
Abstract
Contraception can be a daunting topic for both patients and doctors. However, choosing effective contraception offers choice in determining family size and spacing. Worldwide effective contraception prevents an estimated 187 million unintended pregnancies and averts an estimated 2.7 million infant and 215 000 pregnancy-related deaths. Progestogen only pills (POPs) are one of the many choices available.
The GP curriculum and progesterone only pill
Contraception—effectiveness rates, risks, benefits and appropriate selection of patients for all methods, including methods of emergency contraception Contraception—the safe provision of all methods of oral contraception (including emergency hormonal contraception) Health education and prevention advice—safe sex and risk reduction Ensure that the doctor's own beliefs, moral or religious reservations about any contraceptive methods or abortion and about sexual behaviour and practices do not adversely affect the management of a patient's sexual health Be aware of the legal aspects of providing contraception and sexual health in under 16s (including child protection)
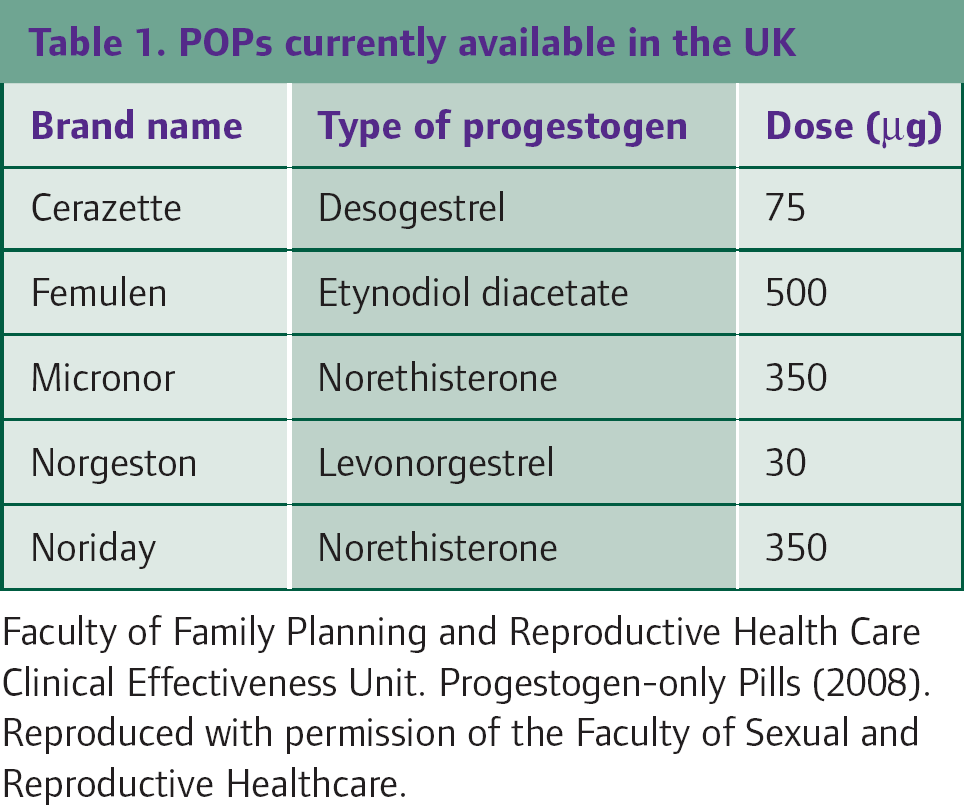
POPs contain only the hormone progesterone. Those available in the UK are summarized in Table 1. Traditional POPs include those containing levonorgestrel, norethisterone or etynodiol diacetate. The desogestrel-only pill is considered one of the new generations of POPs. As a result of their composition, POPs often offer a suitable alternative when oestrogens found in the combined hormone pills are contraindicated, for example, in those with a history of venous thromboembolism.
POPs currently available in the UK
General points
Contraception can be the priority issue of the consultation or arise opportunistically. It is vital to give adequate time to listen to and discuss a patient's health beliefs. Exploring understanding, concerns and expectations, as well as addressing all-too-common misconceptions, can help lower discontinuation rates and the risk of unwanted pregnancies.
It is not always feasible to complete this in one sitting, so providing verbal as well as good quality written information is vital, for example, leaflets provided by the Family Planning Association or www.patient.co.uk. The decision on contraceptive method should be patient centred, with women advised about appropriate options, without unnecessary restrictions.
Opportunistic health care can be provided covering important issues such as previous contraception use and experience, family planning ideals, sexually transmitted infection (STI) risk, cervical cancer screening, smoking and weight. The World Health Organization (WHO) suggests documenting blood pressure prior to starting a POP, although it will not necessarily influence POP use.
Assessment
For the majority of women, a POP is a safe method of contraception. The UK Medical Eligibility Criteria (UKMEC) set out guidance for the safe use of all forms of contraception in patients with a variety of clinical problems (Table 2).
UKMEC criteria
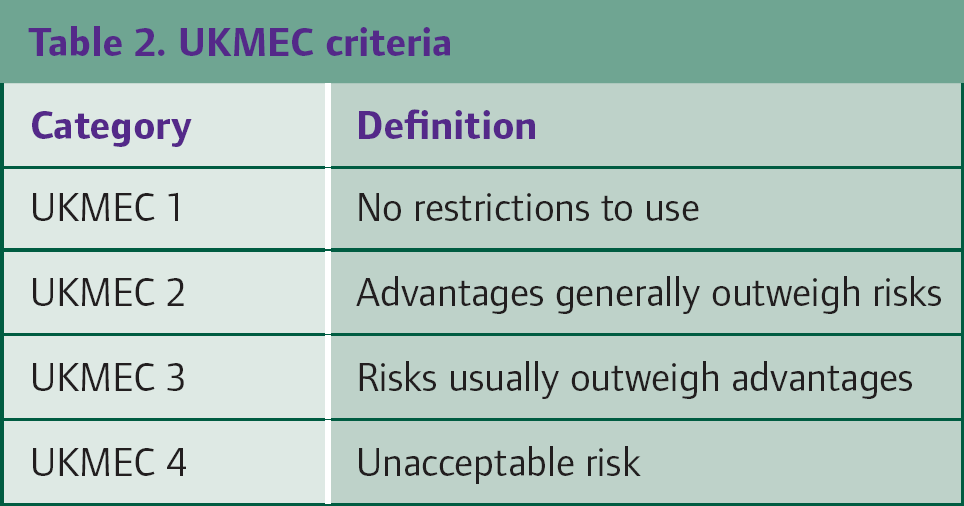
GPs may consider providing contraception, with appropriate follow-up, to those with conditions falling within UKMEC 1 and 2. However, those with conditions falling under UKMEC 3 should be referred to a specialist contraception provider. For those with conditions falling under UKMEC 4, contraception poses an unacceptable health risk.
UKMEC and POP
A clinical history should identify any conditions that fall within UKMEC 3 and 4 for the preferred type of contraception. For the POP, under UKMEC 4, current breast cancer poses an unacceptable health risk, so a POP should not be used in those circumstances.
For the POP, the following situations fall under UKMEC 3, where it would be advisable not to provide a POP and to refer to a specialist contraception provider for further advice.
The initiation of a POP in women with a history of breast cancer but with no evidence of disease in the last 5 years; those with a history of gestational trophoblastic neoplasia; patients with active viral hepatitis, severe decompensated cirrhosis or liver tumours and patients using liver enzyme-inducing medication The continuation of a POP by women with the occurrence of new symptoms or having a new diagnosis of ischaemic heart disease, stroke or migraine with aura
Information about the POP
Many factors will influence a woman's choice of contraception and women should be fully informed before they make any choice about method of contraception. For the POP, provide information on mode of action, efficacy, side effects and fertility post-cessation.
Mode of action
All POPs alter cervical mucus to prevent sperm entering into the upper reproductive tract. The traditional POPs work primarily by this action, but the POP may also inhibit ovulation in some women. The primary mode of action of the desogestrel-containing pill (Cerazette) is inhibition of ovulation. Up to 60% of cycles in women using a levonorgestrel-only pill are anovulatory compared with up to 97% in women using the desogestrel-only pill.
Efficacy
Ideally, POPs should be taken at the same time every day with no pill-free interval. With perfect use, POPs are more than 99% effective in preventing pregnancy. There are no data to suggest the superiority of one POP over another.
Previously, it was thought that the efficacy of the traditional POPs may be reduced in women weighing more than 70 kg. Subsequently, this lead to the unlicensed use of two traditional POPs per day. However, there is no evidence that the efficacy of the traditional or desogestrel POPs is influenced by weight, so the licensed use of one pill/day is recommended.
Missed pills
Figure 1 outlines advice for women when a POP is late or missed. If a traditional POP is more than 3 hours late or a desogestrel-only pill is more than 12 hours late, missed pill rules should be followed. Women should

Missed pill advice relating to POPs.
take the late or missed pill immediately continue pill taking as usual (which may mean taking two pills at the same time) use condoms or abstain from intercourse for 48 hours after the missed pill is taken until the effect on cervical mucus has been restored. Emergency contraception may be indicated if unprotected sex occurs during this 48 hour period.
In clinical trials, the efficacy of the traditional and desogestrel-containing pills has been similar. However, the longer window that a woman has to remember to take her pill with desogestrel-containing POPs may facilitate timely pill taking, which may improve their efficacy. For example, the 12 hour window available with the desogestrel-containing POP may improve timely pill taking in a lady working shift patterns who does not want to have a long-acting form of contraception. If forgetting to take the pill is not an issue, it is important to prescribe cost-effectively. One month of desogestrel-containing POP, Cerazette, costs £8.68 compared with £2.10 for 1 month of Noriday.
Vomiting and diarrhoea
If a woman vomits within 2 hours of taking a POP, then she should be advised to take another pill as soon as possible. If she exceeds the 3 hour limit (or 12 hours for a desogestrel-only pill), continues to vomit or has very severe diarrhoea, she will need to follow the missed pill rules.
Drug interactions
Theoretically, liver enzyme-inducing drugs increase the metabolism of progestogen. This may decrease the contraceptive efficacy of POPs. Thus, their concomitant use long term is not recommended. Commonly encountered liver enzyme-inducing drugs include rifampicin, carbamazepine, phenytoin, topiramate and St John's Wort.
After stopping a liver enzyme-inducing drug, it can take up to 4 weeks for liver enzymes to return to normal; therefore, if a POP is started during this time, condoms or abstinences are advised. Efficacy of POPs is not affected by non-liver enzyme-inducing antibiotics such as amoxicillin.
Return of fertility
There is no delay in return of fertility following discontinuation of POPs. Thus, after cessation, another suitable form of contraception should be sought if pregnancy is not desired.
Side effects and discontinuation
Altered bleeding patterns are the most common reason for stopping POPs. Almost half of POP users experience prolonged bleeding; up to 70% report breakthrough bleeding or spotting in one or more cycles. Women should be advised about the likelihood and types of bleeding patterns expected with POP use. As a general guide:
20% of women will be amenorrhoeic 40% will bleed regularly 40% will have erratic bleeding
Between 10 and 25% of women using a POP will discontinue this method within 1 year as a result of these bleeding patterns. Effective counselling about the likelihood of changes to bleeding can help reduce discontinuation rates.
Other noted side effects include nausea, vomiting, dizziness, breast discomfort, skin disorders and altered libido. There is no evidence of a causal association between POPs and weight change, depression, headache, cardiovascular disease (myocardial infarction, venous thromboembolism and stroke) or breast cancer.
Sexual health
Contraception is tied with sexual health issues. When seeing women about contraception, consider discussing and assessing STI risk as well as providing advice regarding safer sex and condom use to reduce transmission of STIs.
Initiation
POPs can be started up to and including Day 5 of the menstrual cycle without the need for additional contraceptive protection. POPs can also be started at any other time if the clinician is reasonably certain that the woman is not pregnant and there has been no risk of conception (Box 1). Additional contraception or abstinence is advised for 48 hours after initiation.
Criteria for excluding pregnancy
Health professionals can be ‘reasonably certain’ that a woman is ‘not currently pregnant’ if one or more of the following criteria are met and there are no symptoms or signs of pregnancy:
No intercourse since last normal menses Correctly and consistently using a reliable method of contraception Patient is within the first 7 days of the onset of a normal menstrual period Patient is within 4 weeks postpartum for non-lactating women Patient is within the first 7 days post-abortion or miscarriage Patient is fully or nearly fully breastfeeding, amenorrhoeic and less than 6 months postpartum
A pregnancy test adds weight to the exclusion of pregnancy, but only if more than 3 weeks since the last episode of unprotected sexual intercourse.
Health professionals should also consider whether a woman is at risk of becoming pregnant as a result of unprotected sexual intercourse within the last 7 days.
Faculty of Family Planning and Reproductive Health Care Clinical Effectiveness Unit. Quick Starting Contraception (2010).
Postpartum
Women who are postpartum (vaginal or operative delivery) may choose to use a POP without restriction regardless of how they are feeding their baby (UKMEC 1). If started up to and including Day 21, contraceptive protection is immediate. If starting after Day 21, condoms or abstinences are advised for 48 hours. This advice is based on the earliest date of ovulation of postnatal women.
Following abortion or miscarriage
The use of POPs is unrestricted in women following abortion (UKMEC 1) or miscarriage (under 24 weeks gestation). If a POP is started more than 5 days after abortion or miscarriage, then condoms or abstinences are required for the next 48 hours.
Following use of emergency contraception
If starting a POP immediately after levonorgestrel emergency contraception is used, advise additional contraception (condoms or avoidance of sex) for the first 2 days of use. If starting immediately after ulipristal acetate emergency contraception is used, advise additional contraception (condoms or avoidance of sex) for the first 9 days of use. Advise all women to take a pregnancy test no sooner than 3 weeks after the last episode of unprotected sex.
Ongoing use
A woman may be offered up to 12 months supply of POPs at her first and subsequent visits. Follow-up should be tailored to the individual woman, encouraging earlier review for problems experienced at any time. Reviews should address any problems with pill taking, side effects, bleeding patterns, any change in medical details or medications, family and sexual history.
Managing bleeding problems
Bleeding is a common problem for POP users. There is no way of predicting who will have what pattern of bleeding and the duration of this change. In women who have persistent bleeding beyond the first 3 months of use, a change to their normal bleeding pattern or symptoms like pain, dyspareunia or post coital bleeding, the following causes should be considered:
STIs (in particular Chlamydia trachomatis) concordance issues drug interactions pregnancy gynaecological pathology, e.g. cervical cancer
There is no clear evidence that changing the type and dose of progestogen will improve bleeding, but subjectively, this does seem to help some individuals. If, after exclusion of other causes, bleeding patterns are still unacceptable, then an alternative contraceptive method may need to be considered.
Special groups
Women aged over 40 years
Women may use the POP until the age of 55 years when natural loss of fertility can be assumed. Alternatively, a woman can continue using a POP and have follicle-stimulating hormone (FSH) concentrations assessed on two occasions at least 1 month apart. If both FSH measurements are greater than 30 IU/l, this is highly suggestive of ovarian failure. In this case, the woman may continue with a POP for a further period of 1 year (or 2 years if she is aged under 50 years). POPs may be used with hormone replacement therapy (HRT) to provide effective contraception, but the HRT must include progestogen in addition to oestrogen too.
Young people
POPs may be prescribed from menarche onwards. The correct and consistent use of condoms should be advised to reduce the risk of STIs. The main challenge with prescribing for this group is not in the medical technicalities but more the ethical and confidentiality challenges presented.
The legal age of consent is 16 years. In England, Wales and Northern Ireland, those under the age of 13 years are considered unable to legally consent to sexual activity. This would be considered statutory rape. Young people should always be made aware of the confidentiality policies for the service they are attending, including the circumstances in which confidentiality may be breached.
A clinician should assess a young person's competence to consent to treatment by their ability to understand information provided, to weigh up the risks and benefits and to express their own wishes. Competence to consent to treatment should be assessed and documented at each visit. Health professionals may wish to use checklists like the Fraser guidelines to assess competence and risk (see Box 2).
Fraser guidelines
The young person understands the professional's advice
The young person cannot be persuaded to inform her parents
The young person is likely to begin, or to continue, having sexual intercourse with or without contraceptive treatment
Unless the young person receives contraceptive treatment, her physical or mental health or both are likely to suffer
The young person's best interests require her to receive contraceptive advice or treatment with or without parental consent
Concordance can be an issue with young patients. Even if the patient specifically requests POPs, it is always worthwhile exploring her understanding about long-acting reversible forms of contraception (such as contraceptive implants) and offering these instead if appropriate because of their superior cost-effectiveness and efficacy in preventing pregnancy.
To aid timely pill taking, it may be more appropriate to offer the desogestrel-containing POP with its 12 hour window to young people as opposed to the traditional pills with their 3 hour window. It is also possible to set up daily alarms or text messages via mobile phones to remind patients of when the pill should be taken.
Key points
The UKMEC criteria determine safety of use of different methods of contraception in a variety of clinical circumstances Effective counselling and a patient-centred approach are vital in contraception provision POPs provide a 99% effective form of contraception with perfect use They work by thickening cervical mucus and inhibiting sperm penetration, as well as by inhibiting ovulation They are a suitable alternative in women who have some medical contraindications to combined hormone pill use Changes in bleeding pattern are a common unpredictable side effect of the POP which women should be warned about