
Abstract
Oesophageal cancer is a common malignancy with an increasing incidence and often poor prognosis. Symptoms can be non-specific which can lead to late presentation or delayed referral. To improve patient outcomes, GPs need to be aware of the key clinical features of oesophageal cancer and the pivotal role that early referral can play in the patient's management and prognosis.
The GP curriculum and oesophageal and gastric cancer
Ability to function as both leader and member of cancer care teams
Knowledge of referral guidelines and protocols, both local and national
Knowledge of the appropriate investigations of patients with cancer and of how they fit in with national guidelines
Knowledge of the principles of palliative care
Have knowledge of investigations such as Helicobacter pylori testing and
Understand the benefit of smoking cessation and alcohol reduction in preventing GI cancers
Epidemiology
The latest statistics from Cancer Research UK show oesophageal cancer is the sixth most common cause of death from cancer in the UK, despite being only the ninth most common cancer overall. The two most common histological types of malignant tumours occurring in the oesophagus are squamous cell carcinoma (SCC) and adenocarcinoma (AC). Other rarer cancers are listed in Box 1. SCC and AC are two quite different diseases epidemiologically. SCC is more common in the Asian ‘oesophageal cancer belt’ which stretches from Iran to China and has a decreasing incidence in the West. Conversely, AC is more common in developed countries where it has an increasing incidence. This is especially evident among white males, where incidence has risen by over 50% in the last 25 years. In the UK, the recorded rates among this ethnic group are the highest in the world and consequently, the ratio of male to female AC is currently over 7:1.
Rare malignant oesophageal pathologies
Basaloid carcinoma
Mucoepidermoid carcinoma
Endocrine carcinoma
Melanoma
Paget's disease
Choriocarcinoma
Metastases
Survival statistics are universally poor, with 5 year survival rates of around 8% in the last decade. This figure has marginally improved over the last 30 years, which has been partially attributed to reductions in perioperative mortality. Over the same time period, absolute mortality rates have sharply increased, with the mortality rate never lying far below the incidence rate. In the UK, in 2007, there were almost 8000 new cases diagnosed with over 7600 deaths during the same time period.
Aetiology
The aetiology also differs between the two principal histological subtypes of oesophageal carcinoma. The proven risk factors responsible for SCC are smoking, alcohol consumption and a diet poor in fresh fruit and vegetables. Other conditions that confer an increased risk are listed in Box 2.
Predisposing factors and conditions for oesophageal carcinoma
Barrett's oesophagus (AC)
High body mass index (BMI) (AC)
Poor fruit and vegetable intake (AC and SCC)
Tobacco consumption (SCC)
Alcohol ingestion (SCC)
Plummer-Vinson syndrome (triad of iron deficiency anaemia, glossitis and dysphagia due to an oesophageal web)
Howel-Evans syndrome (familial palmoplantar hyperkeratosis with oesophageal SCC)
Oesophageal achalasia (a malfunctioning oesophagogastric sphincter)
Coeliac disease
Gastro-oesophageal reflux disease (GORD) and subsequent development of Barrett's oesophagus are the most important risk factor for oesophageal AC. Others include a high body mass index (BMI) and a poor intake of fresh fruit and vegetables.
Barrett's oesophagus is a condition where the stratified squamous epithelium of the distal oesophagus above the gastro-oesophageal junction undergoes a metaplastic change to become lined by columnar epithelial cells normally found in the gastric cardia. This pathological process is usually a complication of longstanding acid reflux at the gastro-oesophageal junction (see Fig. 1), which is often further compounded by the progressive loss of lower oesophageal sphincter function due to continued cellular insult. This can result in a vicious circle of increasing acid reflux and ongoing epithelial injury.

The sequence of oesophageal AC development.
Barrett's oesophagus is a serious premalignant condition; however, progression from Barrett's to invasive oesophageal AC is not inevitable. Research suggests that malignant transformation occurs in 2–5% of patients, the rest either remaining stable or, more rarely, regressing. Studies looking at the progression of Barrett's oesophagus to invasive AC have identified both the grade of dysplasia present and (to a lesser extent) the length of the oesophageal area affected by Barrett's as strong predictive factors.
However, this information is of little use in the setting of a primary care consultation where the luxuries of endoscopic and histological knowledge are rarely available. For this reason, all patients who present to general practice with chronic symptoms of gastro-oesophageal acid reflux should be suspected of having a diagnosis of Barrett's and thus of being at high risk of developing oesophageal AC. The National Institute for Health and Clinical Excellence (NICE) recommends that endoscopic investigation should be considered for these patients if their symptoms persist despite H. pylori testing and acid suppression therapy. Patients with a confirmed diagnosis of Barrett's should be offered regular endoscopic surveillance screening to monitor for disease progression to high-grade dysplasia or intramucosal cancer.
Clinical features
A patient with oesophageal cancer will most commonly present with the symptom of dysphagia, which may be initially experienced with solid foods only, but often progresses to include liquids. Over half of all patients also present with weight loss, which is often due to a combination of carcinomatosis, and decreased nutritional intake due to dysphagia. Other symptoms include vomiting undigested food, haematemesis, odynophagia, epigastric pain, voice hoarseness (signifying likely tumour invasion of the recurrent laryngeal nerve) and respiratory symptoms such as cough and haemoptysis (signifying potential bronchial or tracheal tumour involvement).
On clinical examination, there are no pathognomonic signs to look for; in fact, the examination may be entirely normal. It is nevertheless important to conduct a thorough examination as there may be clear physical signs to signify advanced disease, such as cervical lymphadenopathy, palpable para-aortic lymphadenopathy, ascites, hepatomegaly due to metastases and Horner's syndrome suggesting invasion of the sympathetic chain.
Referral
A suspected diagnosis of cancer necessitates an urgent referral to secondary care for further investigation. Patients should be referred for an endoscopy under the 2 week wait referral system as set out by the 2005 NICE guidance on referral for suspected cancer (see Box 3). Symptoms that NICE recommends should trigger an urgent referral are
dyspepsia plus chronic GI bleeding
progressive unintentional weight loss
progressive dysphagia
persistent vomiting
iron deficiency anaemia or
an epigastric mass
Criteria for urgent investigation of dyspepsia with endoscopy
Patients of any age with new onset dyspepsia +
Chronic GI bleeding
Progressive unintentional weight loss
Progressive dysphagia
Persistent vomiting
Iron deficiency anaemia
Epigastric mass or
Abnormal barium meal
Patient presenting with or without dyspepsia +
Dysphagia
Unexplained upper abdominal pain and weight loss
Upper abdominal mass
Obstructive jaundice
Persistent vomiting and weight loss in the absence of dyspepsia
Unexplained weight loss
Iron deficiency anaemia
Patients aged 55 years and older with unexplained and persistent recent-onset dyspepsia alone should be referred urgently for endoscopy.
Routine endoscopic investigation of patients presenting with dyspepsia WITHOUT alarm symptoms or signs is not necessary.
Appropriate and timely referral is crucial to avoid diagnostic delay, which could adversely affect prognosis.
Diagnosis and staging
The first and most important diagnostic investigation for patients in whom oesophageal cancer is suspected is endoscopy and biopsy. In most cases, this will allow a definitive diagnosis to be made and is the method of investigation recommended by NICE. Further investigations routinely performed following diagnosis include staging computed tomography (CT), which may be combined with positron emission tomography (PET), endoscopic ultrasound (EUS) and laparoscopy. The information yielded from these tests will confirm the tumour size, the lymph node status and the presence or absence of metastatic disease and hence establish the stage of the tumour and determine viable treatment options.
Treatment options
The most effective way of organizing secondary care for major cancers in the NHS is through a multidisciplinary team (MDT) approach. Oesophageal cancer is no exception, and the MDT is especially important due to the complexity of the disease, with most patients requiring specialized imaging and often several modalities of specialist treatment. While patients are clearly assessed individually to plan their management options as a general guide patients with tumours of Stage I, II and often III (fitness allowing) can be offered surgery, while Stage IV tumours are usually limited to non-curative treatment options.
Surgery
For patients who are diagnosed with oesophageal carcinoma, complete surgical resection remains the single treatment option that is potentially curative and offers a chance of long-term survival. However, between 50 and 60% of patients are deemed unsuitable for radical resection due to either unresectable disease or lack of fitness to undergo the procedure. These poor statistics are explained by the late presentation of many patients due to their disease often being asymptomatic in its early (resectable) stages. Additionally, the nature of the symptoms increases the likelihood of a poor nutritional state and hence suboptimal preoperative general health.
It is generally agreed that patients with a tumour in the mid or lower oesophagus should be offered a subtotal oesophagectomy in order to decrease the likelihood of histological positive resection margins due to macroscopically invisible and non-palpable submucosal spread. Aggressive surgical treatment should have the primary goal of achieving complete resection of the tumour and its lymphatic drainage as this has been shown to be one of the most important prognostic factors. However, the likelihood of achieving this is in turn dependent on early presentation—the factor that is central to survival.
Despite improvements in surgical practice over the last 30 years, an oesophagectomy remains a major operation with significant risks and an average mortality of around 10% in skilled hands. This statistic emphasizes the importance of preoperative optimization, the two most significant features of which are correction of malnutrition and smoking cessation. Post-operative complications following an oesophagectomy are listed in Box 4.
Post-operative complications after oesophagectomy
General
Respiratory complications, e.g. pneumonia (25% of patients)
Thromboembolic complications
Myocardial ischaemia/infarction and cerebrovascular accident
Major haemorrhage (rare)
Specific
Anastamotic leak (2% of patients)
Chylothorax (2–3% of patients)
Recurrent laryngeal nerve damage
Gastric outlet obstruction
Acid reflux (common)
Anastamotic stricture (requires endoscopic dilatation)
Oncological treatment and palliative care
Oesophageal cancer frequently presents at a late stage and surgery alone has provided disappointing results. Over the last decade, there has been immense research interest into establishing the effectiveness of neoadjuvant chemotherapy in the preoperative management of these cancers. The interest has especially been focused on its impact on long-term survival, and results have shown survival is markedly prolonged with the addition of preoperative chemotherapy or chemoradiotherapy, despite the inevitable delay of surgery that this implies. This is largely due to downsizing of the tumour, downsizing of any lymphatic metastases and therefore an increase in complete resection rate. Chemoradiotherapy is also often used alone as treatment for patients who have been diagnosed with inoperable disease with the dual aim of alleviating symptoms and extending life.
To palliate means to focus on reducing symptom severity rather than disease cure and one of the worst symptoms to affect quality of life in patients with oesophageal cancer is dysphagia, the alleviation of which often proves challenging. Some of the more proven effective methods are brachytherapy (intraluminal localized radiotherapy to the tumour itself) and self-expanding metal oesophageal stents, in addition to the more conventional modalities of chemotherapy and external beam radiotherapy. The key to successful palliative care is an individualized approach and attention to symptom detail, and the patient's GP can be pivotal in this process. Furthermore, successful management of more common, but equally distressing, symptoms such as pain, nausea and constipation can make the difference between acceptable and intolerable quality of life during the terminal phase of the disease.
Gastric cancer
Although the incidence of gastric cancer is decreasing, according to Cancer Research UK, 7900 people are still diagnosed each year in the UK. It can be a difficult disease to diagnose due to non-specific symptoms at presentation and GPs need to have a high index of clinical suspicion, particularly in ‘at-risk’ individuals, in order to make a timely diagnosis and facilitate early and appropriate referral to secondary care.
Epidemiology and aetiology
Worldwide gastric cancer is the fourth most frequent cancer overall, with the highest incidences in China and Japan. Cancer Research UK puts gastric cancer as the 8th most common cancer in males in the UK and 13th in females; 95% of these cases are diagnosed in people aged over 50 years and 95% of gastric cancers are ACs. Proximal gastric cancers, particularly around the cardia, are far more common than distal gastric cancers.
The stomach is also the most common site for GI lymphomas, representing 3–6% of all gastric malignancies. The majority of tumours are B-cell non-Hodgkin's lymphomas, the most common being the mucosa-associated lymphoid tissue (MALT) lymphoma. These tumours arise from lymphoid tissue within the mucosa and are acquired as a result of H. pylori or H. heilmanni infection.
Gastrointestinal stromal tumours (GISTs) are a rare subgroup of tumours, which can arise in the upper GI tract. GISTs are soft tissue sarcomas of mesenchymal origin and represent 0.3–1% of all gut tumours. The remainder of this article will focus on gastric ACs.
Pathogenesis
The pathogenesis of gastric AC is multifactorial. Important risk factors are listed in Box 5.
Risk factors for developing gastric cancer
H. pylori
Male gender
Older age (more than 95% of cases diagnosed are in those aged 50 years and over)
Lower socio-economic status
Smoking
Alcohol
Poor diet
GORD (Barrett's oesophagus)
Previous gastric surgery, e.g. partial gastrectomy for ulcer
Pernicious anaemia
BMI greater than 27
First-degree relative with the diagnosis
There is evidence to support the Correa hypothesis, which states that there is a progression from chronic gastritis to gastric atrophy with intestinal metaplasia to dysplasia prior to malignant transformation. Infection with H. pylori is the most important known risk factor for any type of gastric cancer as it increases risk by 2-fold. The World Health Organization has listed H. pylori as a Class 1 carcinogen. It is responsible for inducing premalignant severe chronic atrophic gastritis, which later leads to AC. This risk increases with the severity of gastric atrophy.
Clinical features
Gastric cancer is complex, in that, it shares a symptomatic presentation, which is very similar to benign gastric pathology. A key role for the GP is to decide who requires urgent specialist referral for endoscopic investigation. History should confirm that the dyspepsia is new rather than a recurrent episode and exclude common precipitants such as new ingestion of non-steroidal anti-inflammatory drugs (NSAIDs). Symptoms include upper abdominal discomfort/pain, fullness or bloating, excessive flatus, nausea and also symptoms of anaemia. Observational studies indicate approximately 70% of patients with early gastric cancer (confined to the mucosa or submucosa, irrespective of lymph node invasion) present with benign sounding symptoms. As clinical diagnosis is inaccurate in distinguishing between benign and malignant disease, the aim of the consultation should be to detect patients with dyspepsia who are at risk. Symptoms of advanced disease with local or distant metastases include weight loss, vomiting, anorexia, jaundice and ascites.
Referral
The likelihood of gastric cancer increases when vague dyspeptic symptoms are present along with other ‘red flags’ symptoms such as weight loss, vomiting and anaemia. Patients should be referred as early as possible for investigation with gastroscopy and biopsy. A diagnosis of gastric cancer should be suspected in all patients with recent-onset unexplained dyspeptic symptoms that are over the age of 55 years. NICE guidelines on the management of dyspepsia in primary care and the referral criteria for urgent endoscopy are summarized in Box 4.
Diagnosis and staging
Once a histological diagnosis has been confirmed, the staging process must be completed to evaluate the extent of disease progression and plan optimal therapy. Staging with spiral computerized tomography (CT), magnetic resonance imaging (MRI), EUS and positron emission spectrography (PET) scans allows patients to be selected for specific approaches to treatment. Early identification of metastases can allow consideration of a palliative approach and avoid potential morbidity and mortality associated with unnecessary surgery.
Treatment options
Surgery
The aims of curative surgery are to excise the lesion with adequate resection margins and to remove local and regional lymph nodes. The most important factor affecting resectability and survival after surgery is the stage of disease when the patient presents. Early gastric cancer is a curable condition with more than 90% of patients surviving 5 years after treatment. The extent of resection is determined by the location of the tumour. The aim is to excise the tumour adequately while attempting to preserve as much stomach remnant as possible. Figures 2 and 3 show the gastric anatomy following a partial and total gastrectomy, respectively.

Gastric anatomy following partial gastrectomy. Billroth I refers to an operation in which the pylorus is also removed and the distal stomach is anastomosed directly to the duodenum.
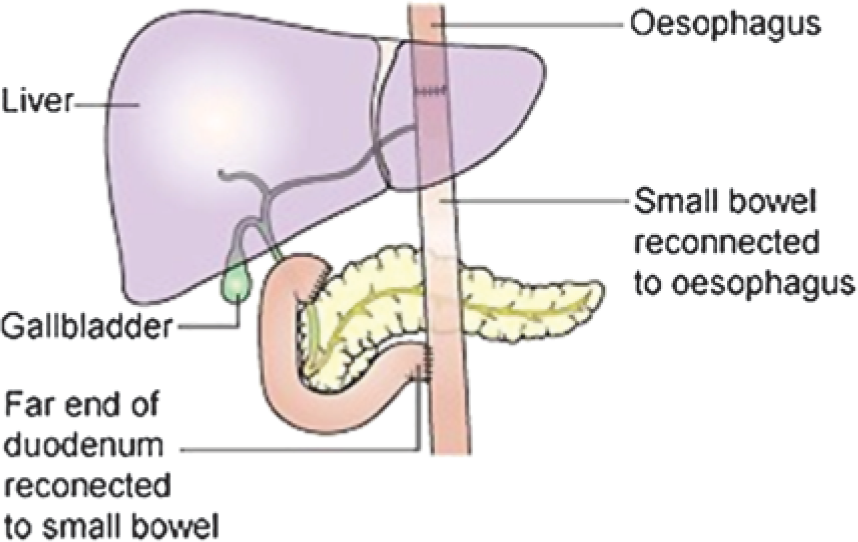
Roux-en-Y anastomosis following total gastrectomy. The stomach is removed and two new anatomoses are created: one between the oesophagus and small bowel and the second between the far end of the duodenum and small bowel.
Surgery is usually combined with neoadjuvant chemotherapy to reduce late patterns of disease recurrence following surgical resection. It can also be used to downsize tumours, which may be difficult to resect. Adjuvant chemotherapy is used in circumstances where operative difficulties have resulted in inadequate tumour resection or if patients are found to have more advanced disease, which had remained undetected at the preoperative staging.
Early complications following gastric resection include haemorrhage, anastomotic leak, intra-abdominal sepsis, pancreatic fistula (if removal of the tail of the pancreas has been carried out) and post-splenectomy infections (if a decision to remove the spleen was made). Late sequelae and complications can be divided into three groups:
side effects and postprandial sequelae
nutritional problems
recurrence of cancer
Loss of reservoir function of the stomach can result in early satiety and abdominal pain. Patients who have loss of pyloric function can be affected by early dumping syndrome, which refers to the rapid filling of the proximal small bowel causing movement of fluid into the gut from the extracellular fluid compartment. This can trigger a complex neurohumoral response that can produce unpleasant GI and cardiovascular symptoms. Other problems include diarrhoea, bile reflux and hypoglycaemic episodes. Weight loss and malnutrition are usually a problem in patients who fail to consume sufficient calories. This is most common in those who experience early satiety and dumping syndrome. Correction of symptoms and adequate dietetic input are crucial to correct malnutrition.
Palliative care
The high proportion of patients presenting with advanced disease reflects the high proportion of palliative treatment (surgical and non surgical) that is carried out. Palliative treatment options are discussed in the context of an MDT meeting and are shared with the patient. Those who are unsuitable for curative gastric surgery will usually require palliation of symptoms. Poor survival in these patients is directly related to primary tumour-related complications. The commonest of these include bleeding, gastric outlet obstruction and nutritional deprivation. Palliative triple combination chemotherapy is the main treatment option for patients with a good performance status and who agree to treatment.
Gastric outlet obstruction associated with incurable distal gastric cancer is difficult to manage as most patients are frail and nutritionally depleted. Treatment options include endoscopic stenting across the obstructive site and/or palliative chemotherapy. Fitter patients with a distal lesion who have a longer life expectancy can be considered for a surgical gastrojejunostomy. These patients have a loop of jejunum anastomosed close to the greater curve of the stomach so the stomach contents can bypass the obstruction. Subtotal gastrectomy is also used to palliate outlet obstruction in patients with a reasonable prognosis and it allows them to undergo palliative chemotherapy.
The role of primary care
Most patients will stay in hospital between 1 and 2 weeks following gastro/oesophagectomy with no major postoperative complications. However, it may take up to 9 months for them to make a complete recovery and for their quality of life to improve to an acceptable premorbid level. It is therefore important for GPs to be aware of the common problems that the gastro/oesophagectomy patient faces during this long recovery period.
Psychological considerations
The massive psychological impact of cancer is widely recognized and has been extensively researched, and hence, unsurprisingly, mental health problems such as depression and anxiety are extremely common among patients with oesophageal and gastric cancers. These patients are particularly vulnerable, mainly because of their significant physical symptoms such as anorexia, malnutrition and fatigue. These symptoms also contribute to the well-documented phenomenon of disappointment during the recovery period, which often increases as the time since surgery lengthens.
Despite being common in this group of patients and often one of the hardest problems to cope with, the symptoms and signs of depression are often missed. It is essential for GPs to consider the possibility of a diagnosis of depression when seeing these patients. Several authors argue that in order to alleviate psychological symptoms and enhance quality of life, physical symptoms should first be addressed and minimized. However, further management options may also be necessary such as counselling and/or antidepressants.
Nutrition
The role of the dietician, both in the hospital and in the community, is central to the care of patients with oesophageal and gastric cancer, and there are often several important nutritional issues to address. The patients usually have a poor baseline in terms of their weight for the reasons given earlier—the malignant process and poor oral intake. Furthermore, they are likely to lose more weight throughout the course of their disease and treatment. One of the main dietetic aims is to minimize this as much as possible. Patients with dsyphagia may require percutaneous endoscopic gastrostomy (PEG) feeding prior to surgery as their symptoms can worsen to the point where oral intake of anything is impossible. Should this be necessary, it is essential that the patient and their family are educated appropriately in order to enable them to operate the feeds and care for the PEG tube at home.
After their surgery, in order slowly to build up strength and increase weight, close monitoring of oral intake and an accurate record of the daily calorie count is vital. Commonly, patients report that a significant barrier to regaining weight is the loss of appetite that they experience as a result of the cancer itself, the surgery and also the many physical and logistical problems they encounter. Additionally, they often find eating more of an effort due to the loss of anatomical capacity to accommodate a full-sized meal. However, these patients need adequate nutritional intake. It is recommended that a problem-solving individualized approach be taken towards these issues, with the long-term goal of helping the patient to regain their appetite and some enjoyment from food.
After total gastrectomy, patients absorb virtually no vitamin B12 and body stores are gradually depleted (this may take up to 24 months to become clinically apparent). All patients should receive intramuscular hydroxycobalamin every 3 months for life. Vitamin D malabsorption is also a problem, particularly in post-menopausal women and long-term survivors. Disorders of calcium and vitamin D metabolism are common after total gastrectomy and oral supplementation should be used to prevent loss of bone mass.
Specialist and district nurses
It has been recognized that providing good nursing care to patients with oesophageal and gastric cancer is complex and involves the employment of many skills. The role of the upper GI clinical nurse specialist encompasses a wide and varied spectrum, but the underpinning theme is to be able to support patients through their diagnosis of cancer and the subsequent treatment, which is highly invasive, life threatening and life altering. The specialist nurse will usually consult with the patient both in partnership with the surgeon and MDT, and also individually, and is well placed to provide a continuity of advice, information and support for the patient and their family throughout their hospital journey. Often, because they are able to offer more time to each patient than the surgeon can afford, this gives the patient the opportunity to ask any forgotten questions from the medical consultation, air any suppressed concerns and discuss any points that they haven't entirely understood. Crucially, they can also act as a liaison point for GPs and other primary care health professionals for advice, support and ensuring continuity of care for the patient. District nurses equally play a key role in continuing this care upon discharge from secondary care. They are also well placed to observe and draw early attention to any problems that may arise.
Health promotion
There are a number of health promoting strategies that can help prevent oesophagogastric cancer from developing, either primarily or secondarily. As with so many other cancers, smoking cessation, reduction of alcohol ingestion, avoidance of obesity and encouraging a high intake of fresh fruit and vegetables are all strategies that could successfully reduce the incidence of oesophagogastric carcinoma. GPs are uniquely placed to undertake health promotion and it is an essential part of primary care, which should be encompassed within each relevant consultation. The aggressive treatment of GORD as a preventative strategy for oesophageal cancer is an attractive notion but for which the supportive evidence to date is lacking. However, if followed correctly, the NICE guidelines for GORD and dyspepsia will help to further identify those patients at an increased risk (i.e. refractory symptoms despite best medical treatment), and therefore those for whom further investigation or referral could be considered.
Screening
Another appealing concept is population screening for H. pylori infection to prevent gastric cancer, which has been recently considered by the UK National Screening Committee. They acknowledged that such a programme could indeed fulfil several of the essential criteria needed to implement population screening, such as the presence of a simple test, an effective treatment and potential cost-effectiveness. However, they concluded that currently more evidence is needed before it can be justifiably implemented in this country. Internationally, it remains a much debated issue as some leading international authorities in the field have already recommended the introduction of screening in high-risk populations (e.g. in certain high incidence areas in China). There have been community-based approaches to H. pylori screening and eradication reported which were associated with varying degrees of success. The emergent theme among their recommendations seems to be that certain population groups should be specifically targeted to maximize both cost-effectiveness and clinical impact. However, there are real concerns surrounding the lengthy delay before epidemiological benefits are evident, which was one of the main limitations identified by the UK National Screening Committee.
Key points
Gastric and oesophageal cancers are heterogeneous diseases with multifactorial aetiologies, which are currently associated with poor prognoses
The key to improving survival is early diagnosis so GPs should adopt a low threshold of clinical suspicion in high-risk patients; patients who present with new dyspepsia over the age of 55 years or with dyspeptic symptoms that fail to settle with medical management should be considered for further investigation.
Alarm symptoms, such as dysphagia, weight loss and iron deficiency anaemia should prompt urgent referral for endoscopy
Management of oesophagogastric cancer is multidisciplinary and often multimodal involving major abdominal surgery and chemotherapy
The recovery process is long and can be arduous due to problems such as depression, malnutrition and significant fatigue. These can be difficult for GPs to manage and specialist nurses can often be a helpful source of advice
Overall, the GP has a pivotal role to play for these complex patients, both in the primary referral process and in the working with secondary care clinicians to provide ongoing management.
Footnotes
Acknowledgements
V.C. is first author for the oesophageal cancer portion and M.P. is first author for the gastric cancer portion.