
Abstract
Consumption of alcohol has been an integral part of society since Neolithic times. Harmful alcohol use accounts for 4% of the total global disease burden. The annual estimated cost to the National Health Service (NHS) alone is £2.7 billion. Around 24% of the adult population in UK consumes alcohol to levels that are associated with potential or actual harm to their health and well-being, while 9% of men and 4% of women aged 16–74 years are alcohol dependent. This article seeks to address the identification, assessment and evidence-based management of harmful and dependent drinkers in the adult primary care population.
The GP curriculum and alcohol
Have an awareness of the physical, psychiatric and social manifestations of alcohol
Use appropriate alcohol screening tools
Differentiate between harmful drinking and alcohol dependency
Recognize the impact that undertaking brief interventions can have on reducing alcohol consumption to less risky levels
Have an understanding of the treatment options available, including pharmacological interventions
Establish and maintain a rapport with patients who have alcohol-use disorders, recognizing the challenging and erratic manner in which they may access health care
Engage patients in recognizing and defining the nature of their problem and involve them in management decisions
Work in conjunction with other agencies to deliver evidence-based interventions
Recognize the potentially stigmatizing nature of having an alcohol problem and how this may impact upon the doctor-patient relationship
In 2009, 8664 alcohol-related deaths were reported in the UK with the highest rates in men and women aged 55–74 years. These figures highlight the problem of alcohol misuse among older patients, a problem which frequently remains unidentified despite evidence that an increasing proportion of the over 65's now drink beyond the weekly recommended limits. Although most ethnic groups have lower levels of drinking compared to people from Caucasian backgrounds, levels of alcohol dependence are comparable. Alcohol consumption is escalating, most notably among Chinese men and Indian women. Irish men living in the UK are particularly over-represented with 34% drinking above recommended limits compared to 27% of the general British population. Evidence suggests that some ethnic groups are at greater risk of alcohol-related harm including Indian men and the Irish and Scottish. Sikh men appear disproportionately susceptible to cirrhosis.
Recommended alcohol limits
In the UK, one ‘unit’ of alcohol contains 8 g of ethanol. Figure 1 illustrates the number of units contained within some common alcoholic beverages.

Units of alcohol
The current Department of Health recommendations on ‘safe’ alcohol consumption are
Men should drink no more than 21 units of alcohol/week (and no more than 4 units in any 1 day)
Women should drink no more than 14 units of alcohol/week (and no more than 3 units in any 1 day)
The Royal College of Obstetricians and Gynaecologists advise that women who chose to drink during pregnancy should consume no more than 1–2 units once or twice per week.
The elderly are more vulnerable to the effects of alcohol due to physiological factors and extrinsic influences such as medication. In the USA, the over 65's are advised to consume no more than seven standard drinks per week or one drink per day. In the absence of specific guidelines in the UK, clinical judgement should be exercised when assessing alcohol consumption in older patients.
Classification of alcohol-use disorders
Harmful and dependent drinking are used as diagnostic terms in the World Health Organisation (WHO) ICD-10 classification. Box 1 lists the salient features of these diagnoses.
Identification and assessment of harmful drinking and alcohol dependence
Barriers to identification
Multiple patient and health professional factors contribute to the failure to identify many who are harmful drinkers or dependent on alcohol. Patients may fear stigmatization, resulting in under-reporting or concealment of their consumption.
This is particularly relevant in Asian communities where alcohol is often prohibited for religious reasons and alcohol misuse is refuted by older generations within the community. Moreover, the notion of ‘sensible’ drinking may not be deemed relevant in cultures where alcohol is forbidden. Many patients from ethnic minority groups are simply unsure of where or how to obtain help with their drinking. Patients from Irish communities typically have low consultation rates in primary care for alcohol-related problems, possibly reflecting perceived negative stereotyping by health professionals.
Features of harmful drinking and alcohol dependence
Harmful drinking
A pattern of alcohol use associated with damage to the physical (e.g. liver dysfunction) or mental well-being (e.g. depression secondary to excessive alcohol consumption) of the user. Although adverse social consequences are often present, this alone is insufficient to make the diagnosis.
Alcohol dependence encompasses a cluster of physiological, behavioural and cognitive phenomena in which the use of alcohol is of paramount concern to the individual.
A diagnosis of alcohol dependence requires that three or more of the following have been simultaneously present at some time during the previous year:
A compulsion to drink
Difficulties controlling drinking
Physical withdrawal symptoms if alcohol consumption ceases or declines (e.g. tremor, autonomic nervous system hyperactivity) or drinking to alleviate or prevent withdrawal
Development of a tolerance state; escalation of alcohol consumption is required in order to produce the same effect that was previously achieved at lower doses
Alternative pursuits that once held greater priority are neglected in favour of drinking and time spent recovering from the effects of alcohol
Persistent drinking despite evidence of harm
In the elderly, social isolation is also implicated due to difficulties in accessing health care. Furthermore, alcohol misuse may present non-specifically, e.g. through falls or cognitive decline, which is often attributed to the ageing process. Doctors may also be reluctant to ask older patients about their drinking due to a false perception that alcohol misuse is an affliction of younger generations.
Who should be screened and how?
NICE (2010a) recommends that alcohol screening should be routinely undertaken during patient encounters where health promotion is an integral component, e.g. new patient registrations or chronic disease management clinics. Alcohol misuse may manifest itself through physical, psychiatric or social problems, requiring GPs to be vigilant for additional screening opportunities. Box 2 lists presentations where the involvement of alcohol should be considered.
The 10-item Alcohol Use Disorders Identification Test (AUDIT) questionnaire was devised by WHO for use in primary care and is regarded as the ‘gold standard’ alcohol screening tool. It performs consistently across a range of cultures. The final score determines whether the patient's drinking is classified as sensible, hazardous, harmful or possible dependency. Abbreviated forms of AUDIT also exist, e.g. AUDIT-C and FAST. Further information on screening for harmful drinking can be found in another article (‘Prevention of harmful drinking’) in this issue of InnovAiT.
Clinical presentations where the involvement of alcohol should be considered
Alcoholic hallucinosis
Depression
Anxiety
Cognitive impairment, e.g. memory problems, dementia
Repeated deliberate self-harm
Treatment resistance in co-morbid psychiatric illness and as a factor in relapse
Marital problems, domestic violence
Drug abuse
Forensic history, e.g. driving offences
Unplanned pregnancy
Financial difficulties
Child neglect
Repeated absenteeism
Frequent sick note requests
Impaired work performance and accidents
Poor employment record
Some studies have shown the CAGE questionnaire to be superior to AUDIT at identifying dependent drinkers as the questions focus on lifetime experiences of alcohol use:
Have you ever felt that you should
Have people
Have you ever felt bad or
Have you ever had a drink first thing in the morning to steady your nerves or get rid of a hangover? (
At scores of 2 or above, CAGE has a sensitivity and specificity of 43–94% and 70–97%, respectively, for detecting alcohol dependency. Biological markers of alcohol consumption such as mean cell volume (MCV) and gamma glutamyl transferase (GGT) are not routinely recommended screening tools but may help to motivate change and monitor consumption over time.
Further assessment
AUDIT is inadequate as a standalone instrument for detecting alcohol dependence since dependence exists in a spectrum of severity. Therefore, identification of possible alcohol dependence should prompt further assessment with a dedicated questionnaire such as the Severity of Alcohol Dependence Questionnaire (SADQ-C). The 20 items of the SADQ shown in Box 3 cover various aspects of dependency, including physical withdrawal symptoms, affective withdrawal symptoms, relief drinking, frequency of alcohol consumption and the rapidity with which withdrawal symptoms develop.
Categorizing alcohol dependence as mild, moderate or severe has important implications for where assisted withdrawal is conducted. In the context of older patients, much lower levels of consumption may trigger the dependence threshold.
Once the diagnosis has been confirmed, the context and wider impact of the patient's alcohol misuse should be explored as this may inform ongoing management. This is particularly pertinent in older patients since most screening tools have not been specifically designed for use in the elderly. Box 4 lists additional information which should be sought.
Management principles in harmful drinking and alcohol dependence
Research has consistently shown that higher intensity interventions are no more effective than less intensive options. NICE (2011) recommends the use of community-based interventions to promote abstinence or moderate drinking and prevent relapse. Treatment intensity may need to be escalated for those with limited social support, complex physical or mental health needs or those unresponsive to initial interventions.
Figure 2 provides a broad overview of the nature and intensity of interventions appropriate for each level of alcohol misuse.

A spectrum of response to alcohol problems.
The Severity of Alcohol Dependence Questionnaire (SADQ-C)

Components of further assessment
Drinking history:
Quantity, frequency and pattern of consumption
Dependence severity
Alcohol-related problems
Co-drug use
Physical or mental health co-morbidities
Risk of harm to self or others
Treatment urgency
Motivation or readiness to change
Sociodemographic features
Relevant physical examination and investigations
Treatment goals
The ultimate goal of treatment in alcohol misuse remains a contentious issue. Increasingly, drinking in moderation is regarded as an acceptable target at harmful and even mildly dependent levels of alcohol consumption providing that adequate social support is available and no medical or psychiatric contraindications exist. Abstinence should be strongly advocated for the majority of dependent drinkers and in the presence of alcohol misuse with associated co-morbidities. While goal setting will largely be governed by clinical factors, the patient's acceptance of the goal must also be established as this will be an important determinant of adherence.
Extended brief interventions and motivational interviewing
Extended brief interventions are recommended for those individuals who have failed to respond to brief advice or in the case of dependent drinkers, where brief advice alone is insufficient as a standalone intervention (see InnovAiT article on ‘Prevention of harmful drinking’ for information on brief advice). The technique of motivational interviewing is commonly employed in delivering extended brief interventions and can be applied to both the initiation and the maintenance phases of treatment. In primary care, extended brief interventions would normally be undertaken by a GP with a specialist interest who has received appropriate training in motivational interviewing (e.g. the proposed RCGP Alcohol Certificate Part 2).
Motivational interviewing encompasses four key principles:
Expressing empathy
Developing discrepancy
Rolling with resistance
Supporting self-efficacy
Presenting the patient with reasons as to why they should modify their drinking behaviour may provoke contradictory arguments within the patient, resulting in perpetuation of drinking. The ‘interviewer’ therefore adopts a non-confrontational approach, using empathy to create an environment conducive to change. The patient is required to delineate the problems that their drinking causes and the reasons why abstinence would be beneficial. This perceived discrepancy between the patient's present behaviour and their treatment goal is then magnified as a means of enhancing patient motivation. Any resistance exhibited by the patient should not be countered but instead used to advantage. The session should culminate with the patient feeling empowered to make change. Ideally, sessions should last 20–30 minutes with follow-up to assess response.
Motivational enhancement therapy (an adaptation of motivational interviewing) ranks number two after brief interventions in the Mesa Grande project, a systematic review that ranks the effectiveness of interventions for alcohol misuse (Miller and Wilbourne, 2002). Project MATCH (Project MATCH Research Group, 1997) found that motivational enhancement therapy delivered over four sessions was as effective as treatment modalities requiring 12 sessions such as cognitive behavioural therapy (CBT).
Individual self-help and mutual aid groups
Although engagement in formal treatment increases the prospects of recovery, a range of additional resources are available to patients in the form of books and web-based self-help. They can be utilized as an adjunct to treatment and during relapse prevention.
Self-help manuals (‘bibliotherapy’) are aimed at harmful drinkers or mildly dependent drinkers. Individuals who have difficulty accessing alcohol treatment services or fear stigmatization may find this approach more acceptable. Most self-help manuals and web-based programmes are based on CBT principles and aim towards a goal of drinking in moderation. They are therefore inappropriate for most dependent drinkers. Bibliotherapy ranks fifth in the Mesa Grande (Miller and Wilbourne, 2002) and has been shown to be effective on both clinical and economic grounds.
All patients should be provided with information on how to access mutual aid groups such as Alcoholics Anonymous (AA) or SMART Recovery. AA is ubiquitous and well established within the UK. The tenet of AA is that alcoholism is an incurable disease, which requires a lifelong commitment to abstinence. ‘The Twelve Steps’ underpins AA's code of principles and practice and contains several references to the existence of ‘a higher power’.
Established members are encouraged to support new recruits and help them attend meetings where ‘recovering alcoholics’ recount their personal stories. The strong spiritual overtone to AA's teachings combined with the candidness required to disclose personal details to others are common reasons why patients are deterred from attending. Elderly people may also have difficulty accessing groups due to physical barriers or concerns that they may not ‘fit in’. While the nature of AA does not lend itself to evaluation in randomized controlled trials, studies have clearly demonstrated an association between frequency and duration of participation in AA and long-term abstinence (Moos and Moos, 2004, 2006).
SMART Recovery (Self Management and Recovery Training) has evolved as an alternative to AA and challenges the belief that alcoholism is incurable. Rather, alcoholism is regarded as a learned behaviour that can be changed using cognitive behavioural techniques. SMART is based on a four-point programme incorporating motivation to abstain, coping and urges, problem solving and lifestyle balance and is delivered on-line and through face-to-face meetings. Unlike AA, SMART's foundations are underpinned by scientific evidence.
The impact that an individual's alcohol misuse can have upon the family unit should not be overlooked. Box 5 lists a range of national alcohol support agencies for patients and their families.
National Alcohol Support Agencies
(Tel: 0800 9178282)
Offers free advice on private rehabilitation and outpatient programmes
Offers support services ranging from counselling and therapeutic interventions to practical advice on housing and employment
Safety and legal aspects
Safety-netting is a key component of patient management. The perils associated with abrupt alcohol cessation must be stressed, particularly in the alcohol dependent.
Many patients will be unaware of the driving restrictions imposed by the Driving and Vehicle Licensing Agency (DVLA). Table 1 lists the DVLA regulations for Groups 1 and 2 licence holders. The General Medical Council (GMC, 2009) has issued clear guidelines for doctors reporting concerns about patients to the DVLA:
DVLA regulations on alcohol misuse
Ensure the patient understands that their condition may impair their ability to drive
Explain that they have a legal duty to inform the DVLA of their condition
If the patient does not accept this, suggest a second opinion and advise them to abstain from driving in the interim
If the patient still continues to drive, make every reasonable effort to persuade them to stop (this may necessitate involving a family member with the patient's consent)
If this fails, disclose medical information to the DVLA after the patient has been notified of the intended course of action
Safety issues surrounding the patient's occupation (e.g. use of machinery), family circumstances (e.g. caring for dependents) and leisure activities (e.g. swimming) may also need to be addressed. Patients should also be encouraged to enlist the support of family, friends and work colleagues as the presence of a supportive social network will not only enhance patient motivation but also reduce the likelihood of accidents.
Referral for alcohol misuse
Referral to specialist alcohol services should be considered for moderate or severe alcohol dependence, those who have failed to benefit from an extended brief intervention but still require further help and patients who exhibit severe alcohol-related impairment or co-morbidities. As part of the referral process, patients should be advised that a considerable amount of their treatment can be shared with primary care.
Evidence suggests that elderly patients are at least as likely to benefit from treatment as younger patients. However, a multidisciplinary approach may be more appropriate in the presence of complex physical or cognitive needs. This may necessitate the involvement of physicians or psychogeriatricians, social services and community-based agencies.
Currently, there are few dedicated alcohol services for minority ethnic groups despite evidence that these patients are most disadvantaged in terms of access to alcohol treatment. Preferences with respect to the type of support offered vary widely with some patients favouring mainstream service provision over specialist minority ethnic services. Regardless of the approach, treatment should be delivered with cultural sensitivity to address the specific needs of this diverse group.
Psychological interventions for harmful drinking and mild dependence
Psychological therapies are the mainstay of treatment for harmful drinkers and those with mild alcohol dependence. NICE (2011) has incorporated CBT, behavioural therapies and social network and environment-based therapies into its treatment recommendations. A detailed appraisal of the various interventions is beyond the scope of this article but the salient points are outlined below.
The application of CBT is based on the premise that alcohol misuse is a maladaptive behaviour that becomes entrenched as a means of dealing with difficult situations. CBT aims to provide coping strategies to help counteract the triggers that lead to drinking. Several techniques are utilized under the umbrella of CBT including social skills training and relapse prevention. The nomenclature is varied and overlaps with behaviour-based therapies.
Social network and environment-based therapies exploit the patient's environment as a means of achieving abstinence or controlled drinking. The development of a social milieu supportive of change is the principle underlying social network therapy. This intervention was developed for the United Kingdom Alcohol Treatment Trial (UKATT Research Team, 2005) and was found to be as effective as motivational enhancement therapy, albeit more expensive. The community reinforcement approach entails a family member (usually the spouse) providing positive reinforcement for abstinence. This positive reinforcement (e.g. access to television) is withdrawn if the patient reverts to drinking.
CBT, behavioural therapies and behavioural couples therapy should ideally be delivered as one 60 minute session/week for 12 weeks. Social network therapy is optimally delivered over 12 weeks consisting of eight 50 minute sessions.
Assisted alcohol withdrawal
Assisted withdrawal aims to attenuate the severity of withdrawal symptoms associated with abrupt alcohol cessation after prolonged heavy consumption. It is just one component of a much broader treatment programme for alcohol dependence. A significant minority will successfully complete an assisted withdrawal programme and remain abstinent for a period of time thereafter. Dependent drinkers are far less likely to succeed without help and are at risk of developing complications, such as withdrawal seizures, delirium tremens and Wernicke's encephalopathy.
Patient selection and preparation
Careful patient selection and preparation are aprerequisite to a successful assisted withdrawal. Individuals who drink more than 15 units of alcohol a day and/score 20 or more on AUDIT should be assessed for their suitability to undergo community-based assisted withdrawal. Indications for inpatient or residential withdrawal are listed in Box 6.
Criteria for inpatient and residential-assisted withdrawal
Referral for inpatient or residential-assisted withdrawal should be considered if one or more of the following criteria are met. They:
drink more than 30 units/day
score more than 30 on the SADQ-C
have a history of epilepsy OR a previous assisted withdrawal attempt complicated by delirium tremens or withdrawal seizures
are co-dependent on alcohol and benzodiazepines
regularly drink between 15 and 20 units of alcohol/day and have:
significant psychiatric or physical co-morbidities-significant learning disabilities or cognitive impairment
The elderly, homeless or socially isolated trigger a much lower threshold for admission
Adequate social support should ideally be available for the duration of the withdrawal process but particularly during the first few days. Providing the patient and carer with written information about the type of symptoms to anticipate (e.g. tremulousness, sweating, insomnia, anxiety, nausea) and practical advice for coping with the period of withdrawal (e.g. re-scheduling work commitments, relaxation skills) is likely to increase compliance.
Conducting assisted withdrawal
Chlordiazepoxide remains the benzodiazepine of choice for patients undergoing assisted withdrawal. Diazepam is a suitable alternative but has greater potential for abuse. Chlormethiazole is not recommended due to the attendant risk of respiratory depression when combined with alcohol.
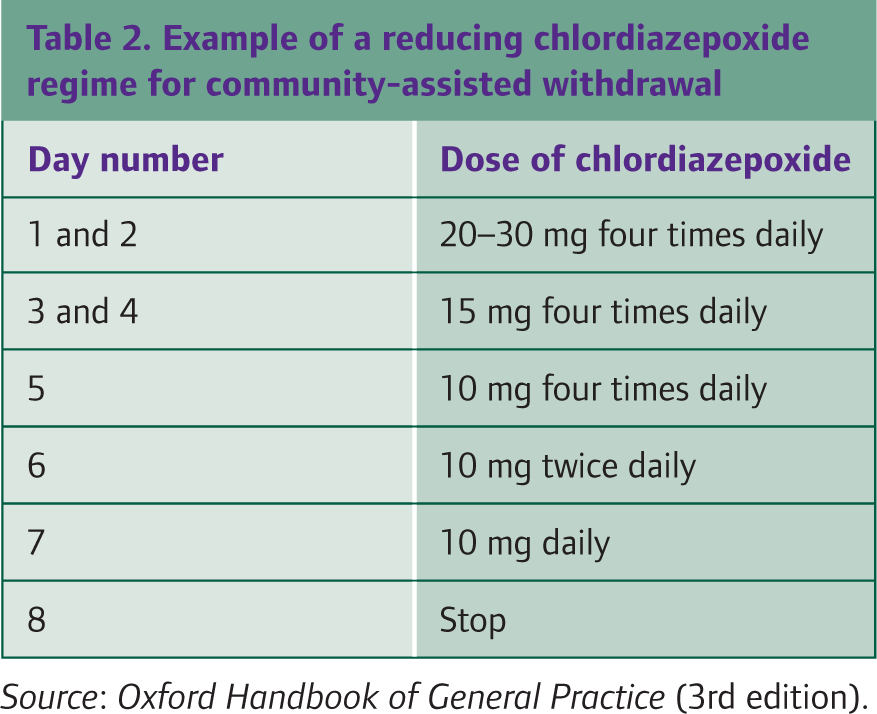
Although symptom-triggered withdrawal regimens have been shown to be more effective and patient centred, they lack the practicality and safety of fixed dosing. Patients undergoing community-based withdrawal should therefore be prescribed fixed-dose medication regimens whereby the starting dose of benzodiazepine is titrated according to dependence severity. The dose is then gradually reduced over 7–10 days. The British National Formulary (BNF 61, 2011) recommends starting with 10–50 mg of chlordiazepoxide four times a day. However, doses in excess of 30 mg should be reserved only for the severely dependent. Protocols are often determined locally but an example of a typical regimen is shown in Table 2.
Example of a reducing chlordiazepoxide regime for community-assisted withdrawal

Safety-netting includes dispensing of benzodiazepines in 2 day instalments to reduce the risk of overdose and ensuring that administration of medication is supervised. Ideally, patients should be monitored by a health care professional on alternate days to assess for the severity of withdrawal symptoms and the development of complications. A breathalyser may be used to monitor compliance, with a positive reading necessitating termination of the assisted withdrawal process.
Thiamine and Wernicke's encephalopathy
Wernicke's encephalopathy is a well-recognized neuropsychiatric complication in alcohol-dependent patients who are deficient in thiamine. Susceptibility is enhanced during alcohol withdrawal. Thiamine may be depleted through inadequate nutritional intake, reduced absorption and impaired utilization. Oral prophylaxis should therefore be prescribed to harmful or dependent drinkers in the following circumstances (NICE, 2011):
Questionable nutrition
Decompensated liver disease
Acute alcohol withdrawal
Before and during planned-assisted withdrawal
It is common practice to prescribe 200–300 mg of oral thiamine/day (in divided doses) along with one to two tablets of vitamin B Co-strong three times daily. Thiamine is required at least 2 weeks prior to starting assisted withdrawal and may be indicated for a variable period of time following completion. Since oral thiamine is poorly absorbed, the BNF recommends considering parenteral thiamine (Pabrinex) for high-risk patients receiving treatment in primary care. In contrast, NICE (2010b) advocates its use solely in selected hospital patients. Although Pabrinex carries a small risk of anaphylaxis, the risk is diminished further if given intramuscularly. Nevertheless, anaphylaxis drugs should still be available when it is administered.
A high index of suspicion for Wernicke's encephalopathy is crucial as the classic triad of confusion, ataxia and opthalmoplegia is only present in around 10% of patients. The presence of additional symptoms and signs such as hypothermia, hypotension, memory disturbance and persistent vomiting warrant urgent medical referral. Untreated Wernicke's encephalopathy may rapidly progress to Korsakoff's psychosis. This devastating condition is characterized by amnesia and confabulation and is associated with high rates of institutionalization.
Relapse prevention
Following successful withdrawal, patients with moderate to severe dependence should receive a pharmacological intervention to reduce the risk of relapse. Acamprosate and naltrexone are the agents of choice, although naltrexone is not currently licensed in the UK for this indication. Disulfiram has recently fallen from favour due to the lack of evidence for its efficacy but its use may be warranted if other alternatives are unsuitable. While most prescriptions will be initiated by specialist alcohol services, acamprosate can be commenced in primary care following community-based withdrawal. As GPs may be required to oversee the maintenance phase of treatment, a familiarity with the agents listed in Table 3 would be advantageous.
Pharmacological interventions for relapse prevention
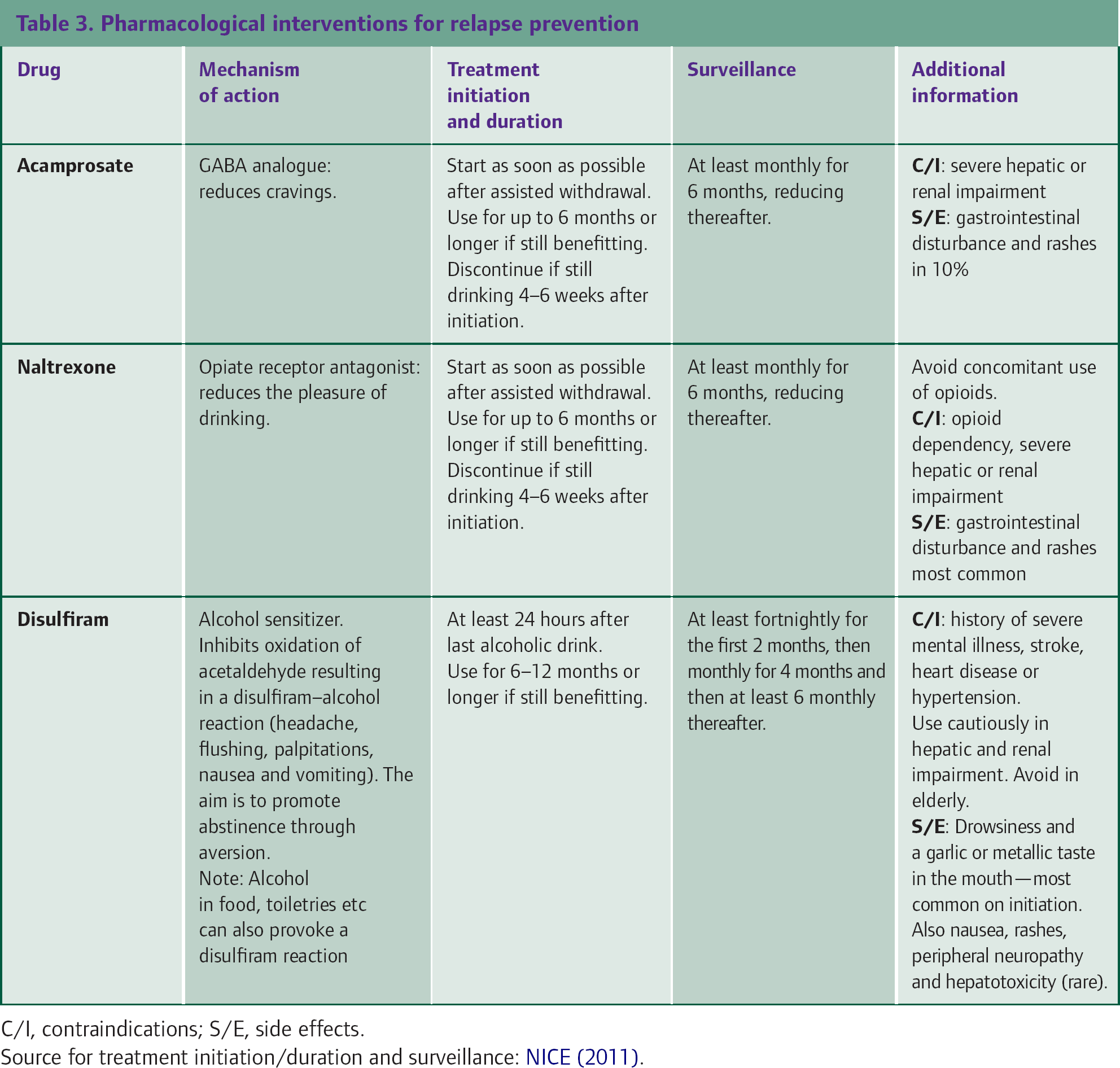
Pharmacotherapy should be used as an adjunct to the psychological interventions aforementioned. Following discharge from the care of specialist alcohol services, patients will require continued monitoring in primary care. Ideally, contact should be maintained with the same health care professional via telephone calls or brief consultations for at least 3 years. These low-intensity measures have been shown to reduce the severity of relapses.
Key points
GPs should be alert to the multiplicity of presentations associated with alcohol misuse
Barriers to identification and treatment are commonplace in the elderly and ethnic minority groups
Detection of possible dependency requires further assessment to determine severity and the extent of any associated co-morbidities
Psychosocial interventions are the mainstay of treatment for harmful and mildly dependent drinkers
Patients undergoing community-assisted withdrawal require careful selection, preparation and monitoring
Relapse prevention combines pharmacological and psychological interventions with long-term, low-intensity follow-up.