
Abstract
Every year, 250 000 people experience burns in the UK, 175 000 will attend an emergency department and 13 000 will require admission to hospital. Burns are usually accidents, often due to carelessness or inattention, but they may also be associated with alcohol or drug abuse or related to a pre-existing medical condition. The key role of the GP is to oversee patient care from initial first aid provision to rehabilitation and to be aware of when it is appropriate to refer to secondary care, including specialist burns units.
The GP curriculum and burns
Burns are listed as an important condition in
Initiate management of the patient who has been burnt Be aware of the safety of the patient and medical staff at the scene of the incident Be aware of how to summon help in an emergency Be competent in reducing pain with the use of analgesia or other methods Recognize referrals requiring emergency action to save life or prevent serious long-term sequelae Understand the roles of allied health professionals (nursing, physiotherapy, occupational therapy, counselling and psychological services) Consider chronic disease management including systems of care, multidisciplinary teamwork and shared-care arrangements
Almost all adults will have personal experience of a burn at some point. The majority of these burns are minor and can be managed with prompt first aid in the community, but up to 50% will suffer some restriction of daily activity as a result of being burned (British Burns Association, 2001). The home is the most common location where adults and children are likely to be burnt. The kitchen and bathroom are most frequently associated with scalds, while the laundry and garden shed may contain corrosive substances, which can cause chemical burns or flammable liquids which may cause thermal burns.
Causes
Burns can be divided into four broad aetiological categories: thermal, inhalation, electrical and chemical. Thermal injury is most common. Table 1 summarizes the aetiology and associated features of each type of burn and management strategies for chemical and electrical burns.
Aetiology of burns, associated features and management

Pathophysiology
A burn can be described by three pathological zones as first proposed by Jackson in 1953 (Fig. 1).
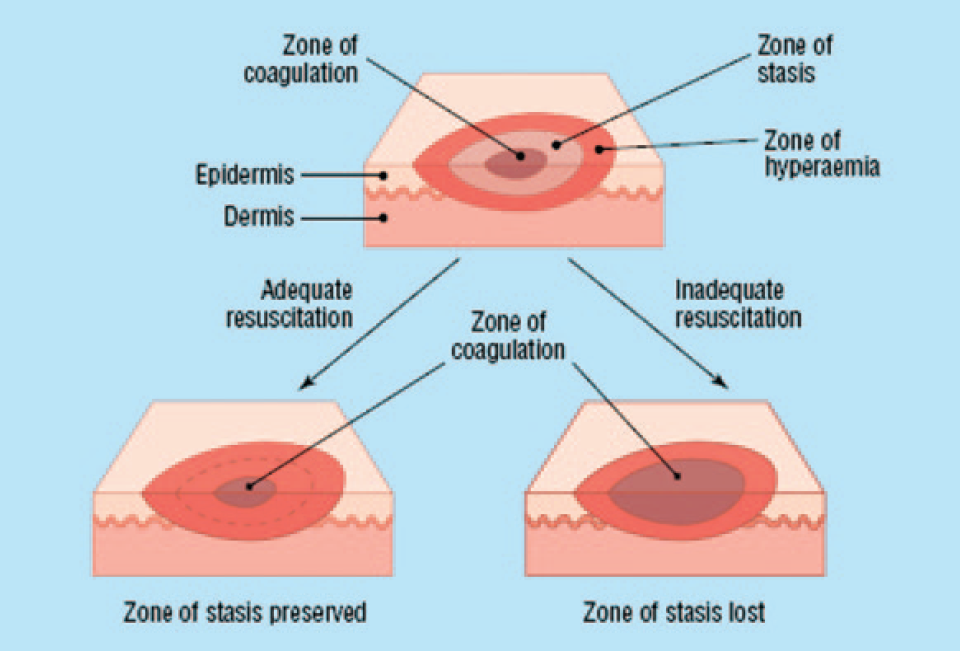
Jackson's burn zones and the effects of adequate and inadequate resuscitation.
Zone of coagulative necrosis
The zone of coagulative necrosis is the point of maximum damage where the heat cannot be conducted away. Irreversible tissue death occurs due to coagulation of constituent proteins.
Zone of stasis
The burn injury in the zone of stasis causes damage to the microcirculation and resultant decreased tissue perfusion. Tissue in this zone may progress to necrosis due to release of inflammatory cytokines but is potentially salvageable with early resuscitation. Prolonged hypotension, oedema or infection may cause this zone to progress to an area of complete tissue loss.
Zone of hyperaemia
The zone of hyperaemia is the outermost area affected. It represents increased tissue perfusion in response to injury with inflammation, cytokine release and increased blood flow. In smaller burns, the tissue in this zone will return to normal after the hyperdynamic vascular response has resolved. In burns over 20% total body surface area (TBSA), this zone may include the whole body.
Depth
Burns are usually classified as superficial or deep according to the depth of tissue damage; however, there may be a combination of both within the wound. Fig. 2 illustrates the layers and structures, which are present in normal skin.

Skin histology diagram.
Superficial burns
Superficial burns have the ability to heal spontaneously by epithelization. They can be sub divided into epidermal burns and superficial dermal burns.
Epidermal burns only affect the epidermal layer. The stratified layers are burned and complete healing occurs from regeneration of the basal layer. The skin is classically erythematous due to inflammatory mediators producing hyperaemia, but no blisters are present. These burns are initially painful but the pain typically ceases after 48–72 hours. They usually heal within 7 days, leaving no scar. Pure erythema is not included in percentage TBSA calculations.
Superficial dermal burns extend through the epidermis into the superficial part of the dermis. They are characterized by pink erythematous blisters as shown in Fig. 3. The skin covering the blister is no longer viable and is separated from its living base by inflammatory oedema. Sensory nerve endings are exposed and therefore, the burn is extremely painful. Superficial dermal burns usually heal spontaneously within 14 days, leaving a colour match defect but no long-term scarring.

Sperficial dermal burn of a patient's neck and back, showing pink skin with erythematous blisters.
Deep burns
Deep burns are more severe. They are less likely to heal spontaneously or by epithelization and may heal after a prolonged period with significant scarring. They can be sub divided into deep dermal burns and full-thickness burns.
Deep dermal burns may have some blistering but are blotchy red in colour, due to extravasation of haemoglobin from destroyed red cells leaking from ruptured vessels as shown in Fig. 4. The burn destroys the dermal vascular plexus and surrounding nerve endings and so sensation will be dull or absent.

Deep dermal burn of a patient's arm and torso shows areas of pale insensate skin with surrounding erythema.
Full-thickness burns destroy both epidermis and dermal layers. Deep underlying structures may also be affected.
There are no blisters, they are leathery dense white or possibly charred black (known as an eschar). Blood vessels and sensory nerve endings are completely destroyed. Sensation and capillary return are absent.
Management
History and examination
It is essential to take a history of the incident with particular attention to mechanism (blast or explosions may lead to co existing injuries), time course and location (enclosed spaces suggest possible inhalation injury). If known, the causative agent will give an indication of whether the burn is likely to be superficial or deep. If inconsistencies are noted between the appearance of injury and history, be suspicious of non-accidental injury and refer to a burns unit for further investigation.
The burn should be carefully examined and appearance recorded. Note:
The colour Area involved Presence or absence of blistering Capillary return Level of pain Any exudate and its nature Presence or absence of surrounding inflammation suggesting sepsis
Burn area
Burn severity is determined by the area and depth of a burn. The likelihood of mortality is calculated using the patient's age and %TBSA burnt.
The %TBSA affected by a burn can be easily estimated using the' Wallace rule of nines'. The body is divided into areas of 9% and the total burn area can be calculated as shown in Fig. 5. This has been modified for children as they have proportionally smaller hips and legs and larger shoulders and heads than adults. Smaller burns can be estimated using the surface area of the patient's palm (from wrist to fingertips), which equates to approximately 1% of TBSA. It is important to remember that erythema is not included in these estimations.

Wallace's rule of nines.
Alternatively, Lund and Browder charts can be used which are more accurate than the rule of nines. They are useful across all age groups, particularly in children as they take into consideration the patient's age and body proportions. Charts are required, however, to make these calculations.
Small partial thickness burns less than 10% TBSA are compatible with out-patient management. This may be in the GP setting or in conjunction with an out-patient clinic at the local hospital. Intravenous fluid resuscitation is required in children with greater than 10% TBSA and adults with greater than 15% TBSA burns and therefore requires referral to a burns unit.
First aid
The principles of first aid are to remove the burning source, stop the burning process and to cool the burn wound (Hudspith and Rayatt, 2004). Stopping the burning process reduces tissue damage. Cooling the surface of the burn is extremely effective analgesia, reduces the inflammatory reaction and can prevent further necrosis in the zone of stasis.
Hot charred clothing should be removed as quickly as possible. Similarly, with scalds, wet clothing should be removed as soon as possible as it can act as a reservoir for heat. If clothing is tightly stuck to the patient, cut it away from the edge of the burn leaving the remaining adherent fabric in place.
Cool the burned surface with cold running water for 20 minutes, ideally at 15°C (8–25°C is acceptable). Sponging the wound is quite effective if running water is not available. Wet towels are less efficient as they heat up, and if used, they must be changed frequently (Yuan et al., 2007). Do not use ice or iced water; this increases vasoconstriction and experiments have suggested that it may deepen the injury (Sawadal et al., 1997). It also leads to a greater risk of hypothermia. Small children are at particular risk of becoming hypothermic due to their increased surface area to body mass ratio. It is very important to keep the rest of the child (or adult) wrapped up warm and if required, raise the ambient room temperature. If more than 3 hours have elapsed since the time of injury, there is no benefit to applying cold water.
With chemical burns, it is important to be aware not to injure the patient further. Wearing thick rubber gloves and cutting off contaminated clothing prevents spread. Follow this by washing with copious amounts of water. With electrical burns, try to isolate the power source; if this is not possible, use an electrically insulated tool to move the patient away from the current source.
Covering the burn, preferably with a clean cotton sheet (sterile if available) or preferably polyvinyl chloride film (cling-film) helps limit evaporation and hence heat loss. A transparent covering enables the wound to be reviewed and it can be easily removed as it is non-adhesive. Ensure dressings are not circumferentially constrictive as this may compromise circulation to the wound. Do not apply any topical creams or agents such as silver sulfadiazine as these can alter the initial assessment of burn depth. If a limb is affected by the burn, elevate where possible to help limit swelling.
Considerations in primary care
Analgesia
When appropriately dressed, small burns can usually be managed with oral analgesia titrated in a step-wise fashion according to the patient's needs. If pain is not well controlled and narcotics are required, consider admission to hospital for interim treatment. Pain is usually most severe during dressing changes and physiotherapy. Consider oral opioid analgesia 30–45 minutes before these activities are undertaken. Dressings of burns in children can cause considerable distress. A familiar face to provide distraction with toys during a dressing change can be helpful.
Wound care
Manage burns with the same principles as any wound, taking care to avoid further tissue damage. Aseptic technique minimizes the risk of contamination. Wash the burn with soap and water and then remove any loose skin with sterile scissors. Small blisters can be left intact. If blisters are greater than 1 cm across, consider bursting and de-roofing with scissors as the skin will be dead and insensate; this procedure will prevent re-accumulation of fluid which is a possible medium for bacteria (Hudspith and Rayatt, 2004).
Once the area has been cleaned and debrided, it is essential to re-examine the wound as the depth can change with time. Always be alert for evidence of surrounding inflammation suggestive of infection. Antibiotics are not routinely required but it is important to make sure tetanus immunizations are up to date.
Dressings
There is little evidence about the best dressing to use in the management of burns. However, it is generally accepted that keeping the wound environment moist is a key feature in optimal wound healing; therefore, plain gauze is not widely used (Hudspith and Rayatt, 2004). Advice should be provided by the hospital if a specialist opinion has been requested. For epidermal and superficial dermal wounds managed solely in the community, simple non-adhesive dressings such as silicone [Mepitel® (Mölnlycke)] followed by padded gauze are most effective. Other non-adhesive dressings such as dressing gauze impregnated with paraffin [Jelonet® (Smith and Nephew)] are a suitable alternative but are more prone to drying.
Hydro-colloids [Comfeel® (Coloplast), DuoDERM® (ConvaTec)] are suitable for superficial dermal or small areas of deep dermal burns and particularly useful in difficult areas such as elbows, heels and digits. Semi-permeable plastic films [Opsite® (Smith and Nephew), Tegaderm® (3M)] are suitable for superficial or superficial dermal burns with minimum exudate. Advantageously, they allow for visual checks and may be left in place for 2–3 days but should not be used for infected or heavily exuding burns.
Silver sulfadiazine hydrophilic creams [Flamazine® (Smith and Nephew)] are widely used as topical agents. The silver ions act as a broad-spectrum antimicrobial agent, with the additional benefit of keeping the wound well hydrated. They should not be used in early treatment of superficial burns as they make burn depth assessment very difficult due to staining of the wound. They should be reserved for deep dermal burns. When in use, silver sulfadiazine creams should be changed on alternate days until any eschar has lifted and there is evidence of epithelization.
Further layers of gauze padding, wool, and crepe in a' figure of eight' fashion, secured by tape will help prevent movement and shearing forces of the dressing layers below. Examine the burns 48 hours after initial dressing and reassess the depth of wound. They can then be reviewed every 3–5 days providing there was no prior soakage of dressings, evidence of infection or malodour and the patient is relatively pain free.
When applying bandages, care must be taken to ensure that they are not applied too tightly. It is important to ensure fingers and toes are left exposed so sensation and circulation of limbs can be assessed at regular intervals. Limbs should be elevated in a sling or on pillows to encourage resolution of dependent oedema.
Referral guidelines
The British Burn Association has identified a list of injuries that are known to predict a complex clinical course (Box 1). All patients with these injuries should have early consultation with a burns unit.
Surgery
A circumferential full-thickness burn can compromise circulation by acting like a tourniquet. It may therefore become necessary to surgically release the constriction by surgically incising down to subcutaneous fat with cutting diathermy or scalpel. This procedure is known as an escharotomy. Light dressings are required to cover the area once the incision is performed. Split-thickness skin grafting may be required for deep dermal or full-thickness burns. The department where these procedures are performed should arrange follow-up in their out-patient/dressing clinic.
National burn injury referral guidelines

Multi disciplinary approach
Minor burns to anatomical areas such as hands, wrists, elbows, axilla and neck are prone to hypertrophic scarring and contractures. These patients should be referred to physiotherapists and occupational therapists as soon as possible. Exercises, pressure garments, adhesive tape and silicone therapy can help to minimize functional limitation. Those patients with persistent contracture and skin shortage may require referral for secondary surgical treatment.
Considerable cosmetic disability can occur after burns have healed. Colour match defects and irregular wound contours post skin grafting can lead to disturbance in body image. The availability of a psychiatrist specializing in body image disorders is limited outside major burns centres and the third sector is often the main source of support. Camouflage makeup preparations like Derma Blend can provide excellent results and there are many centres throughout the UK, being run by charitable organizations like The British Red Cross, which have trained volunteers to teach its application. The charity Changing Faces also provides support for those with facial disfigurement. The GP is the cornerstone of a multi disciplinary team approach to promote confidence and independence for these patients and their families post-burn injury.
Key points
There are 250 000 burns/year in the UK; the majority are avoidable Many minor burns can be adequately treated in the community with initiation of prompt first aid Appropriate dressings changed in a timely manner facilitate normal healing and help prevent complications Referral to a burns unit may be required to prevent long-term sequelae Secondary referral of healed minor burns may be required for physiotherapy, psychotherapy, scar management and surgical reconstruction