
Abstract
Endometriosis is a common and debilitating gynaecological problem affecting up to 50% of premenopausal women presenting to general practice in the UK. It is characterized by the presence of endometrial glands and stromal tissue in locations other than the uterine cavity. Common associations include pelvic pain, dysmenorrhoea, dyspareunia and sub-fertility although clinical investigation findings do not always correlate well with the degree and severity of symptoms. The impact on quality of life for women with severe symptoms results in GPs playing a central role in diagnosis and managing physical, mental and social aspects of the condition. This article aims to provide an overview of current guidelines and strategies for recognizing and managing endometriosis in general practice.
The GP curriculum and endometriosis
Demonstrate knowledge of women's health problems, conditions and diseases
Demonstrate a reasoned approach to the diagnosis of women's symptoms in a manner that is comfortable for both the patient and the GP using history, examination, incremental investigations and refer appropriately
Discuss the psychosocial component of women's health and the need, in some cases, to provide women patients with additional emotional and organizational support
Describe and implement the key national guidelines that influence health care provision for women's problems
Communicate sensitively with women about sexuality and intimate issues
Evaluate the effectiveness of the primary care service you provide from the female patient's point of view
Incidence and burden
The prevalence and resultant burden of endometriosis remain difficult to assess as many women will remain asymptomatic despite the presence of the condition. Conversely, many women with pelvic pain may have no evidence of endometriosis at laparoscopy. The prevalence in asymptomatic women may be anywhere between 2 and 50% depending on the population and modality of diagnosis. Little verified data exist on the financial burden of endometriosis in this country. ‘Endometriosis UK’ estimates that of those women with symptoms, 82% have had some difficulty carrying out day-to-day activities and 38% have had problems with work due to their symptoms. The society therefore suggests that up to £2.8 billion is lost annually to the economy in sick days alone.
Pathophysiology
Several theories for the pathogenesis of endometriosis have been proposed. The exact cause, however, remains unknown. Retrograde menstruation through the fallopian tubes, which was first described in 1927 remains the predominant theory. Other theories include lymphovascular spread of endometrial tissue to distant sites, metaplasia of epithelium into endometrial type tissue and immune—genetic defects which predispose to the proliferation of endometrium from embryonic cells at sites distant to the uterine cavity.
Endometriosis can cause lesions anywhere in the pelvis and on the peritoneum, although it is most commonly seen on the ovary where lesions can vary in size from small spots of disease to large endometriomas or ‘chocolate cysts’ containing haemolysed blood. The uterosacral ligaments and pouch of Douglas are commonly affected. The serosal surface of the uterus may also be involved along with the bowel, bladder and ureters. Deposition of endometrial tissue in these areas can lead to chronic inflammation and fibrosis, which in turn can cause adhesions and distortion of pelvic anatomy. Less common but important sites include abdominal scars, the umbilicus and in rare cases distant sites such as the thoracic cavity.
Just as normal endometrium responds to hormonal changes, so do endometrial lesions elsewhere. As endometrial tissue proliferates in response to oestrogen, pain at the sites of lesions may worsen, giving rise to the classical premenstrual worsening of pain in endometriosis.
How will endometriosis present in general practice?
Many women may not know that they have endometriosis. This may be due to a lack of symptoms, although poor knowledge of the condition and reluctance to seek help may also play a part in under-diagnosis. The common symptoms that women may present with are displayed in Box 1. Women are of reproductive age and their predominant symptom is long-standing pelvic pain. Pain that is cyclical in nature makes the diagnosis of endometriosis more likely. Severe dysmenorrhoea may also be the only presenting symptom in a significant proportion of women.
Common symptoms suggestive of endometriosis
Cyclical premenstrual pelvic pain
Dysmenorrhoea
Deep dyspareunia
Painful defecation
Painful micturition
Infertility
The site of the lesion does not always correlate with symptoms; however, fixed retroversion of the uterus by Pouch of Douglas lesions, for example, may be associated with deep dyspareunia. Painful defaecation or dysuria may also be features. Chocolate cyst rupture can lead to a chemical peritonitis causing acute exacerbations of abdominal pain. More rarely, patients may develop bowel obstruction or obstructive uropathy as a complication of endometriosis.
An association with sub-fertility compounds the morbidity associated with endometriosis. Up to 30% of cases of sub-fertility involve underlying endometriosis and it therefore remains an important underlying consideration for GPs who see couples finding it difficult to conceive even if the woman is asymptomatic. Hence, early recourse to diagnostic intervention may be considered in a sub-fertile patient who has pelvic pain.
Pelvic examination should be offered to all women where endometriosis is suspected. Adnexal tenderness, tenderness in the posterior fornix or a fixed retroverted uterus may all be clinical features. Deeply infiltrating nodules may be palpable through the posterior vaginal wall. Deep infiltrating bluish nodules may also be visible on speculum examination through the vaginal wall. Pelvic examination may, however, yield no positive findings even if symptoms are severe.
Diagnosis
Before considering the diagnosis of endometriosis, it is important to rule out other important causes of pelvic pain. These are listed in Table 1. Women should be considered for pregnancy testing to exclude ectopic pregnancy if pain is acute in onset. Pelvic inflammatory disease is another important condition not to be missed and assessment should include sexual history and routine screening for sexually transmitted infections.
Differential diagnosis in pelvic pain

With these factors in mind, the eventual diagnosis of endometriosis can be problematic because presentation is variable and the degree of symptoms may not correlate well with extent of disease. The Royal College of Obstetricians and Gynaecologists (RCOG) suggest that there is often a delay of up to 12 years from onset of symptoms to definitive diagnosis. Although the clinical features can point towards diagnosis, direct visualization under laparoscopy remains the ‘gold-standard’ diagnostic test (RCOG, 2006).
The Revised Classification of the American Society of Reproductive Medicine can be used to grade endometriosis I—IV based on findings at laparoscopy and is shown in Box 2. This grading system assesses the extent and location of lesions although it is important to recognize that this scoring system does not indicate the severity of symptoms for the patient. Histological confirmation is recommended to confirm the diagnosis but if negative does not rule out endometriosis.
ASRM revised classification of endometriosis
Findings restricted to only superficial lesions and possibly a few filmy adhesions
In addition, some deep lesions are present in the Pouch of Douglas
As above, plus presence of endometriomas on the ovary and more adhesions
As above, plus large endometriomas, extensive adhesions
There is a role for pelvic ultrasound in the investigation of other underlying pathologies that may be causing pelvic pain, such as ovarian cysts (including endometriomas) and fibroids, although it is not sensitive for endometriosis. Magnetic resonance imaging (MRI) is occasionally used to image the pelvis and can be helpful in planning major surgery where bowel or ureteric involvement is suspected. MRI has not been shown to be superior to laparoscopy in the diagnosis of endometriosis. Serum cancer antigen-125 (CA-125) levels can be raised in endometriosis and have been used for research purposes but are not cost effective to measure in clinical practice where levels bear no relationship to severity of symptoms.
When to refer?
Endometriosis is difficult to diagnose clinically and further investigation is often required to confirm the diagnosis. If a GP suspects the condition, referral to secondary care for further investigation is indicated; however, this should not delay appropriate medical therapy. Symptoms of endometriosis may overlap with other conditions such as irritable bowel syndrome and establishing an accurate diagnosis with laparoscopy guides ongoing clinical management. It is important to counsel women prior to referral and in particular explain that they may have to undergo surgery to help establish the underlying cause of their symptoms.
‘Red flag’ symptoms that should prompt urgent referral to secondary care for pelvic pain include:
Bleeding per rectum
New bowel symptoms over 50 years of age
New pain after the menopause
Pelvic mass
Suicidal ideation
Excessive weight loss
Irregular vaginal bleeding over 40 years of age
Post coital bleeding (RCOG, 2005)
Management
An individualized and patient-centred approach to management is essential. Treatment decisions depend on severity of symptoms, plans for future fertility and tolerance of side effects. Good counselling is essential to ensure that women can make informed choices about their treatment.
As symptoms are chronic and often physically and mentally debilitating, a multidisciplinary approach is also vital to successful management of the condition. GPs therefore play a central role in coordinating vertical integration of care for patients where close communication with specialists in secondary and tertiary care in planning management and follow-up is crucial.
It is also important for GPs to consider the obstacles that face women with chronic pelvic pain ahead of visiting the GP surgery. The prospect of discussing a very personal problem with their doctor can create huge anxiety. The intimate nature of examination can further exacerbate anxiety for some women. It is important to ensure that vaginal examination is carried out with particular attention paid to privacy and confidentiality. A chaperone should always be offered. Improvements in practice organization may improve access for women with pelvic pain and dysmenorrhoea; for example, sign-posting patients to GPs with expertise in women's health may result in a better patient experience.
With these key points in mind, the management of endometriosis can be considered in three categories: medical, surgical and supportive therapy (summarized in Table 2).
Management of endometriosis
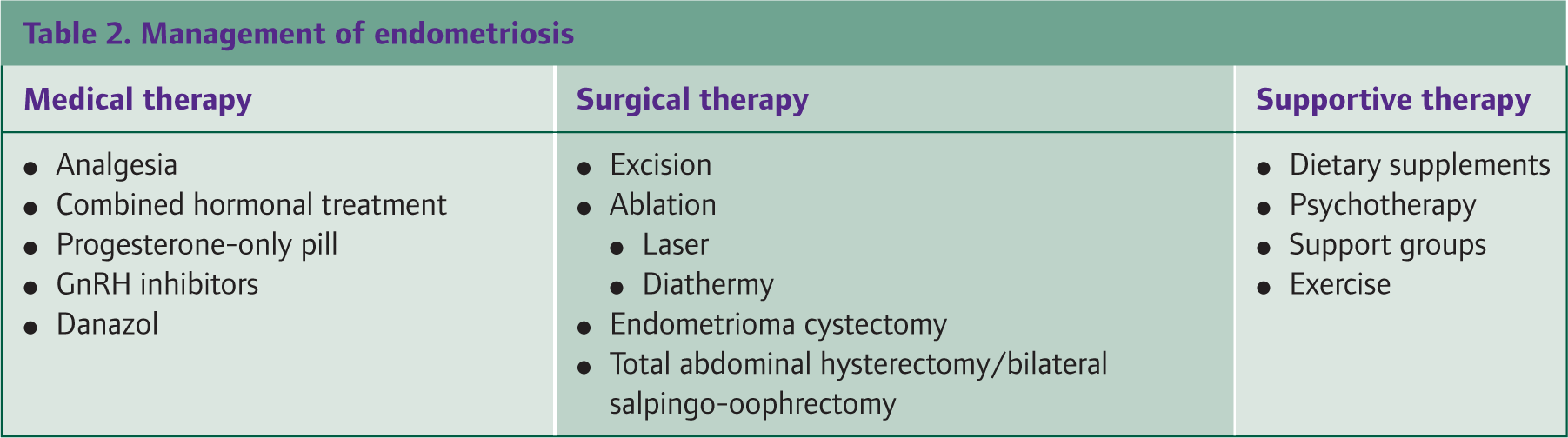
Medical therapy
Empirical medical therapy should be considered if endometriosis is suspected clinically before a definitive diagnosis is made (RCOG, 2006). This includes provision of simple analgesia and hormonal therapies, which can be initiated in general practice.
First-line analgesia should be guided by symptoms and patient preference. It is important to counsel women about adverse or unwanted effects of analgesia. Pelvic pain can be managed initially with paracetamol and non-steroidal anti-inflammatories (NSAIDs). If dysmenorrhoea is a predominant symptom, then mefenamic acid may be effective. Tranexamic acid may also be helpful if menorrhagia is a particular feature. Cyclooxygenase-2 (COX-II) inhibitors may be considered if first-line analgesia is ineffective or poorly tolerated.
Unfortunately, response to treatment with simple analgesia is variable and may be ineffective in pelvic pain associated with endometriosis. Agents such as amitrptyline or pregabalin for neuropathic pelvic pain should only be initiated following specialist confirmation of diagnosis (National Institute for Health and Clinical Excellence, 2010).
The main aim of hormonal therapy is to suppress ovarian function. Therapies include progesterone-only preparations and combined oral contraceptives. If symptoms are particularly severe, continuous or tricyclic regimes of hormone therapy may be used but their effectiveness is uncertain so these treatments need to be tailored to patient response and side effect profile. Factors such as high body mass index, smoking status and age may also influence the eligibility of patients for medical treatment.
The levonorgestrol intrauterine system (Mirena) may also be helpful in improving symptoms for some patients with endometriosis. It is already a well-established treatment for menorrhagia and has been shown to be of some benefit in patients with endometriosis. It is advantageous in that, if effective, it can be used long term in women who are not trying to conceive. It is not always effective, however, with a proportion of women experiencing troublesome ‘breakthrough’ intermenstrual bleeding.
Gonadotrophin-releasing hormone (GnRH) analogues play an important role in the management of symptoms. Response to these treatments is much the same compared to other hormonal preparations and concerns about effects on bone mineral density and menopausal type side effects limit their use to a usual maximum of 6 months. Treatment with GnRH analogues may be extended, however, with the use of ‘add-back’ therapy where small doses of progesterone, oestrogen or tibolone (a synthetic steroid which mimics oestrogen and progesterone) may improve the side effect profile of therapy. Danazol may also be used for ovarian suppression although it has a limited duration of use and can be associated with significant side effects, such as weight gain, bloating and an adverse effect on lipid profiles. GnRH analogue therapies are only initiated in a secondary care setting.
Although helpful for initial control of symptoms, all medical therapies are associated with incomplete resolution of pain or relapse of symptoms following treatment cessation. Recurrence rate estimates vary but suggest that up to 50% of women will have recurrence of painful symptoms within 12–24 months following therapy.
Surgical therapy
Laparoscopy forms the mainstay of accurate diagnosis of endometriosis. Before undertaking surgical treatment of the condition, however, careful preoperative assessment should be performed including full informed consent. Pelvic ultrasound assessment and magnetic resonance imaging may also be necessary. As disease may be multifocal, severe and sometimes deeply infiltrating, surgical treatment should be undertaken in a centre with the necessary multidisciplinary surgical expertise. This involves surgeons trained in advanced laparoscopy as well as laparotomy.
Surgical therapy is effective for many women. Lesions can be excised or ablated with laser therapy or diathermy. Adhesions can be treated with adhesiolysis and chocolate cysts can be drained and stripped. Two double blind randomized controlled trials reported outcomes in terms of pain and quality of life scores for women who underwent either laser ablation or excisional surgery compared to diagnostic laparoscopy or placebo alone (Sutton et al., 1994; Hawe et al., 2004).
Total abdominal hysterectomy and bilateral salpingo-oophrectomy may also be considered as surgical treatment options that may improve symptoms. The decision to proceed with these interventions may be guided by factors such as age, co-morbidities, parity and above all patient choice. Hormone replacement therapy is recommended for young women who undergo bilateral oophrectomy. Despite positive outcomes in a large proportion of cases, symptom recurrence remains common either as a result of incomplete surgical excision or as a postoperative disease recurrence.
There is significant controversy surrounding the management of sub-fertility in endometriosis. Surgical treatments such as ablation of lesions, division of adhesions and tubal flushing have been shown to improve chances of conception and possibly aid assisted conception in mild to moderate disease. The role of surgery in improving fertility in severe disease, however, remains uncertain. In vitro fertilization is recommended as an appropriate treatment, particularly where there is coexisting tubal dysfunction or male factor infertility.
Supportive therapies
The complex lifestyle challenges faced by women with endometriosis should not be underestimated. They may struggle in completing day-to-day activities and face difficulties at work. Relationships can also be affected by psychosexual dysfunction and infertility. Chronic symptoms may result in coexistent anxiety or depression. Women who have persistent symptoms despite medical and surgical therapies may turn to alternative therapies, dietary interventions, counselling and support groups to find coping strategies. It is important for GPs to signpost patients to helpful sources of information.
Few trials have looked at dietary supplementation to relieve pelvic pain. One randomized controlled trial reported some possible benefit in vitamin E supplementation for patients with primary dysmenorrhoea (Ziaei et al., 2001).
Similarly, no studies exist looking at psychotherapy in the context of pelvic pain; however, counselling, group-based therapy or cognitive behavioural therapy (CBT) may be helpful for some women to come to terms with the complex physical and emotional difficulties they face while coping with endometriosis. A Cochrane review has demonstrated some small positive effects of CBT on chronic pain, mood and disability (Eccleston et al., 2009). It is vitally important that GPs discuss these issues with women and direct them to appropriate local services. GPs also play an important role in recognizing and treating coexisting depression and anxiety.
Women may also report improvement with alternative therapies, such as acupuncture and reflexology. Despite the absence of an evidence base and lack of National Health Service (NHS) provision for these treatments, some women may find them helpful.
Further support and guidance may be found through Endometriosis UK, the largest UK-based support group for women that provides patient information through newsletters, a helpline and local support groups. Endometriosis.org also provides an extensive online international source of information, which can inform both patients and clinicians of updates in evidence and best practice. It also provides a list of support groups throughout the world.
Key points
Endometriosis is a common cause of pelvic pain, dysmenorrhoea and dyspareunia
There is an association between endometriosis and infertility
Diagnosis can be considered with a classical history of cyclical pain in primary care though laparoscopy remains the gold standard test
Endometriosis should be managed holistically with a multidisciplinary approach
Analgesia and simple hormonal medical therapies can be initiated in a general practice setting prior to formal diagnosis
Surgical treatments are commonly effective and should be carried out at centres with appropriate advanced laparoscopic services