abdomen when the inner thigh is brushed) may be absent. Supportive elevation of the testicle does not relieve the pain (a so-called negative Prehn's sign), but none of these features should be relied upon to make the diagnosis as the absence of clinical signs does not exclude the diagnosis of torsion. As the clinical course in younger children can be particularly vague, any suspicion of torsion should be referred as a urological emergency for surgical exploration.
If the testicle is salvageable surgically, the contralateral side is also usually surgically fixed to the dartos muscle to prevent torsion subsequently in that testicle. Figure 2 shows the appearance of a testicular torsion that was not operated on in time to preserve function.

Cute testicular torsion resulting in necrosis.: Aso, C., Enríquez, G., Fité, M. et al. Gray-scale and color doppler sonography of scrotal disorders in children: an update. Radiographics (2005) 25: p. 1197–1214. Reprinted with permission from the Radiological Society of North America.
Torsion of the testicular appendage
Occasionally, torsion of various vestigial remnants of the embryological origins of the testis can occur. These are most common in 6- to 12-year-olds and are most often of the testicular appendage (or hydatid of Morgagni), which lies at the apex of the testis. In approximately a fifth of cases, there is a characteristic tender blue-tinged area seen at the top of the testicle (blue dot sign), but due to difficulty in discriminating clinically from a true testicular torsion, the GP should also refer to urology as an emergency for exploration.
Epididymal cysts
Epididymal cysts (shown in Fig. 3) are the origin of much anxiety, most commonly occurring in the fourth decade onwards. They are often completely asymptomatic and are usually noticed incidentally on self-examination or by partners. Sometimes they may be the cause of some general testicular discomfort, particularly if large, which may be most noticeable during sexual activity or other physical exertion.

Epididymal cyst
Examination in cases of epididymal cysts reveals one or more trans-illuminating fluctuant structures arising from the epididymis, which is separately palpable from the testis. It is possible to ‘get above’ the structure on palpation. If there is clinical doubt, an ultrasound scan may be of use to differentiate an epididymal cyst from a true testicular mass.
Unless interfering with normal function or significantly symptomatic, a patient can be reassured about the aetiology of these benign structures and no action is necessary. Aspiration often results in recurrence, and surgical removal can potentially cause more problems than a conservative strategy. Often, reassurance of the nature of the lump is all that is needed for most patients.
A variant of the epididymal cyst is a spermatocele, the only difference being the ‘fluid’ in the cyst is more milky and contains spermatozoa. These can similarly be managed conservatively if asymptomatic, else referred to urology for surgical excision.
Orchitis
The most frequent cause of an acute orchitis (acute testicular inflammation) is viral, but a chronic orchitis can follow trauma or testicular surgery. The most common causative agents are mumps virus and infectious mononucleosis, although coxsackie virus and rubella can be responsible. Approximately a fifth of post-pubescent males who contract mumps will develop orchitis, which can be bilateral. Testicular atrophy and even infertility are possible complications. The Health Protection Agency has issued a number of warnings over the last couple of years about an alarming rise in the number of mumps cases in adolescents and adults; therefore, it is important for the GP to be aware that an orchitis may be the only presenting feature of this condition.
In early orchitis, the testicle becomes tender, with sparing of the epididymis, but as the condition progresses, the whole scrotum may become inflamed and oedematous. Other features associated with systemic viral infection may be present, and serology may be helpful to confirm the underlying viral cause. Consideration must be given to public health notification if appropriate. Treatment is conservative, with analgesia and advice about testicular/scrotal support and rest as the course is self-limiting. Ongoing chronic orchitis should be referred to a urologist for further investigation to exclude a granulomatous process.
Epididymitis and epididymo-orchitis
Infection of the epididymis can lead to painful inflammation, which if it spreads to involve the testicle is termed epididymo-orchitis. Men with this condition often complain of a tender scrotal swelling, which may occasionally be bilateral, worsening over a couple of days. Examination reveals a tender and often thickened epididymis that is separately palpable from the testis. If there are also features of orchitis, it may not be possible to feel the epididymis separately from the testis.
The most likely organism (and therefore treatment) will depend upon risk factors identified in the history. The presence of any urethral discharge is important as in men under the age of 35 years, it is most commonly caused by Chlamydia trachomatis and should therefore prompt a more detailed sexual history. If it is not possible to screen for Chlamydia and gonorrhoea at the time of diagnosis, consideration should be given for referring the man to a local sexual health service for investigation and treatment. In men over the age of 35 years, the most common causative organism is Escherichia coli, and a midstream urine culture may be useful.
Treatment of this condition is with adequate analgesia, rest, scrotal supports and antibiotics, the choice of which will depend on age and most likely causative agent as per a detailed history. In men under the age of 35 years, treatment should cover Chlamydia pending microbiology results and as such doxycycline 100 mg twice daily for 14 days or ofloxacin 200 mg twice daily for 14 days are the recommended choices if gonorrhoea is excluded [British Association of Sexual Health and HIV (BASHH), 2010]. If there is a specifically high suspicion of gonorrhoea, GPs should liaise with the local sexual health service regarding local sensitivities and antibiotic treatment. In men aged over 35 years in whom there is a low risk for sexually transmitted infection (STI), treatment with trimethoprim or ofloxacin is recommended.
Symptoms can persist for several weeks, and extending the therapy for up to a month is recommended for incomplete resolution. Contact tracing and treating are important if a STI is identified. Occasionally, the pain is so severe that an acute admission under the urologists is needed for analgesia and intravenous antibiotics. Ultrasound imaging can be helpful to exclude an underlying testicular malignancy in young men with epididymo-orchitis, especially if adequate palpation is difficult.
It is worth noting that a more chronic form of epididymitis is also occasionally encountered. This can be caused by microbial agents such as Mycobacterium tuberculosis or syphilis or secondary to some medications (e.g. amiodarone). Such cases are best managed by specialists; therefore, referral to urology or sexual health is indicated.
Varicocele
A varicocele is a varicosity of the pampiniform plexus that provides venous drainage of the cord and scrotum. These are very common, affecting upwards of 8% of men to some degree, and can occur on either side. However, more than 90% occur on the left, due to the left testicular vein draining directly into the left renal vein. A patient may complain of a dull ache or dragging sensation in the scrotum or groin region that is worse towards the end of the day or on standing and straining. The onset of a swelling and discomfort is usually long term over many months. The abrupt appearance of a significant varicocele on the left may herald an acute renal vein abnormality, and the GP should be aware of a potential renal malignancy and arrange appropriate imaging.
On examination, a swelling in the upper scrotum that is distinct from the testis and appears to be emerging from the groin is found. It is characteristically worse on standing and straining and may be absent on laying flat. Traditionally, the feel of a varicocele has been described as a ‘bag of worms’, referring to the firm jelly-like feeling of multiple adjacent varicosities.
Management is usually conservative unless significantly symptomatic. There is a suggested link between varicoceles and reduced fertility, which may be due to increased testicular temperature that the pathology results in. If the varicocele is significantly troublesome, the GP should refer to urology. Surgical options include open or laparoscopic direct ligation, or embolization of the testicular vein, which is being increasingly undertaken by interventional radiologists. However, it is important to counsel patients that there is no evidence that excising the varicocele improves fertility. If symptoms are only mild, then advice and reassurance in primary care may be all that is needed.
Hydrocele
A hydrocele is a collection of fluid between the tunica vaginalis and the tunica albuginea. The majority occur spontaneously and gradually, but it is important to be aware that a sudden occurrence in an adult may herald the presence of another pathology (infective or malignant) in the testis underneath.
Some (even massive) hydroceles may be asymptomatic, but often, there is a general discomfort or ache in the testis. As they can become quite large, functional or cosmetic concerns may be a consideration for some patients rather than pain. The scrotum swells asymmetrically, but the overlying skin is normal (Fig. 4).

Testicular hydrocele Dr P. Marazzi/SPL
A testicular hydrocele is distinguishable clinically as a smooth, trans-illuminating fluctuant mass. The testis is not palpable separately as it is entirely inside the hydrocele. Due to the possibility of heralding another more sinister pathology, advice is to arrange prompt ultrasound imaging of first presentation hydroceles in adults. Once the diagnosis is confirmed, management can be conservative if the patient is reassured and not particularly symptomatic. Surgical options include aspiration or open surgery. The recurrence rate is significant.
Infantile hydroceles are usually congenital and secondary to a patent processus vaginalis. They often resolve spontaneously in the first year of life, but if not should be referred for surgical correction to urology or paediatric surgery according to local procedure.
Testicular tumours
Testicular malignancy, although thankfully fairly rare overall, is the most common malignancy in men aged 18–35 years. Although not usually presenting with testicular pain, it is included in this article as its early recognition and treatment are vital to maximize survival as it affects the demographic group statistically least likely to have contact with primary care health services. As a result of recent media campaigns and high-profile celebrities and sports personalities promoting awareness of the condition, GPs might expect to see an increase in younger men presenting for an opinion on testicular and scrotal masses.
Table 2 summarizes the key features of the two principal types of malignant testicular cancer: seminomas and teratomas. Benign testicular tumours (Sertoli cell and Leydig cell adenomas) account for fewer than 2% of testicular tumours. All tumours commonly present as a painless lump found incidentally on self-examination or by partners, but there may be some discomfort or slight tenderness. The lumps are usually firm, non-tender and not palpable separately from the testis and do not trans-illuminate. Occasionally, hydrocele occurrence can be secondary to a testicular tumour, so treat any new onset of a hydrocele in a younger man with suspicion and consider prompt imaging. Any suspicious testicular lump warrants urgent referral to urology to exclude malignancy. Occasionally, these tumours unfortunately present with symptoms of spinal or lung metastasis.
Characteristics of testicular malignancies

Scrotal skin
A common presentation to primary care concerns scrotal swellings, some of which can be painful. Often, the patient may indicate the pain as being testicular when the pathology is actually dermatological in origin. Superficial skin infections, including Staphylococcus aureus furuncles and abscesses are common and can range from minor self-resolving infections to those requiring formal incision and drainage. A course of oral antibiotic treatment may be useful for more significant cases. In recurrent or advanced cases, it is important to consider hidradenitis suppurativa in the differential as approximately half of male sufferers will have groin or scrotal involvement at the site of apocrine sweat glands. Referral to dermatology may be helpful for the long-term management of this relapsing incurable condition.
Fournier's gangrene (Fig. 5) is a rare but potentially devastating spreading necrotizing cellulitis that commonly originates in the groin or scrotal skin. Most often, it is caused by a combination of anaerobic and aerobic bacteria and occurs more frequently in middle-aged and older patients or those with risk factors for skin infections (diabetes, obesity, immunocompromise, etc); however, cases in children are not unheard of. It often commences as a non-specific scrotal or groin pain, which can progress alarmingly rapidly to frank cellulitis with systemic features. Often, clinical examination underestimates the extent of the necrosis, but spreading erythema and oedema, anaerobic odour and crepitis may all be present. A portal of entry in the form of a minor wound or abrasion is often identified on examination. Even treated mortality is as high as 40%. Rapid emergency admission for parenteral antibiotics and surgical debridement is required if there is any clinical suspicion of an evolving Fournier's gangrene.

Fournier's gangrene.: Reprinted by permission from Macmillan Publishers Ltd: Nature Reviews Urology (2006) 3: p. 54–7
It is also important for GPs to consider STIs as potential causes for localized scrotal pain and lesions. Herpes simplex virus characteristically presents as a painful shallow ulcer, and a painless ulceration should prompt consideration of a syphilitic chancre. The treatment of these conditions is covered in InnovAiT articles ‘The presentation and management of genital herpes’ (Nicum and Mahida, 2010) and ‘conditions affecting the penis’ (Nash, 2010).
Hernias
A scrotal swelling that it is not possible to palpate above should lead the GP to consider an inguinal hernia. The detailed discussion of hernias is beyond the scope of this article and is covered in detail in the previous InnovAit article ‘Hernias’ (Stubbs and Hyder, 2009).
Key points
GPs must be aware of the perceived embarrassing nature of testicular symptoms and the associated anxiety regarding testicular swellings and respond sensitively to men presenting with testicular problems The majority of diagnoses can be reached by careful history taking and clinical examination and often reassurance is all that is required Clinical suspicion of a torsion or acute testicular injury following trauma requires referral for surgical exploration as an emergency GPs should treat any true testicular mass with suspicion and refer urgently to exclude malignancy Ultrasound is a useful tool when the clinical diagnosis is uncertain, but its use should not delay urgent referral where suspicion is high Epididymo-orchitis in younger men is most commonly the result of STI