
Abstract
Afemale genital prolapse, or pelvic organ prolapse, is a hernia of one or more pelvic organ (uterus, vaginal apex, bladder or rectum) and its associated vaginal segment into the vaginal canal. The exact prevalence of prolapse is unclear because many women do not report it; however, prolapse is a common presenting complaint in primary care. It is therefore vital for GPs to understand how to diagnose and treat women with this important condition in an empathetic and sensitive manner.
The GP curriculum and female genital prolapse
Know about common or important conditions such as vaginal and uterine prolapse
Describe the functional anatomy of the male and female genital systems and the female reproductive physiology to aid diagnosis
Perform a gentle and thorough pelvic examination, including digital and speculum examination, assessment of the size, position and mobility of the uterus and the recognition of any abnormality of the pelvic organs, paying attention to professional etiquette, patient consent, comfort and information
Demonstrate an understanding of the importance of risk factors in the diagnosis and management of women's problems
Demonstrate a reasoned approach to the diagnosis of women's symptoms in a manner that is comfortable for both the patient and the GP using history, examination and incremental investigations and refer appropriately
Communicate sensitively with women about intimate issues
How can prolapse occur?
The vagina is a 7–9 cm fibromuscular canal which extends from the uterus to the vulva. Pelvic organs are supported and kept in position by the ligaments, fascia and muscles of the pelvic floor. The anatomy of the female genital system is shown in Fig. 1. There are several risk factors (Box 1) which can cause damage to these structures and thus predispose women to prolapse.

The female genital system.
Risk Factors for prolapse
Childbirth—higher risk with difficult long delivery and large baby
Previous pelvic surgery—hysterectomy, colposuspension and sacrospinous fixation
Peri/postmenopausal—due to oestrogen deficiency
Chronic cough—increase in intra-abdominal pressure
Ascites
Repeated lifting of heavy weights
Habitual straining due to constipation
Large pelvic tumour
Advanced age
Obesity
Dysfunction of the nerves and tissue
Congenital collagen deficiency (rare)
Symptoms
Most women presenting with prolapse are over the age of 40 years. The type of symptoms depends on the degree of prolapse and the structures involved as summarized in Table 1. Symptoms may only be present when upright, i.e. while awake, and may get worse if standing for a long time, coughing or straining. Common symptoms include:
Symptoms of prolapse

a dragging sensation
a feeling of ‘something coming down’ or a ‘lump’
urinary tract symptoms—stress incontinence, recurrent cystitis and/or frequency of micturition
difficulty in defaecation
dyspareunia
symptoms resulting from complications, such as purulent discharge or vaginal bleeding due to cervical ulceration
Presentation may be delayed due to embarrassment or other personal reasons. Some women who develop vaginal prolapse do not experience any symptoms and prolapse may be found incidentally when doing a pelvic examination for another reason.
Diagnosis
In the primary care setting, female genital prolapse is diagnosed by clinical examination. The patient should be positioned in the left lateral position with her knees drawn up to the chest. The vaginal wall is held back with a lubricated speculum and the prolapse inspected. Ideally, a Sims speculum, also called a univalve speculum, should be used. Any ulceration, atrophy or bleeding are noted. The maximum protrusion experienced by the patient should also be observed as described in Box 2.
Maximum protrusion of prolapse
The full extent of the prolapse can be demonstrated when either:
Protrusion of the vaginal wall has become tight when the patient is asked to strain
The prolapse does not descend anymore after traction
The patient says that the size of prolapse demonstrated in front of the examiner is the same as the most severe protrusion she has had (the patient can use a handheld mirror to visualize this)
A standing and straining examination confirms that the full extent of prolapse is observed when Sims speculum is used
An abdominal and a bimanual pelvic examination are also required. A rectal examination is only indicated if a pelvic mass is suspected. If the patient has any urinary symptoms, dipstick the urine for blood, protein, leucocyte esterase, nitrites and glucose and send a sample of urine for microscopy, culture and sensitivity testing. Imaging is not routinely used in primary care to make a diagnosis of prolapse but is sometimes used to confirm the diagnosis and structures involved in secondary care.
Classification
Different types of prolapse are commonly named according to the organ that prolapses. For example, urethrocele is the prolapse of the urethra into the vaginal canal. However, this classification is not accurate or reliable.
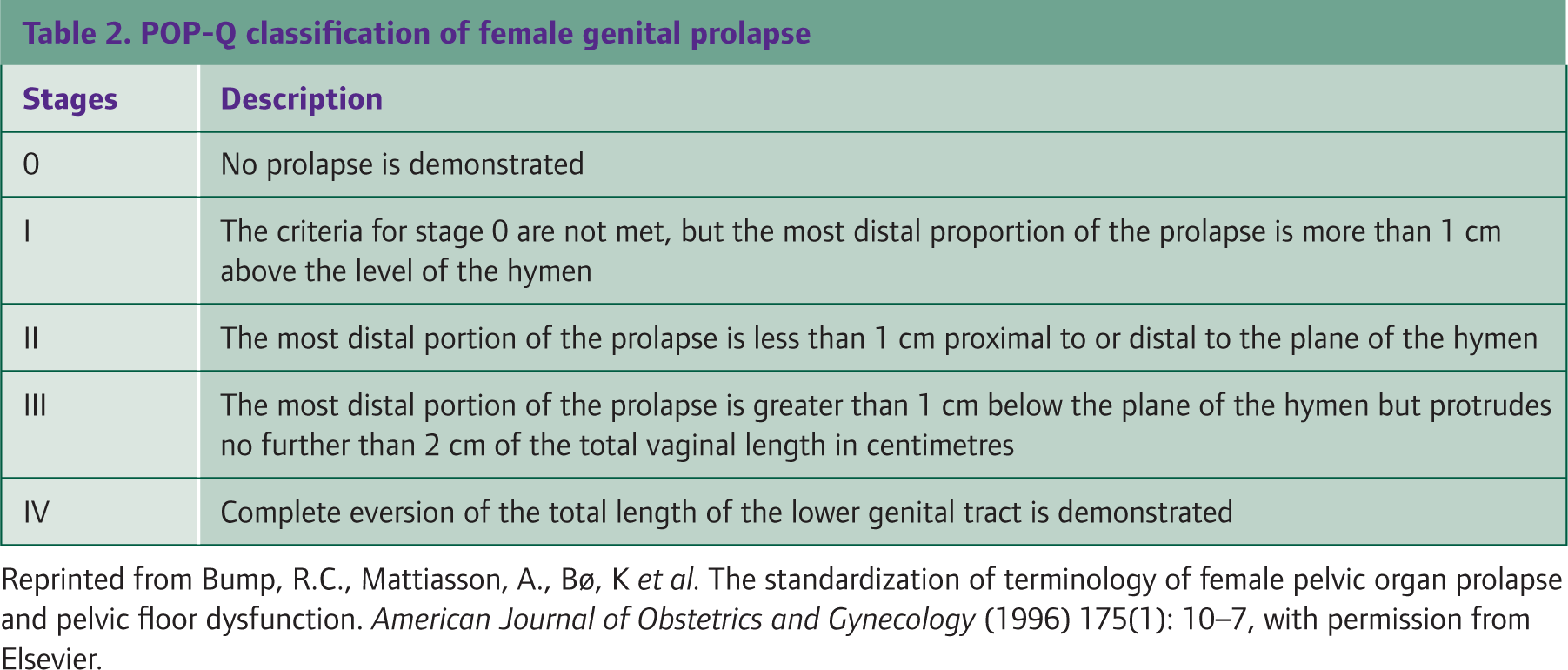
Instead, the Pelvic Organ Prolapse Quantification (POP-Q) should be used to classify genital prolapse regardless of which organ is involved. The hymen (a membrane that surrounds or partially covers the external vaginal opening) is used as the fixed reference point. Severity of the prolapse is classified into five stages as summarized in Table 2.
POP-Q classification of female genital prolapse
Primary care management
The aim of treating prolapse is to relieve symptoms. The choice of treatment depends on patient preference, general health, degree of prolapse, severity of symptoms and wish to preserve fertility and sexual activity.
Lifestyle
Recommend lifestyle changes to all patients. These include:
decreasing weight if overweight
smoking cessation
avoiding heavy lifting
General measures
Treating conditions that contribute to, or exacerbate, prolapse may improve symptoms. These conditions include cough resulting from chronic obstructive pulmonary disease or asthma, constipation or atrophic vaginitis.
Pelvic floor exercises
All patients should be encouraged to try pelvic floor exercises. This can improve muscle function, improve urinary symptoms and reduce back pain and abdominal discomfort. In mild prolapse, pelvic floor exercises may prevent deterioration or progression. However, they are unlikely to improve any prolapse that is already present. There are many websites that give detailed instructions on how to do pelvic floor exercises for patients, such as the Bladder and Bowel Foundation (www.bladderandbowelfoundation.org) and Patient UK (www.patient.co.uk). Consider referral for specialist physiotherapy if the woman finds pelvic floor exercises difficult or if the prolapse does not extend to or below the hymen and self-help measures have failed.
Vaginal pessaries
Vaginal pessaries are rubber or plastic devices that are inserted into the vagina to hold the uterus in place and have been reliably used to treat vaginal prolapse since Roman times. A vaginal pessary can either be of the ring (Fig. 2) or be of the shelf type (Fig. 3). Ring pessaries tend to fail in women with deficient perineum (pelvic floor), who may require shelf pessaries instead. Shelf pessaries interfere with normal sexual intercourse and thus are more suitable for women who are not sexually active.

Ring pessary.

Shelf pessary.
Pessaries can be used as a temporary measure to relieve symptoms of prolapse while awaiting surgery or as a permanent measure for those who are unfit for surgery, decline surgery or wish to have more children [Royal College of Obstetricians and Gynaecologists (RCOG), 2007].
Pessaries are available in a variety of sizes and must be fitted for each individual woman. Vaginal ring pessaries can be fitted in primary care by GPs with appropriate training as described in Box 3. Patients with more advanced prolapse who are unfit for surgery, but whose prolapse cannot be controlled with a single ring pessary, may benefit from insertion of two ring pessaries (Singh and Reid, 2001). Shelf pessaries are not currently available on prescription so can only be fitted in secondary care. For patients with vaginal atrophy, a course of topical oestrogen prior to ring fitting or changing (if there are no contraindications) may make the procedure easier.
Fitting and managing ring pessaries
Do a bimanual examination and use the forefinger to estimate the size of the vagina
Use trial and error to determine which size of pessary should be used and ensure that a variety of sizes and styles are available
Place the pessary in the vagina and encourage the woman to walk around. If she reports pain or discomfort, the pessary is likely to be too big and a smaller one should be tried
If no adverse symptoms such as discharge, pain or bleeding, the pessary can be changed every 6–8 months
Once fitted, if there are no adverse symptoms such as discharge, pain or bleeding, the pessary is generally changed every 6 months (although it is now thought to be safe to leave pessaries in situ for up to 8 months). Patients should be advised to report any problems to their GP or hospital specialist. Complications of pessary use are usually minor and include:
Discomfort
Vaginal erosions or ulceration with or without vaginal bleeding
Vaginal irritation
Unpleasant vaginal discharge
Urinary tract infection
Difficulty with bowel movements
Problems with intercourse
A robust recall system should be in place in GP practices to follow-up patients with pessaries, to ensure that they are changed at the appropriate time. This is particularly important for frail elderly ladies who can easily be lost to follow-up if they develop memory problems or go into residential care. This can be achieved by placing alerts in the patients' electronic notes or highlighting that the patient has a pessary in the active problem list.
Referral to gynaecology
Women with cervical or vaginal ulceration, those who are fit for and would like surgery for prolapse and women who require a shelf pessary should be referred to a gynaecologist.
The indications for surgery are
failure of ring pessary
patients wanting definitive treatment
co-existing urethral sphincter incompetence or faecal incontinence
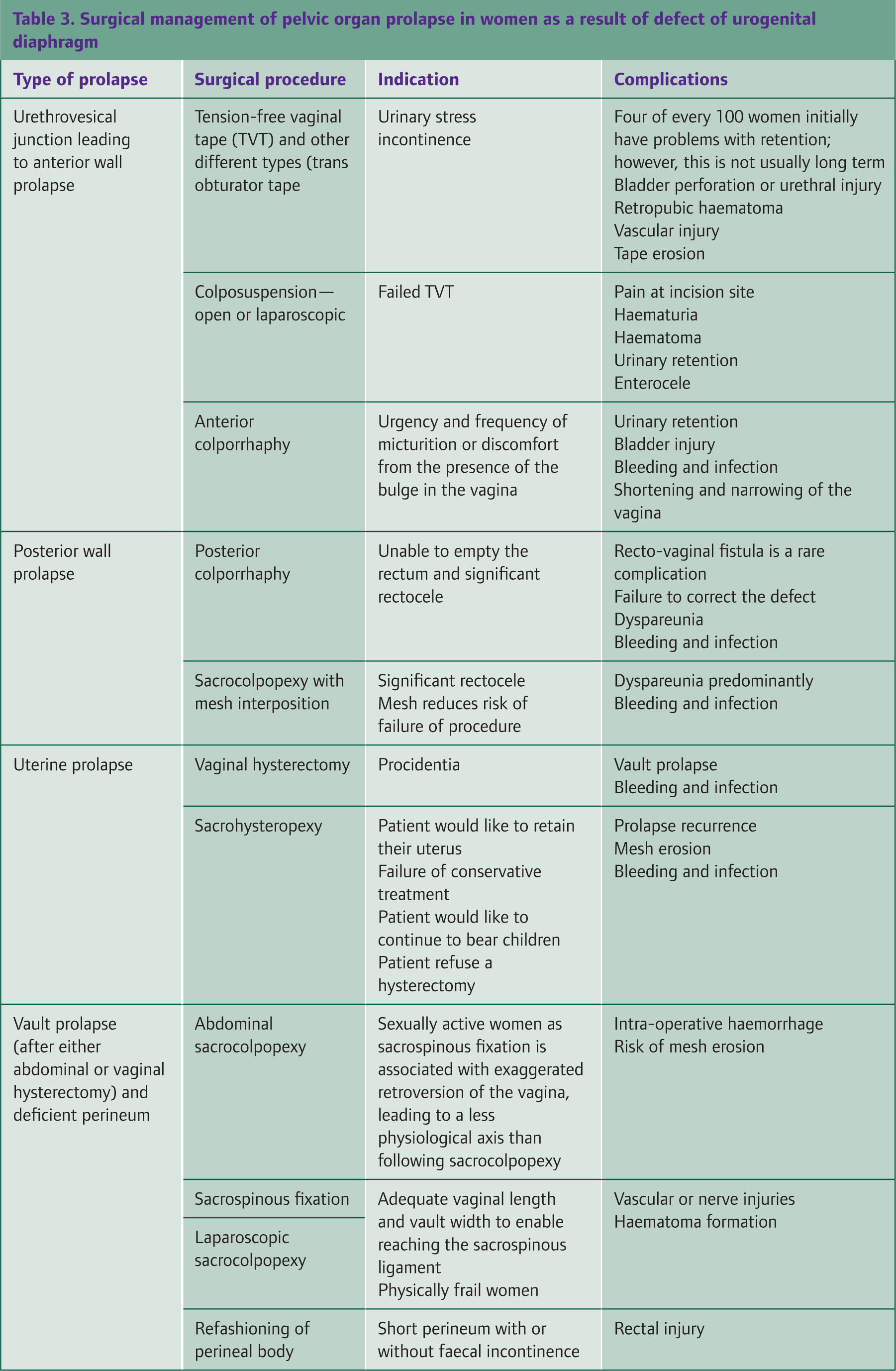
There are a number of surgical procedures used to correct vaginal wall and uterine prolapse and these are summarized for reference in Table 3. The aims of surgery are to provide support for the vagina, restore the affected pelvic organs to their natural position and to prevent another prolapse. Surgery also aims to preserve coitus and urinary and anal continence. Evidence about pregnancy outcome post-corrective surgery is limited; therefore, it is vital to ascertain prior to surgery whether premenopausal patients intend to have children in the future as this may affect the options offered to them. Post-operatively, patients are advised to avoid heavy lifting and strenuous activity for 6–8 weeks to avoid complications.
Surgical management of pelvic organ prolapse in women as a result of defect of urogenital diaphragm
Associated urinary incontinence
The National Institute for Health and Clinical Excellence (NICE) recommends that a trial of supervised pelvic floor muscle training of at least 3 months duration should be offered as first-line treatment to women with stress or mixed urinary incontinence presenting to primary care (NICE, 2006). Pelvic floor muscle training programmes should comprise at least eight contractions performed three times/day. If pelvic floor muscle training is beneficial, an exercise programme should be maintained.
Routine secondary care referral should be considered for women with:
urinary incontinence who have prolapse that is visible at or below the vaginal hymen
persisting bladder or urethral pain
benign pelvic mass (e.g. fibroid)
associated faecal incontinence
suspected neurological disease
symptoms of voiding difficulty and/or
suspected urogenital fistula
Associated pelvic mass
If a pelvic mass is identified during assessment, an urgent referral for ultrasound scan should be arranged if the mass is not obviously uterine fibroids and not of gastrointestinal or urological origin. If the ultrasound scan is suggestive of cancer or urgent ultrasound scan is not available, an urgent referral (to be seen within 2 weeks) to gynaecology should be made to allow timely further investigation (NICE, 2008).
Prevention of prolapse
Take every opportunity to educate younger women about minimizing risk factors for prolapse. These include:
Excess weight—advise weight loss through exercise and healthy diet
Constipation and chronic straining—high fibre diet is recommended with higher fluid intake
Chronic cough—this should be investigated and treated appropriately
Heavy lifting—avoid heavy lifting and learn how to lift safely
Smoking—give advice about smoking cessation
Pelvic floor muscles—regular pelvic floor muscle exercises will strengthen the pelvic floor and decrease likelihood of prolapse
Pregnant women may ask about the possibility of caesarean delivery to prevent the risk of vaginal prolapse in the future. However, in uncomplicated pregnancy, complications associated with caesarean delivery outweigh the risks of prolapse. Furthermore, pregnancy alone, regardless of the method of delivery, contributes to the development of pelvic floor disorders such as prolapse.
Key points
Always consider a diagnosis of genital prolapse in women presenting with genito-urinary symptoms, pelvic fullness or back pain
Female genital prolapse is diagnosed via clinical examination, using a Sims speculum, and must demonstrate the maximum protrusion of the prolapse experienced by the patient
The POP-Q classification is the most reliable and accurate way of classifying female genital prolapse
Primary care treatment involves lifestyle measures, treatment of other contributory medical conditions, pelvic floor exercises and a vaginal ring pessary where appropriate
Secondary care referral should be made for those who are fit enough and wish to have surgery, those who have failed to retain a ring pessary, those with associated urinary incontinence that has not improved with conservative measures or those with associated faecal incontinence
Footnotes
Acknowledgements
We would like to say thank you to Mr Osama Abu-Ghazza, MRCOG, for giving us advice and support.