
Abstract
Aretaeus, a Greek physician and disciple of Hippocrates first coined the term diabetes, which means siphon in Greek. He described the disease as ‘melting down of the flesh and limbs into the urine’. There was no treatment available until insulin was discovered in 1921 by Banting and Best. Diabetes is the second most common chronic disease in childhood after asthma. Around 25% of newly diagnosed children present with diabetic ketoacidosis (DKA). Chronic hyperglycaemia can lead to long-term complications. The role of the GP is to diagnose children early in their presentation to prevent DKA, refer them to the multidisciplinary diabetes team, coordinate care in the community and provide advice regarding management during day-to-day activities.
GP and diabetes in children
Be able to manage primary contact with children and families Have a sound knowledge base of chronic diseases in children such as diabetes Coordinate care with other primary care professionals, paediatricians and other appropriate specialists, leading to effective and appropriate care provision, taking an advocacy position for the patient or family when needed Provide longitudinal continuity of care as determined by the needs of the patient and family and support young people with a chronic disease and their parents to negotiate the process of transition Manage conditions which may present early and in an undifferentiated way and be able to recognize a seriously ill child and intervene urgently when necessary
Manage primary contact with patients who have diabetes mellitus Coordinate care with other primary care health professionals, such as diabetes nurse specialists, dieticians, district nurses, community matrons, chiropodists and opticians to enable chronic disease management Be able to recognize the common symptoms of diabetes, interpret the investigations and understand the principles of treatment in primary care and management of diabetic emergencies
Definition
Diabetes mellitus is a group of metabolic diseases characterized by chronic hyperglycaemia resulting from defects in insulin secretion, insulin action or both. This leads to abnormalities in the metabolism of carbohydrates, protein and fat. The symptoms and signs of hyperglycaemia include polyuria, polydipsia and weight loss.
Prevalence and types of diabetes
Diabetes is more common in the developed world. In 2009, the International Diabetes Federation estimated that there are around 480 000 children (0–14 years) with diabetes worldwide. Around 70 000 children are diagnosed with diabetes every year and the incidence is increasing at around 3.4% per year. Finland, Sweden and Denmark have the highest rates of type 1 diabetes in the world. There are approximately 23 000 children and young people with diabetes in England (Royal College of Paediatrics and Child Health, 2009). In the National Diabetes Audit 2008–2009, nearly 30% of the patients were found to have poor long-term glucose control and 7.6% of the patients experienced at least one episode of diabetic ketoacidosis (DKA) during 1 year.
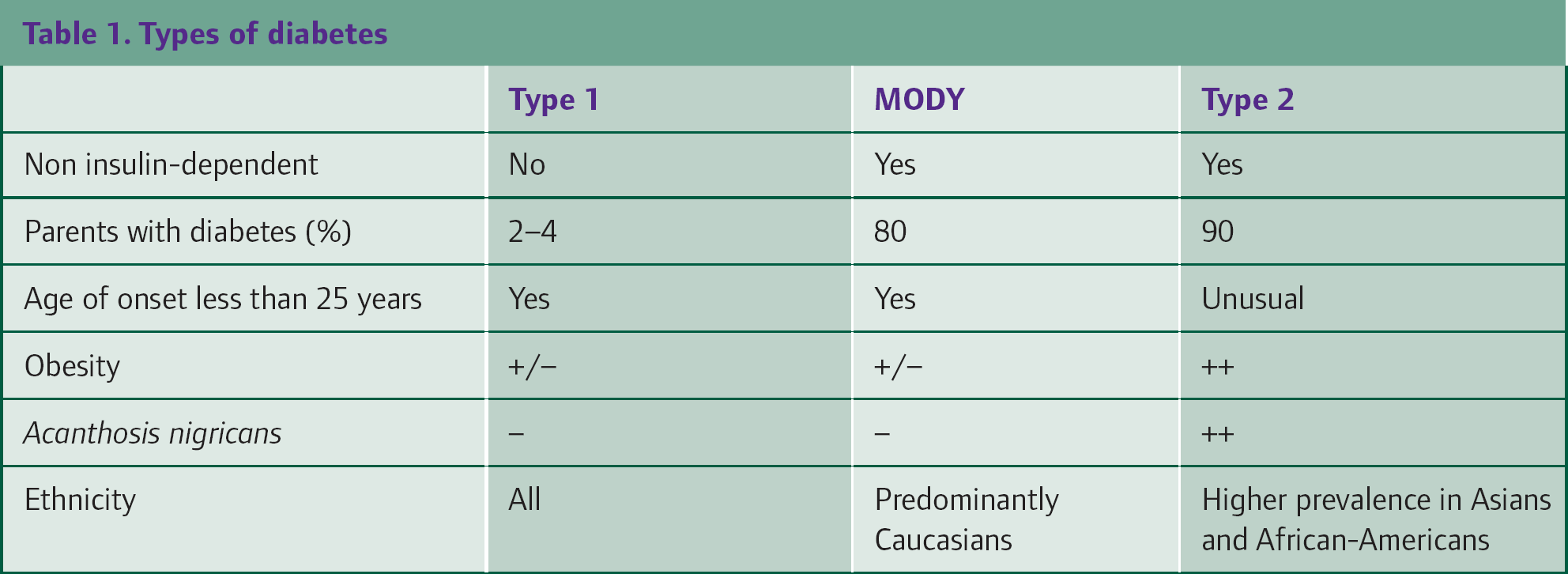
The American Diabetes Association (ADA) and World Health Organization (WHO) expert committees have classified diabetes into various types. Type 1, type 2 and monogenic diabetes, previously known as Maturity Onset Diabetes of Young (MODY), are the three major types described in children and young people. The predominant form of diabetes in children is type 1 diabetes. Ninety seven per cent of children with diabetes have type 1, 1.5% have type 2 and 1.5% have other types of diabetes. Peak prevalence of all types of diabetes is found to be in the age group over 10 years.
Though the prevalence of type 2 diabetes is less common in children, it is rising steadily due to increasing rates of obesity. Around 10% of the children with type 2 diabetes have insulin autoantibodies. A strong family history of diabetes is often also present.
MODY is less common and is diagnosed in children by genetic testing following the discovery of several genetic mutations which cause the disease. MODY3 is due to a mutation in the HNF1A gene and accounts for 70% of all MODY. This is inherited in an autosomal dominant fashion and is seen in non-obese children. These children require very low doses of insulin to maintain normoglycaemia and can also respond well to sulfonylurea treatment. The important differences between the three main types of diabetes affecting children are shown in Table 1.
Types of diabetes
Pathophysiology
Type 1 diabetes occurs primarily due to T-cell-mediated pancreatic islet b-cell destruction, which is an autoimmune process and susceptibility is genetically determined. Autoantibodies to islet cells (ICA), insulin (IAA) and other cellular components (GAD65, IA-2 and ZnT8) are present in 80–90% of patients with the disease. The inheritance of both HLA antigen DR3 and DR4 increases the risk of development of diabetes by 10- to 15-fold. Though there is a strong genetic component, environmental factors such as viral infections and toxic chemicals may also contribute. Risk of developing type 1 diabetes is higher in identical twins or siblings of the patient. The risk is increased 30-fold if both parents have diabetes.
Natural history
The natural history of type 1 diabetes is characterized by:
Preclinical diabetes Presentation of diabetes Partial remission or honeymoon phase Chronic phase of lifelong dependency
Characteristics of preclinical diabetes
Islet cell autoantibodies (ICA) Glutamic acid decarboxylase (GAD) autoantibodies Tyrosine phosphatase (IA-2) autoantibodies Insulin autoantibodies
HLA DR3—DQA1*0501—DQB1*0201 (susceptible genotype) HLA DR4—DQA1*0301—DQB1*0302 (susceptible genotype) HLA DR2—DQA1*0102—DQB1*0602 (protective genotype)
Viral infections (congenital rubella and enteroviral infection) Toxic chemicals Cereals Low levels of vitamin D and lack of vitamin D supplementation in early life
Impaired first phase insulin release on glucose tolerance test (defined as an insulin response less than the 10th percentile for age- and sex-matched controls) confers a 60% risk over the next 5 years
Preclinical diabetes
Children are usually asymptomatic during the months or years before initial presentation with type 1 diabetes. This period is called preclinical diabetes. During this period, antibodies can be detected against different components of b cells and genetic markers may also be present. Children with immunological markers, genetic markers and impaired insulin response following glucose tolerance test are at increased risk of developing diabetes. There are a number of potential factors which can trigger diabetes in susceptible individuals (Box 1).
Screening and following up patients at high risk can help in early diagnosis of diabetes. The role of GPs is vital in identifying and screening high-risk patients when they visit for other reasons. In the Diabetes Prevention Trial, when high-risk individuals were followed, 63.3% of participants who were diagnosed with diabetes were asymptomatic (Triolo et al., 2009).
Presentation of diabetes
The classical presentation of a child with diabetes includes a history of increasing polyuria, polydipsia and weight loss over a period of 6–8 weeks. The onset of symptoms is slow in some children while it is rapid in others who may present with DKA. The usual and emergency presentation of symptoms is given in Table 2. Most of these symptoms are non-specific and can potentially lead to misdiagnosis. A high index of suspicion is necessary when children present for the first time to the GP. Failure to consider the possibility of diabetes results in late diagnosis and increased risk of DKA. Atypical presentations also delay the diagnosis and initiation of treatment. Children and young people with suspected type 1 diabetes should be offered immediate (same day) referral by the GP to a multidisciplinary paediatric diabetes care team that has the competencies needed to confirm diagnosis and provide immediate care.
Presentation of diabetes

Partial remission or honeymoon phase
After establishing the diagnosis and initiating insulin treatment, the insulin requirements may decrease transiently in approximately 80% of patients. This is known as the partial remission phase, which can start as early as a few days after commencing treatment. During this period, patients show good glucose control with less insulin requirements (less than 0.5 units/kg/day) and have glycosylated haemoglobin (HbA1c) of less than 7% indicating good long-term glucose control in spite of variations in diet and exercise. Few children and adolescents will be able to maintain normoglycaemia without insulin therapy for a period of time. This phase can last for weeks or months and it is important for GPs to advise parents and children that this is only a transient period and does not mean complete remission of diabetes.
Chronic phase of lifelong dependence to insulin
The partial remission phase progresses gradually to the chronic phase. This is due to a further decrease in the functioning islet cells with time leading to lifelong dependency on insulin. This can be further accelerated by any intercurrent illnesses and infections. Glucose control will depend on the exogenous insulin administration during this chronic phase.
Prevention of the disease
At present, there are no proven strategies or interventions to help prevent or delay diabetes in high-risk patients or their first-degree relatives. Oral or subcutaneous insulin therapy given to high-risk patients or their relatives has been tried unsuccessfully (Diabetes Prevention Trial Type 1 Diabetes Study Group, 2009). Screening of any population or intervention in the preclinical phase is not recommended currently, except for research purposes.
Diagnosis and management
Diagnosis is based on presentation of symptoms (Table 2) and laboratory tests that include blood glucose levels and/or an oral glucose tolerance test (OGTT). The WHO criteria for diagnosis are given in Box 2. Recently, the ADA added HbA1c of 6.5% or greater as another criterion. Usually, children present to primary care so a high index of suspicion by GPs is necessary to make the diagnosis. Once suspected, the GP should refer the child immediately to a paediatrician to be seen on the same day. Initial management depends on the presentation. If the child presents with emergency symptoms suggestive of DKA, immediate treatment should be initiated in hospital.
Diagnosis of diabetes mellitus
Symptoms of diabetes plus random plasma glucose concentration more than or equal to 11.1 mmol/l (200 mg/dl)
Fasting plasma glucose more than or equal to 7.0 mmol/l (126 mg/dl) Fasting is defined as no caloric intake for at least 8 hours
Two hour post-load glucose more than or equal to 11.1 mmol/l (200 mg/dl) during an OGTT. The OGTT should be performed as described by WHO, using a glucose load containing the equivalent of 75 g anhydrous glucose dissolved in water or 1.75 g/kg of body weight to a maximum of 75g.
Diabetic ketoacidosis
Children may present to primary care with DKA, which is often precipitated by infection and resultant poor glucose control. Treatment of DKA is not within the remit of primary care management. This is a life-threatening condition and it is important to make the diagnosis to facilitate immediate referral and treatment in a specialist centre. DKA should be suspected in the presence of hyperglycaemia (blood glucose more than 11.1 mmol/l) and ketones in the urine (ketonuria). Emergency assessment of patients is performed in hospital to confirm the diagnosis. The management of DKA includes correction of dehydration and acidosis, reversal of ketosis, restoration of blood glucose to normal levels, identification and treatment of any precipitating events and avoidance of any complications.
Newly diagnosed diabetes
Children with type 1 diabetes who are younger than 2 years of age and children and young people who have social or emotional difficulties or who live a long way from hospital should be offered inpatient initial management (NICE, 2004). The aim of initial management is to confirm the diagnosis and initiate insulin therapy. The patient and their family should be offered a comprehensive package of support by the multidisciplinary paediatric diabetic care team and 24 hours a day access to the team for advice. They should feel involved in all decisions relating to every aspect of their care. The multidisciplinary team should include a paediatrician, paediatric diabetic specialist nurse (PDSN) and dietician.
It is paramount at this initial stage of management to offer children and their families a structured programme of education to cover the aims of insulin treatment, methods of delivery, self-monitoring of blood glucose, the effects of diet, physical activity and intercurrent illness on glycaemic control and the detection and management of hypoglycaemia. The education should be tailored to each child depending on his or her maturity.
Treatment with insulin
Different types of insulin and insulin analogues are available for use and these are described as:
rapid acting regular or soluble intermediate acting basal long acting long acting
Regular or soluble insulin is most often used intravenously in the treatment of DKA. Different insulin regimes are available for ongoing treatment. Frequently used regimes include two injections daily, three injections daily, the basal–bolus regime and the insulin pump regime. The type of regime used in a particular patient will depend on a number of factors including age, duration of diabetes, school and work commitments, dietary pattern and the preference of the patient and the family. At least two injections daily are advisable in most children. Basal–bolus regime tries to mimic the physiological release of insulin with 40–60% of the total daily insulin requirement given as basal long-acting insulin and the rest given with meals in divided doses (see Table 3 and Fig. 1).
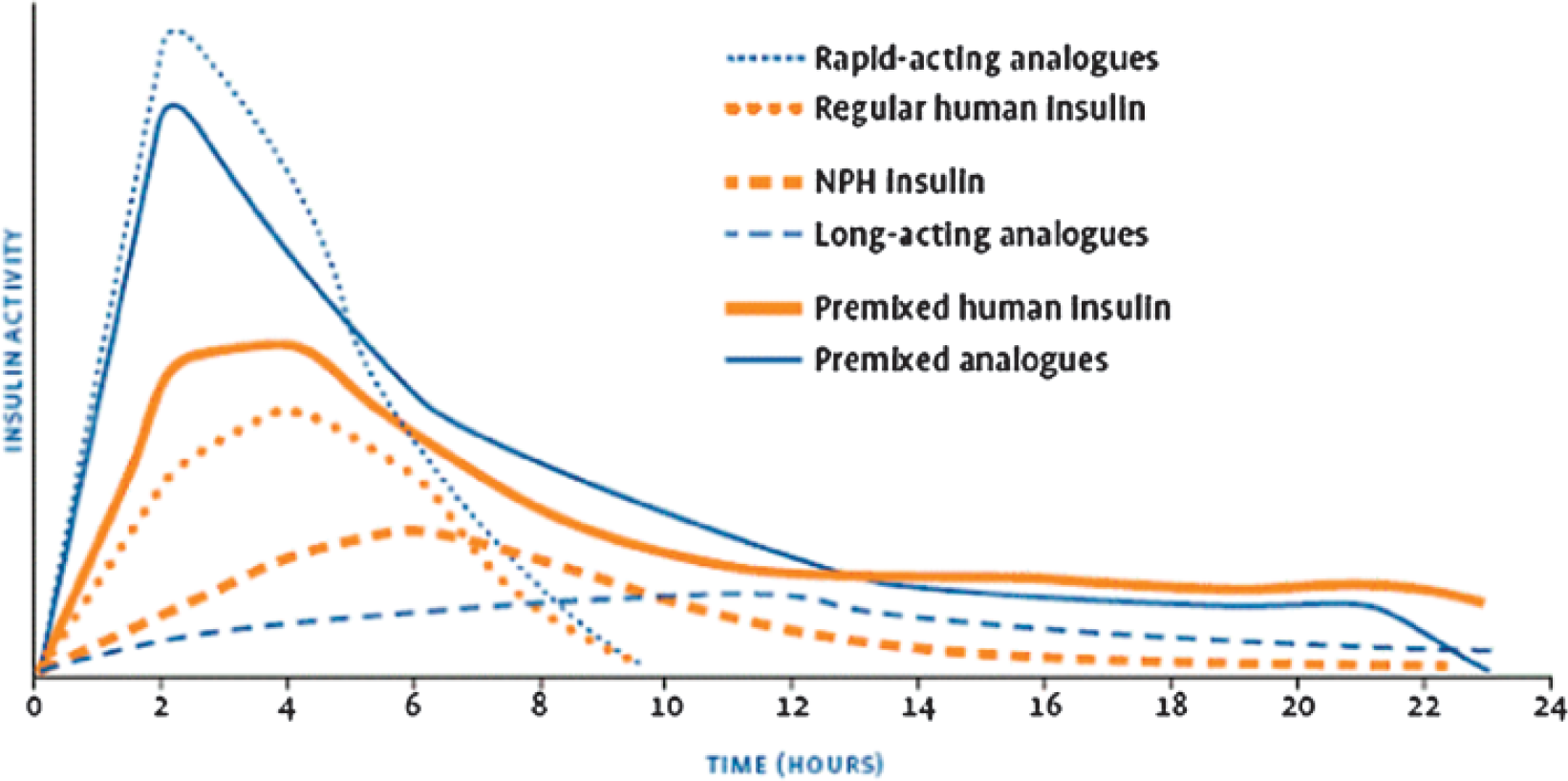
Activity of insulin preparations. The figure illustrates the activity of different insulin preparations. The rapid acting insulin preparations reach their peak effect within 2 hours and are short acting. The long-acting analogues have the peak effect between 10 and 12 hours and are long acting. The combined preparations have earlier peak effect and are long acting.
Insulin regimes

Ongoing management
As diabetes is a lifelong chronic disease, the management of children with diabetes will involve paediatric services from the time of initial diagnosis to the safe transfer of care to the adolescent and adult services. Children should be followed up three to four times each year but may need to be seen more often depending on their glycaemic control.
The aim of follow-up is to achieve good glycaemic control, to screen for short-term and long-term complications and to monitor associated conditions. The diagnosis of diabetes will have a huge psychological impact on the child and family. Coming to terms with the diagnosis can be very difficult and may take time. In addition to the support provided by the secondary care team, the role of the PDSN and GP is vital in helping children and families to pass through this difficult period.
Monitoring during follow-up visits
Immediate and every day glucose control are usually monitored by measurement of blood glucose. Glycosylated haemoglobin (HbA1c) reflects the control of blood glucose during the preceding 4–12 weeks. The target for long-term glycaemic control is HbA1c less than 7.5% and children should be encouraged to use self-monitoring of blood glucose three to four times daily to achieve this. Urine glucose monitoring is less effective in achieving long-term glycaemic control. Optimal glycaemic control will help in preventing episodes of hypoglycaemia and hyperglycaemia as well as long-term macrovascular and microvascular complications. Any child with HbA1c persistently above 9.5% should be offered additional help to achieve better glucose control. Further advice regarding management during exercise, travel and illness should also be offered during follow-up visits.
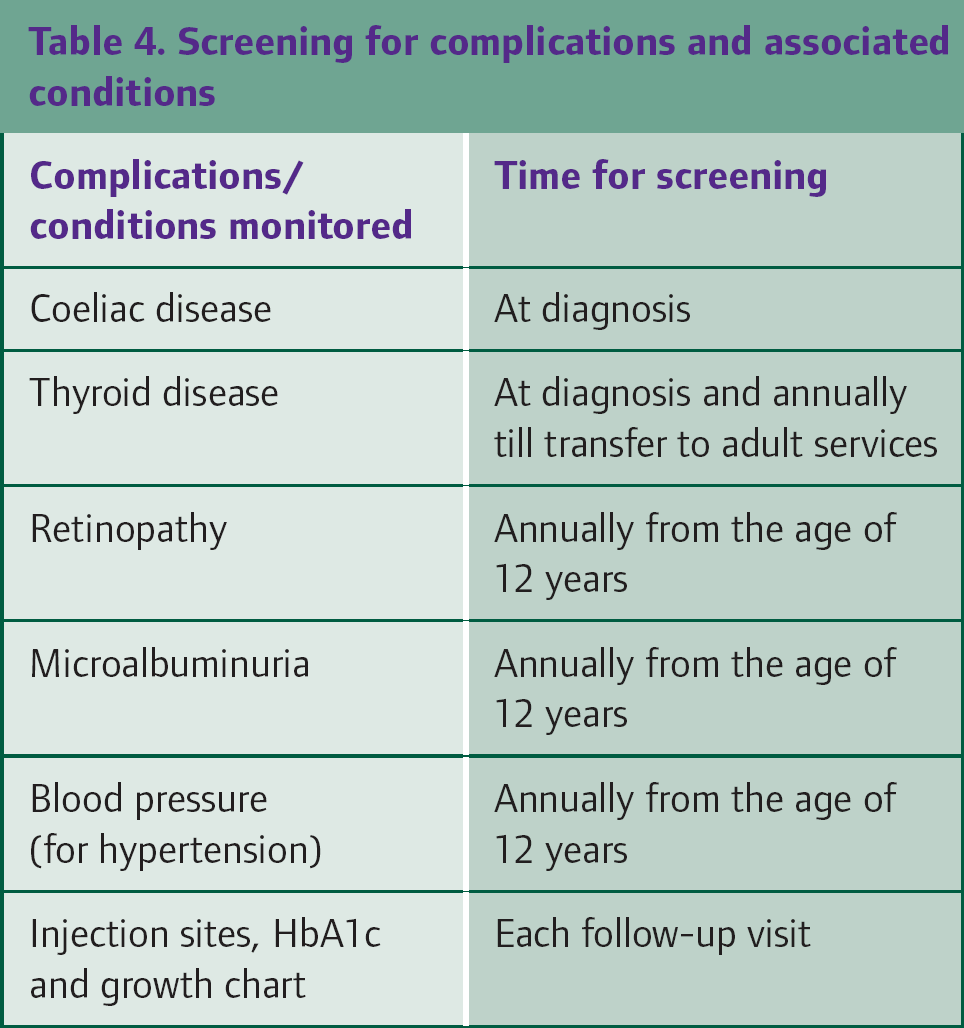
The state of injection sites should be checked during each visit and foot care review should be performed annually. Impaired growth and development are more likely to occur in children with diabetes so monitoring of height and weight on percentile charts is crucial. Although rare, children should be examined for juvenile cataract, necrobiosis lipoidica and Addison's disease during clinic visits. Diabetes is also associated with other long-term complications (as shown in Fig. 2) and patients should be screened for these at the recommended intervals (Table 4).

Complications of diabetes mellitus.
Screening for complications and associated conditions
Managing psychosocial problems
Children and young people with diabetes are at greater risk of developing emotional and behavioural problems than other children. The International Society for Paediatric and Adolescent Diabetes (ISPAD) Consensus Guidelines (2009) state that ‘psychosocial factors are the most important influences affecting the care and management of diabetes’.
It has been observed that many young people with diabetes have depression, eating disorders, behavioural problems, anxiety and low self-esteem. The diagnosis of diabetes itself can have a devastating effect on children. They may find it difficult to explain their condition to siblings at home and friends at school. They are prone to develop anxiety or depression especially when they encounter difficulties in self-management of diabetes and after a long duration of treatment. Eating disorder is especially common in female adolescents and can lead to increased episodes of persistent hyperglycaemia and poor glucose control. These children need early referral to psychologists for intervention. The diabetic care team and mental health professionals should manage them jointly to achieve concurrently better glucose control and treat psychosocial disorders.
Recurrent hypoglycaemic episodes associated with seizures increase risk of long-term neurocognitive dysfunction. These children should be referred for assessment of cognitive function. Non-adherence to treatment can be a major issue in adolescents. This should be handled in a sensitive manner and patients and their families should receive advice and counselling where appropriate. It is important to consider psychological assessment within the multidisciplinary diabetic team to exclude depression even in children with excellent glycaemic control as they come to terms with their lifelong illness.
Parents and other family members also need support in order to manage the child with diabetes. Reports suggest that 24% of mothers and 22% of fathers undergo post-traumatic stress disorder 6 weeks after the child's diagnosis. Family-based behavioural procedures such as goal-setting, self-monitoring, positive reinforcement and appropriately shared responsibility should be offered at the diabetes clinic by doctors, nurses and psychologists. Psychologists and social workers should be part of the multidisciplinary team to enable appropriate management of children with diabetes. GPs play a major part in identifying issues of family disharmony and stress and making appropriate referrals if required.
Care of diabetic children in school
When a child is diagnosed with diabetes, the PDSN should contact the child's school and arrange a school visit soon after discharge from the hospital. The visit should involve a meeting between the form teacher, special educational needs coordinator, specialist teachers and the school nurse along with the child and their parent to draw up an individual care plan. This care plan should then be updated yearly. In addition, the PDSN can offer group education to the teaching and nonteaching staff in the school during staff meetings and inset days. In some areas of the UK, the PDSN and the dietician jointly run training sessions for the school staff on how to manage a child with diabetes in school. The staff should then disseminate this information to their teams in school.
When the child is offered a change in insulin regime during follow-up with the diabetic care team, the PDSN usually arranges a further visit to the school to make relevant changes to the care plan.
Exercise
Regular exercise may reduce the risk of developing macrovascular complications in the long term and should be encouraged. There is no contraindication for children with diabetes to restrict their participation in sports. If playing sport professionally, patients will need to have a comprehensive review with the diabetic care team beforehand and also should be referred to the local and national governing bodies for such sports.
Exercise can produce hypoglycaemia and it may occur several hours after prolonged exercise. Changes in food intake and insulin requirement are necessary during exercise. Blood glucose levels should be checked at regular intervals before and during any prolonged exercise (Box 3). This will enable the patient to identify his or her own glycaemic response to different exercise conditions and will help in planning the insulin dose adjustments that are necessary.
Long distance travel and holiday
Diabetes should not be a barrier to travel for children and their families. Planning in advance is essential to minimize any potential problems and have a safe holiday. No major change to insulin is required during travel on short flights and when the time zone change is less than 4 hours. It is important to carry enough monitoring kit and insulin for the period of travel and taking at least twice as much as would normally be required is recommended. A letter from the GP is necessary to carry such medications in hand luggage in a cool bag as insulin would freeze and become denatured in the hold of an aeroplane. Box 4 shows a checklist of key considerations prior to and during travel.
Alcohol, smoking and recreational drugs
Young people with diabetes should receive education on the effects of alcohol consumption, smoking and the use of recreational drugs on glycaemic control. Hypoglycaemia is more likely to occur with alcohol consumption. Moderate amounts of alcohol in line with daily guidelines can be consumed without affecting short-term glucose control. Serious hypoglycaemia can occur especially with minimal carbohydrate intake during consumption of large quantities of alcohol and this can occur many hours after prolonged drinking. Hypoglycaemia can be missed or mistaken for drunken confusion. It is important to advise patients not to drink on an empty stomach and consume a starchy or carbohydrate snack before, during and after drinking. Patients should also be advised to keep a form of diabetic identification to obtain help in case of any emergency.
Advice for exercise
Monitor blood glucose levels before, during and after exercise Consume additional carbohydrate before exercise if glucose level is less than 7 mmol/l Make carbohydrate-based food readily available and consume to avoid hypoglycaemia during exercise Adjust insulin dose depending on response to exercise If the blood glucose level is more than 17 mmol/l, undertake exercise with caution Continue monitoring of glucose levels at regular intervals as hypoglycaemia can occur several hours after prolonged exercise
Long distance travel checklist
Essential vaccinations before travel Advice from the diabetic care team when travelling across time zones Letter from the doctor (GP) Travel insurance Insulin syringes in a cold bag and glucose monitoring kit (twice as much as needed) Extra snacks if any delay is anticipated Glucogel and glucagon Make sure the people at the place of your visit and stay are aware of your condition
Smoking has harmful effects (as shown in Box 5), which increase the risk of vascular complications in patients with diabetes. Children and young people should be encouraged not to start smoking. Those who smoke should be offered help through smoking cessation programmes.
Illness and sick day rules
Illness and infection can increase the blood glucose levels. Presence of high glucose levels can be associated with polyuria leading to dehydration. Dehydration is made worse with high temperature and certain illnesses such as gastroenteritis. Some children may exhibit symptoms of hypoglycaemia. High blood glucose levels make glucose control very difficult and increase the severity of some infections. Hence, blood and urine glucose levels should be monitored more often (eight times in 24 hours) to determine the response to and adjust the dose of the insulin. It is important to drink plenty of fluids to avoid dehydration while continuing with insulin to control the blood glucose level. Adequate supply of monitoring strips and equipment should be available.
Effects of smoking
Increase in low-density lipoproteins Increase in blood pressure Decrease in the oxygen supply to tissues Increase in blood sugar levels Increased risk of developing end organ damage (neuropathy, nephropathy and retinopathy)
Children can become ill very rapidly and help should be sought early. Hospital admission and treatment may be necessary when children with diabetes become ill. When the blood glucose is more than 15 mmol/l, urine and blood ketone testing is necessary. Once recovered from the illness, blood glucose control may take time to return to normal. During this time, monitoring of blood or urine glucose should be continued with increased frequency. Children should be vaccinated against flu, swine flu and pneumococcal infections.
Immunization
Children with diabetes should be immunized according to the Department of Health guidelines. In addition to the routine immunization schedule, those above 6 months of age should be offered annual immunization against influenza. The Department of Health also recommends additional doses of immunization against pneumococcal infections for children with diabetes.
Continuity of care
The care of children with diabetes will need to be transferred over to adult services during adolescence. The transition should be made as seamless as possible. There are additional physical and psychological changes that occur during adolescence, which should be taken into account. Increased insulin requirements during puberty can make the management of diabetes more complex. The transition should be discussed with children and their families several visits before it is due to take place. This will help in mentally preparing them for the transition. The transfer of care should occur at a time of relative stability in the child's health. Problems noted during transition include lack of consistent care in a significant number of patients and difficult metabolic control in spite of good care. Counselling about the changes in care and the importance of regular attendance are important in achieving good glycaemic control following transition.
Complications and associated conditions
Hypoglycaemia
Hypoglycaemia is defined as blood glucose less than 3.9 mmol/l in children and adolescents with type 1 diabetes. The symptoms due to hypoglycaemia can be autonomic or neuroglycopenic (Box 6). Hypoglycaemia is classified as mild, moderate or severe. With mild or moderate hypoglycaemia, the child or parent is aware of and able to treat the hypoglycaemia orally after documenting the low blood glucose level. With severe hypoglycaemia, the child has altered mental status and conscious level and may have convulsions. Severe hypoglycaemia requires parenteral glucose therapy. The aim of treatment is to restore the blood glucose to normoglycaemia (greater than 5.6 mmol/l) by administration of quick acting simple sugars as outlined in Table 5.
Symptoms and signs of hypoglycaemia
Hunger Headache Nausea Tiredness
Irritability Erratic behaviour Nightmares Inconsolable crying
Trembling Pounding of heart Cold sweatiness Pallor
Difficulty concentrating Poor judgement and confusion Dizziness and unsteady gait Slurred speech Loss of consciousness Seizure Death
Treatment of hypoglycaemia

Associated autoimmune conditions
A higher proportion of children with type 1 diabetes are found to have organ-specific autoantibodies (e.g. thyroid, adrenal) than children from the general population. Primary hypothyroidism due to autoimmune thyroiditis occurs in 3–8% of children with diabetes and it is confirmed by the presence of low free thyroxine levels and high thyroid-stimulating hormone (TSH) levels in serum. Hyperthyroidism can also occur but is less common than hypothyroidism.
Coeliac disease occurs in 1–10% of diabetic children. It is usually asymptomatic and is not necessarily associated with poor growth or poor diabetic control. Any diabetic child with gastrointestinal symptoms should be investigated for coeliac disease. Children with proven coeliac disease should be referred to a paediatric gastroenterologist and receive support from a paediatric dietician with experience of gluten-free diets.
Vitiligo, which is an acquired pigmentary disorder, occurs in 6% of patients and primary adrenal insufficiency (Addison's disease) develops in up to 2% of patients. Children should be screened for these complications at regular intervals (Table 4).
Vascular complications
Children with diabetes are prone to develop microvascular complications, such as retinopathy, nephropathy and neuropathy. Retinopathy can progress to loss of vision. Nephropathy is defined as persistent proteinuria or microalbuminuria and can be associated with hypertension. Neuropathy can affect both somatic and autonomic nerves. Hypertension and atherosclerosis are other vascular complications. Improvement in glycaemic control can reduce the risk of onset and progression of vascular complications.
Considerations for primary care
Children and adolescents often present initially to primary care with symptoms of diabetes. It is vital that GPs can recognize the symptoms and establish the diagnosis. Misinterpretation of symptoms and delay in diagnosis increase the risk of DKA. Children with symptoms should be referred on the same day for specialist assessment on the basis of capillary glucose testing only without delaying to get a laboratory sample to confirm the diagnosis.
Additional vaccination (influenza and pneumococcal) should be offered according to the national guidelines for children with established diabetes. In reality, most children are managed by the secondary care multidisciplinary team and have good access to the team; however, as they present to primary care with common illness and infections, it is important that practice staff are aware of children on the list with type 1 diabetes so that they are given urgent appointments or triaged to the GP if acutely ill. GPs should have an understanding of the changes in insulin requirements during illness and the time to refer to the specialist.
Links for useful websites and support groups
Diabetes UK (www.diabetes.org.uk) Diabetes Federation of Ireland (www.diabetes.ie) American Diabetes Association (www.diabetes.org) International Society for Pediatric and Adolescent Diabetes (www.ispad.org) International Diabetes Federation (www.idf.org) Juvenile Diabetes Research Foundation (www.jdrf.org.uk) NHS Diabetes: (www.diabetes.nhs.uk)
Diabetes Research and Wellness Foundation (www.drwf.org) Diabetic foot page (www.diabeticfoot.org.uk) Diabetic retinopathy screening (www.nscretinopathy.org.uk)
Primary care management
Newly diagnosed diabetes in children Emergency symptoms/DKA Significant deterioration or exacerbation of complications (acute visual disturbance, renal failure or vascular emergencies) Severe hypoglycaemia Diabetic foot emergencies (gangrene, deep ulcers or infection)
Episodes of hypoglycaemia Poor glycaemic control Psychosocial problems
Follow-up of high-risk children (for early diagnosis) Diagnosis at presentation Initial treatment of emergencies and severe hypoglycaemia prior to transfer to hospital Treatment of mild or moderate hypoglycaemia Monitoring (growth chart, injection sites and HbA1c) Immunizations Advice (diet, lifestyle, travel and exercise)
GPs also need sufficient knowledge to give the patient and family advice regarding air travel across time zones, exercise and be able to address psychosocial problems and support transition of care to adult units. Information for patients is available from diabetes organizations and patient support groups. Patients and families can be given the list of their websites to access information (Box 7). A summary of the suggested management of a child or adolescent presenting to primary care with symptoms is depicted in Fig. 3. The ongoing management responsibilities for GPs caring for children with diabetes are described in Box 8.

Management of diabetes in children.
Key points
Diabetes mellitus is a metabolic disease mediated by an autoimmune process and susceptibility is genetically determined Type 1 diabetes is more common in children. The majority of children with diabetes have type 1 diabetes Symptoms of diabetes in children and adolescents can be misinterpreted and the diagnosis can be missed which can increase the risk of subsequent presentation with DKA Management of diabetes in children should involve a multidisciplinary team involving a paediatrician, diabetic nurse, dietician, optometrist, chiropodist, psychologist and the patient's GP Children with diabetes and their families should be offered education regarding the disease and its management and advice regarding immunization and managing long distance travel, exercise, sickness and psychosocial problems Children with diabetes should be followed up for the long-term complications such as retinopathy, nephropathy, thyroid problems and coeliac disease according to nationally established guidelines