
Abstract
Problem drinking is a significant public health concern in the UK and is receiving growing media attention. While the headlines often focus on the harm of teenage ‘binge drinking’, the more subtle and far reaching psychosocial implications of chronic alcohol misuse can often be overlooked. GPs are well placed to recognize and manage the diverse health complications of alcohol misuse. Evidence suggests that even minimal brief interventions can have a significant positive impact on individuals who drink to excess. This article discusses some of the medical and psychosocial complications of both acute and chronic alcohol use that GPs should be aware of in order to assess and reduce the harm caused by alcohol within the primary care setting.
The GP curriculum and alcohol use
Recognize the physical, psychological and social manifestations of alcohol problems
Have an understanding of the health and social burden of excess alcohol consumption
Have a knowledge of the screening tools which can be used to identify excess alcohol use
Understand the difference that health professionals can make by providing brief interventions for alcohol use
Understand alcohol-related emergencies, such as fits, delirium and psychosis
Have an understanding of the term ‘harm reduction’
The scale of the alcohol problem
It is estimated that in the UK, 24% of adults drink in a harmful or hazardous way and 5.9 million people engage in binge drinking. Of increasing concern is the number of teenagers and young people who use alcohol harmfully. At peak times on Friday and Saturday nights, more than70% of hospital emergency department attendances are alcohol related and in excess of 30 000 acute admissions to hospital take place annually as a direct consequence of chronic alcohol-related diseases. Excess alcohol use can affect every organ system in the body and can be the source of significant physical disability, mental health problems and psychosocial harm and may have implications beyond the individual patient. The GP must therefore be aware of the acute and chronic implications of alcohol misuse and be equipped to manage them.
Assessing problem drinking
While some patients may present to primary care either with evidence of the consequences of harmful alcohol use or requesting support to change their relationship with alcohol, many opportunities for alcohol-related health promotion will be missed if opportunistic screening and brief interventions are not offered. All patients should be asked about their level of alcohol use at registration with the practice and advice given to those drinking above the recommended maximum. Indeed, this is the focus of the recently renewed Alcohol Direct Enhanced Service (DES) in England, which financially rewards practices screening all new patients aged 16 years and over and appropriately referring individuals for further support if scoring above the threshold. These aims are mirrored by the alcohol Enhanced Service Programmes in Scotland, Northern Ireland and Wales. Patients undergoing annual review for any chronic health conditions should also be asked about their alcohol use and offered advice and support as appropriate. Standard practice in the UK is to assess alcohol intake in terms of the ‘units’ system (see Box 1).
What ‘alcohol units’ mean in practice
For men: 3–4 units/day
For women: 2–3 units/day
10 ml (8 g) of pure alcohol
1 × 25 ml measure of standard spirits
One-third of a pint of standard strength lager
Half of a standard 175 ml glass of wine
The use of standardized screening questionnaires is recommended when alcohol use is excessive. Screening is also important when there is clinical suspicion that a patient may be harmfully using alcohol, for example, when clinical findings suggest a disease or condition that can be secondary to excessive alcohol use or when there is direct evidence of intoxication or self-neglect. The identification of risk factors, such as previous history of excessive alcohol use, emotional or family problems, drug problems, recurrent absenteeism or social isolation, should also prompt the use of a screening tool. Two commonly used screening tools are the ‘CAGE’ questions and the more detailed alcohol use disorders identification test (AUDIT) tool recommended by the World Health Organization (2001a), which are shown in Box 2.
Medical complications of chronic alcohol misuse
Figure 1 summarizes the spectrum of medical complications that can be associated with harmful drinking. While a variety of chronic conditions can be exacerbated by heavy alcohol use, there are some medical conditions that occur primarily as a consequence of problem drinking. Box 3 summarizes some of the more common biochemical abnormalities that may be associated with excessive alcohol consumption and may be useful for estimating the extent of alcohol excess and as a discussion point with patients about the physical harm their alcohol use is having.
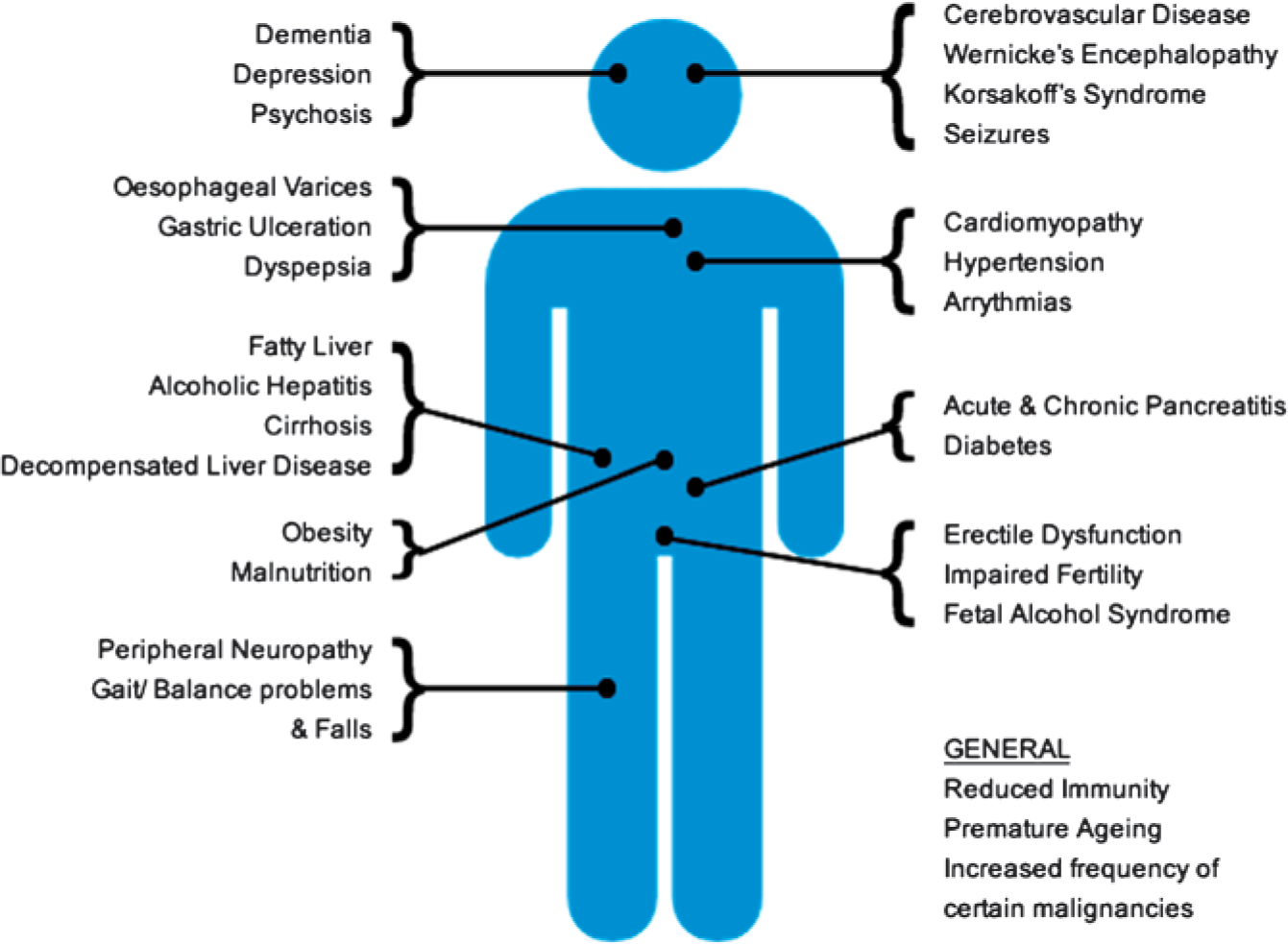
The medical consequences of harmful drinking.
Alcohol withdrawal and delirium tremens
Chronic heavy alcohol use is associated with features of withdrawal when individuals suddenly reduce their intake or stop altogether. Sometimes this can be as a result of a self-initiated attempt to ‘detox’ and sometimes as a result of an abrupt change in the availability of alcohol due to social upheaval or financial consequences. Features of minor withdrawal include anxiety, mild tremor, tachycardia and sweating.
More severe withdrawal may manifest itself as delirium tremens, with the features indicated in Box 4. Delirium tremens has a high mortality rate of up to 15% if not adequately managed and therefore should be considered a medical emergency requiring prompt hospital admission for in-patient management. Alcohol withdrawal seizures, should they occur in the primary care setting, should be managed as for any other seizure: ensure that the airway is clear, remove obstacles from the immediate vicinity, if possible turn the patient into the recovery position and give consideration to 5–10 mg of per rectum (PR) diazepam if the seizure does not spontaneously settle within a few minutes. An ambulance should be called to arrange urgent transfer of any patient who has an alcohol-related seizure in the community.
Harmful alcohol use screening tools
Have you ever felt you should
Have people
Have you ever felt
Have you ever had a drink first thing in the morning to steady your nerves (an
A score of 2 or more is considered clinically significant.
AUDIT

Blood abnormalities associated with alcohol use
Elevated mean cell volume (MCV)
Low platelet count
Low haemoglobin (associated with chronic iron deficiency of malnutrition but is commonly normal)
Low vitamin B12/folate (associated with chronic malnutrition)
Elevated alanine aminotransferase (ALT) and aspartate aminotransferase (AST) (mildly in alcohol-related fatty liver, markedly in acute alcoholic hepatitis)
Elevated bilirubin (in acute alcoholic hepatitis or decompensated disease. May be normal in chronic stable cirrhosis)
Elevated alanine phosphatase (ALP) (may be only slightly raised in both cirrhosis and acute hepatitis)
Elevated gamma-glutamyl transpeptidase (GGT) (raised in heavy alcohol consumption even in the absence of liver damage)
Low albumin (in cirrhosis and decompensated disease)
Elevated international normalized ratio (INR) (in acute hepatitis and decompensated disease)
Elevated amylase/lipase (in acute alcoholic pancreatitis)
Low urea (found in chronic alcohol use)
Reduced potassium, magnesium or calcium
Wernicke's encephalopathy
This form of encephalopathy is caused by a deficiency of thiamine (vitamin B1) and is common with chronic alcohol excess and malnutrition. It is recognized by its characteristic clinical triad of ophthalmoplegia, ataxia and confusion. Most commonly, the ophthalmoplegia involves the external recti muscles; however, a variety of eye signs including ptosis, nystagmus and papillary abnormalities can be seen. It can also be associated with peripheral neuropathy. It is important to have a low clinical suspicion of an evolving encephalopathy in at-risk patients, as not all the characteristic features may be present. Prolonged periods of vomiting or other intercurrent acute illness can precipitate Wernicke's encephalopathy, as can administration of glucose.
Clinical features of delirium tremens
It is recommended that all harmful or dependent drinkers be encouraged to take prophylactic oral thiamine at a dose of at least 200 mg daily if they are at risk of malnourishment, have signs of liver disease or are actively withdrawing. Anyone with suspected features of Wernicke's encephalopathy should be referred to hospital as an emergency for the administration of parenteral high-dose thiamine.
Korsakoff syndrome
This irreversible syndrome, also a result of thiamine deficiency, may follow untreated Wernicke's encephalopathy and highlights the importance of prompt thiamine treatment in those deemed at risk. It is characterized clinically as an inability to form new memories and by periods of (often plausible and convincing) confabulation. Korsakoff syndrome can be a very disabling and distressing condition and therefore needs to be managed in partnership with specialist neuropsychiatric services.
Other neurological conditions
The long-term neurological effects of chronic alcohol use include alcoholic neuropathy, with its associated reduction in mobility and increased falls risk. The effects can be far reaching, including implications for continence, speech, swallowing and impotence in men. Alcohol-related dementia can cause significant long-term cognitive impairment and often follows the Wernicke—Korsakoff syndrome.
Alcohol-related liver disease
The spectrum of alcohol-related liver disease ranges from reversible transient conditions to chronic and life-limiting irreversible damage. The most common hepatic complication of alcohol use is alcohol-associated fatty liver disease, which affects up to a quarter of adults in the UK, the majority being due to alcohol. It is caused by an accumulation of triglyceride vacuoles in the liver parenchyma and is associated with deranged serum ALT, AST and GGT levels. It may be asymptomatic and appear only on routine bloods performed for other reasons or may present with a smoothly enlarged liver or symptoms of abdominal pain and nausea. However it is detected, the presence of alcohol-associated fatty liver disease should prompt a full assessment and discussion by the GP about alcohol use, as the condition predisposes to alcoholic hepatitis and potentially fatal cirrhosis. It is reversible by abstinence from alcohol.
Alcoholic hepatitis can present as any other acute hepatitis, with diarrhoea and vomiting, abdominal pain, tachycardia, pyrexia and clinical features of tender hepatic enlargement, jaundice and ascites. Box 3 summarizes the biochemical abnormalities that may be seen with this condition. Referral to a hepatologist or gastroenterologist is important as the majority progress to cirrhosis, and fulminant hepatic failure can occur in up to 10% of cases. Specialist assessment may involve liver biopsy, corticosteroid treatment and even consideration of transplantation in severe cases.
Liver cirrhosis is the ultimate consequence of long-term excessive alcohol consumption. It is important to recognize that only a quarter of alcoholics will develop cirrhosis (or pancreatitis), probably due to individual genetic factors. However, approximately a quarter of cases of liver cirrhosis in the UK are as a result of alcohol. It is caused by fibrotic nodular regeneration of hepatic tissue. Clinically, cirrhosis can manifest with hepatomegaly, although the liver shrinks in size and becomes firm as disease progresses. Clinical findings of spider naevi, clubbing, gynaecomastia, Dupuytren's contractures, palmar erythema or the manifestations of portal hypertension should prompt the GP to consider cirrhotic liver disease. When associated with continued alcohol use, it carries a nearly 50% 5 year mortality rate. The presence of decompensated liver disease, as evidenced by new jaundice, encephalopathy, oedema and ascites or associated renal impairment (the so called hepato-renal syndrome), should prompt urgent referral to a specialist as this carries a very poor prognosis.
Alcohol-related pancreatitis
Alcohol is one of the most common causes (along with gallstones) of acute pancreatitis and the most common cause of chronic pancreatitis. Both may present to primary care, and GPs commonly have to manage the long-term consequences of pancreatic damage—notably including diabetes mellitus. Acute pancreatitis may present following a ‘binge’ and can manifest as boring epigastric pain that radiates to the back which is worse on laying flat, vomiting and general systemic features of evolving shock. Acute pancreatitis is a result of pancreatic auto-digestion by pancreatic enzymes, leading to elevated serum lipase or amylase levels. Referral for acute admission under either the medical or the surgical team (depending on local policy) is mandatory as acute pancreatitis requires close monitoring and carries a 5–10% mortality rate. It is generally advised to avoid morphine pre-hospitally due to the potential to induce spasm of the sphincter of Oddi.
Chronic pancreatitis is a relapsing—remitting condition, which can present with acute flares in a similar way to acute pancreatitis. Serum markers are often normal as pancreatic function declines with gradually increasing fibrosis. Again, referral to a specialist gastroenterologist is recommended as patients will likely need a multidisciplinary approach to manage the pain of flare-ups, initiate insulin replacement therapy if necessary and adhere to a low-fat and high-calorie diet with appropriate vitamin and enzyme supplementation. GPs should also consider referral to a dietician as these patients are at risk of malnutrition due to poor fat-soluble vitamin absorption.
Other gastrointestinal diseases
Significant gastrointestinal morbidity can result from the complications of portal hypertension. Oesophageal varices and the potential for life-threatening haemorrhage result from porto-systemic shunts. Alcoholic cirrhosis is the most common underlying cause of bleeding varices and is a distressing and alarming emergency requiring hospitalization for urgent endoscopy. A history of haematemesis in a heavy drinker should also prompt the primary care clinician to consider gastric erosions and peptic ulcer disease. Indeed, current guidance suggests that alcohol can be a precipitant of symptoms in non-ulcer dyspepsia.
Cardiovascular conditions
The relationship between alcohol consumption and cardiovascular health is complex and has been the subject of much research. While some evidence suggests a slight protective relationship between a small amount of alcohol intake (1–2 units daily) and cardiovascular events, the relationship is not even across men and women, is possibly related to the type of alcoholic drink and is only valid for very modest amounts of daily consumption. Increasing above the recommended daily maximum intake (see Box 1) is associated with hypertension, arrhythmias (particularly atrial fibrillation), dilated cardiomyopathy and cerebrovascular disease. The overall advice remains that while a small amount of some forms of alcohol may be of benefit, regularly exceeding the recommended daily maximum is associated with significantly increased risk to cardiovascular health.
Mental health and alcohol
Heavy alcohol misuse is associated with 15–25% of suicides and 65% of suicide attempts. Increasing numbers of alcohol-related psychiatric problems are being reported, with alcohol affecting mood, motivation, learning and attention and memory. The association between alcohol and depression is not a clear cause-and-effect relationship. Advice from the Royal College of Psychiatrists suggests that there are complexities between the psychological use of alcohol to alleviate perceived symptoms of low mood and an increased likelihood of depression and psychosis in those who drink heavily. An awareness of this complex relationship is important in primary care as screening for excessive alcohol use in those with mental health problems is as important as seeking out underlying mental health issues in those who drink heavily.
Other health implications
As there are in excess of 50 calories per unit of pure alcohol, a pint of regular strength lager can contain 250 calories. A significant proportion of an individual's recommended daily calories can be accounted for by alcoholic drinks alone if regularly exceeding the recommended daily maximum intake. This can have two diverse implications—firstly in someone maintaining a normal (or excessive) calorie intake alongside this, the alcohol can contribute to the development of obesity and its associated health complications. Conversely, as these calories have limited nutritional value, chronic excessive drinkers can fairly quickly become malnourished.
Primary health care clinicians should also be aware of the variety of physical health implications that, while not solely caused by alcohol, are associated with long-term excessive drinking as summarized in Fig. 1. GPs should also discuss alcohol use during reproductive health consultations, particularly as part of the management of erectile dysfunction and sub-fertility.
Alcohol and pregnancy
The link between excessive alcohol during pregnancy and foetal alcohol syndrome (FAS) is well established. The amount of alcohol at which the risk of FAS increases is less clear. While there is some evidence that small amounts of alcohol during pregnancy might not be harmful (one to two units of alcohol once or twice a week), the current Royal College of Obstetricians and Gynaecologists recommendation is that advising women not to drink alcohol at all during pregnancy is safest particularly in the first trimester.
Non-medical complications of alcohol use
Social
A variety of social factors are associated with problem drinking and it can often be difficult to separate cause and effect. Criminal activity is strongly associated with harmful alcohol use, and the current UK prison inmate population consumes a significant percentage of the budget (in excess of 100 million pounds) spent annually on specialist alcohol services in the UK. Nearly a third of sexual offences and burglaries in the UK have alcohol as a precipitating factor, and acute intoxication is associated with half of all street crime. The relationship with alcohol use and substance misuse is also well established. Unemployment, dropping out of formal education, being arrested and having financial problems are all strongly associated with harmful drinking.
Domestic
Alcohol misuse is strongly associated with domestic violence towards both genders and is linked to around a third of all episodes of reported domestic violence in England. Marriages and partnerships where at least one individual has alcohol problems are twice as likely to end in divorce. This directly impacts upon children and family stability, and it is estimated that up to 1.3 million children suffer harm or neglect as result of a parental alcohol problem. As a result, it is recognized that children of parents with alcohol problems perform less well at school and achieve lower examination performance than their peers. These children are more than twice as likely to develop a harmful relationship with alcohol themselves as adolescents and adults, thus perpetuating the cycle of alcohol misuse.
In primary care, all these problems could become evident during a consultation and should prompt the GP to consider whether alcohol is a precipitating or perpetuating factor in a variety of social problems. While it will not be possible to solve all of these wider issues, reducing the harm that alcohol has on an already difficult social situation may be significantly beneficial. Consideration must also be given to the safeguarding of children and vulnerable adults in situations where problem drinking is evident, including the involvement of necessary support services.
Alcohol and driving
Driving while acutely intoxicated has obvious potentially disastrous consequences, but the Driver and Vehicle Licensing Agency (DVLA) also sets down patterns of problem alcohol use that might result in refusal or revocation of a driving license. For example, alcohol dependence requires a period of 1 year ‘free from alcohol problems’ and a single alcohol-related seizure requires 6 months without driving. The DVLA also states that ‘driving should cease’ when certain alcohol-related disorders are identified, including cirrhosis and neuropsychiatric disorders. The regulations for commercial drivers are even stricter. GPs must remind patients of the need to inform the DVLA when harmful drinking is identified and be sensitive to the difficulties this may result in.
Binge drinking
Binge drinking refers to the consumption of excessive amounts of alcohol in a short time period, often with the specific intention of becoming intoxicated. The exact quantification of what constitutes a binge is less clearly defined, but the National Health Service (NHS) and Office of National Statistics consider anything in excess of double the recommended daily maximum to be a ‘binge’. The practice of binge drinking statistically peaks among individuals in their early to mid-20s, with data from the Academy of Medical Sciences (2004) suggesting that 23% of adult males and 9% of adult females engage in binge drinking. However, recent concern is growing over the number of increasingly younger adolescents who engage in the practice. Factors behind binge drinking are complex, but most experts recognize the interplay between social and personal factors. The availability of inexpensive alcohol (particularly so called Ready to Drink ‘alcopop’ products), the change in licensing laws to allow the 24 hour retail of alcohol and a shift in youth culture (particularly in Northern European countries) to include excessive alcohol as part of socializing have all been blamed.
Risk-taking behaviour and alcohol
Binge drinking is associated with its own risks to health. Harmful effects are essentially dose related, with altered behaviour ranging from mild relaxation to euphoria and from violent aggression to coma depending on the individual and amount consumed. Binge drinkers are at higher risk of accidents and sustaining trauma due to impaired motor co-ordination, more likely to engage in risky behaviour including unsafe sex, engage in more self-harm events and suicidal behaviours and can suffer the consequences of acute toxicity such as hypoglycaemic collapse, coma, arrhythmias and cerebrovascular events. UK death rates due to acute alcohol intoxication have doubled in the last two decades, and data suggest that 29% of all injury-related deaths occur when the individual is acutely intoxicated.
As binge drinkers are often younger adults and adolescents, their contact with primary care services may be relatively limited. However, factors that might trigger a GP to screen for binge drinking behaviour may include repeated patterns of absence from school, college, university or work secondary to being ‘hung over’, repeated episodes of injury or self-harm, presentation with sexually transmitted infections and as part of a wider evaluation of mental health or social problems. It is recommended that all young adults with depressive symptoms are asked about their alcohol use as the link is well established.
Managing the complications of alcohol
GPs are ideally placed to help patients tackle the problem of harmful drinking before the physical and psychosocial damage is irreversible. The ‘Management of Harmful Drinking’ article, also in this month's journal, covers in detail strategies of brief intervention, detoxification, supporting abstinence and harm reduction.
Key points
Regularly exceeding the recommended daily maximum intake of alcohol has significant and diverse physical and mental health implications
There is a complex relationship between alcohol use and psychosocial factors
Binge drinking has its own health implications, mainly related to the dangers of acute intoxication and increased risk-taking behaviour
The long-term health complications of excess alcohol use require a multidisciplinary approach in conjunction with specialist support services
GPs should be aware of the need to use screening questionnaires to identify problem drinking