
Abstract
Public health specialists can be described as leaders of the ‘upstream health workforce’, concerned with preventing unnecessary and ‘revolving door’ contact with health services. Achieving this requires working to promote good health, improve health services and protect populations from infectious disease and environmental risks. Public health work is based upon the recognition that populations are complex constructions of groups of individuals, who may or may not seek help for health problems or be able effectively to take action to improve their own health. This article will define key areas of public health practice giving specific examples of the role of the public health specialist in the UK, as well as how and why primary care professionals might access specialist advice. The examples demonstrate the great potential for improving population health through the complementary efforts of primary care and public health professionals.
The GP curriculum and public health
GPs should be able to describe the roles of the other professionals involved in public health, e.g. school nurses, health visitors and public health specialists. GPs should understand:
The concept of health
The need to reconcile the needs of individuals with the needs of the community in which they live
The inequalities in health care provision: the ‘inverse care law’
The epidemiology of problems presenting in primary care
The principles of prevention and preventative strategies
The role of the GP and the wider primary health care team in health promotion activities in the community
Promotion of health through health promotion or disease prevention programmes
The importance of ethical tensions between the needs of the individual and the community and to act appropriately
Public health and the role of the public health specialist
Some of the greatest health improvement advances in the last century are attributable to public health efforts. An international poll, conducted by the British Medical Journal, asked readers to nominate and then vote on a shortlist of 15 of the most important medical advances since 1840 (BMJ Supplement, 2007). Sanitation was ultimately voted the winner, with nominations including public health efforts relating to immunization and the characterization of the risks of smoking.
The availability of interventions and development of an understanding of risk factors for disease is only part of the battle for public health professionals. Variation in progress with regard to these major health advances internationally is an ongoing public health concern. Furthermore, the public health challenges facing the higher income world simply evolve.
In the UK, the increasing prevalence of long-term conditions such as coronary heart disease, diabetes, asthma and chronic obstructive pulmonary disease is exerting pressure on the current health care system. It is, thus, important that a sustainable solution to health service delivery is found. Responding to this challenge involves mitigating risks to and optimizing the determinants of health and ensuring health services, whether in the community, or in primary and secondary care, are provided and accessed in a way that is proportionate to need. Underpinning this work is the importance of using limited health care resources to maximize population health benefit.
The need for protection from ongoing and emerging infection and environmental threats also persists in the UK, despite advances in previous decades. Furthermore, one of the most important evolving environmental threats to public health, for which universal action is necessary, is climate change (Costello et al., 2009). This is a neglected but crucial area for health workforce action.
The role of the public health workforce in the UK includes four main interlinked areas of work: improving health, protecting health, improving health services and academic public health. It can be difficult to imagine what the daily work of a consultant in public health might involve, given these broadly defined activities. Indeed, almost all efforts to provide for the needs of society have an impact on population health, from health care provision to good civil engineering. To help develop an understanding of the role of the public health specialist, each domain of public health work will be considered in detail.
Improving health and health services
These two areas of public health practice are closely linked with regard to specialist skills employed, and often considered together when approaching a public health problem. Both areas involve public health specialist teams working with a wide range of health and social care professionals in the community, in primary and secondary care, as well as with local authorities and the voluntary sector. These domains of work are concerned with primary prevention (preventing disease), secondary prevention (early detection of disease and prevention of further morbidity) and tertiary prevention (prevention of further morbidity and disability due to established disease) activities. For example, health improvement activity to promote physical exercise can be considered part of the same area of work as treatment for people with cardiovascular disease. Importantly, primary prevention activities should be considered not solely in terms of illness prevention but as a means of promoting good health, in keeping with the World Health Organization definition of health:
Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity. (World Health Organization, 1948)
Public health professionals act as advocates for the public good; through commissioning, planning and evaluating interventions influencing health determinants at individual and wider societal or environmental levels (Fig. 1). This may, for example, involve working with primary and community care professionals to support the implementation of cost effective brief interventions such as those related to alcohol consumption reduction (NICE, 2010), smoking cessation (NICE, 2006a) or increasing physical activity (NICE, 2006b). The role can also involve assessing the evidence and lobbying for appropriate legislative action, such as the introduction of the public smoking ban in 2007, for which there is accumulating evidence of health benefit (Fig. 2). More recently, the Faculty of Public Health joined other members of the Smokefree Action Coalition, including the Royal College of General Practitioners, to lobby the Secretary of State for Health to remove point of sale tobacco advertising and support introduction of plain cigarette packaging requirements (Faculty of Public Health, 2010). The public health remit also includes overseeing population interventions such as screening and vaccination programmes.

Determinants of Health. Dahlgren G, Whitehead M. Tackling inequalities in health: what can we learn from what has been tried?
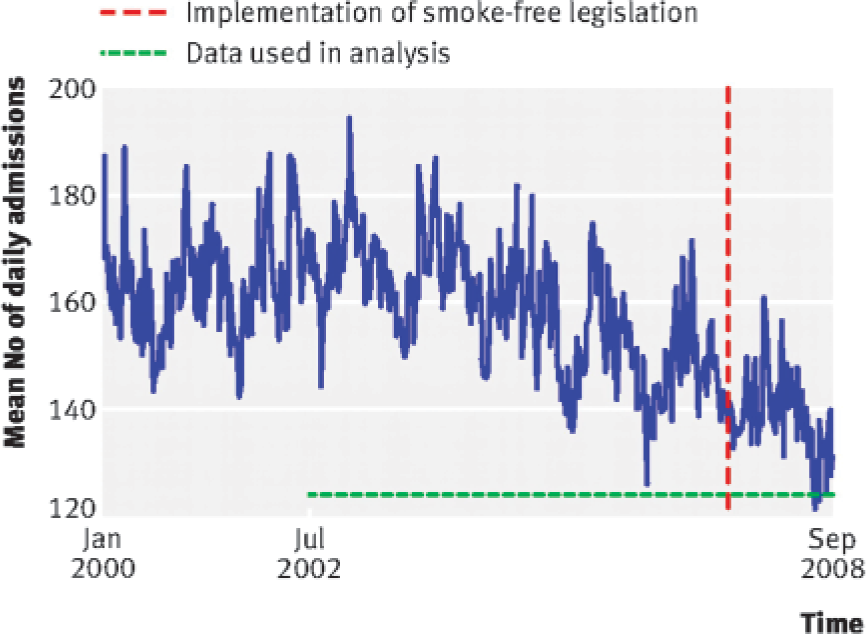
Trends in overall weekly number of emergency admissions for myocardial infarction (average daily count) from January 2000 to September 2008.
Improvement of health services focuses on secondary and tertiary prevention activity, aimed at minimizing morbidity, disability and mortality and ensuring the best (i.e. cost effective) use of limited health care resources. For example, identifying patients at high risk of cardiovascular disease in the 40–74 years age group from primary care registers has led to the opportunity to provide early intervention, through the National Health Service (NHS) vascular risk check programme (UK National Screening Committee, 2008). Implementation of the vascular risk check programme in Sandwell Primary Care Trust is estimated through modelling to prevent 278 cardiovascular and cerebrovascular admissions and 123 deaths over a 10-year period, based on pharmacological management instituted for an initial cohort of 20000 patients identified for the check. Interventions offered in Sandwell following risk checks include support with smoking cessation, obesity management, provision of advice regarding physical activity, diagnostic testing for diabetes and chronic kidney disease and appropriate aspirin, antihypertensive and statin prescription (Marshall et al., 2008; Westerby, 2009).
Specialists work with commissioners and providers of primary, secondary and community care to review how services are delivered, with reference to local health needs and evidence regarding what is effective. When services are re-organized, e.g. if there is a need for them to be provided differently or in a different physical setting, public health specialists play a key part in the development of new patient pathways. Their role is to help link the steps of a patient's journey, which may involve contact with a variety of health care organizations and departments, taking into account the needs of clinicians, patients and other interested groups (such as carers). For example, if considering how best to provide rehabilitation services for individuals with neurological injury, it is important to understand how neurosurgical operating activities are organized and whether there is provision for inpatient specialist neurorehabilitation, outpatient support and vocational rehabilitation.
Identifying where there are important gaps in provision and understanding how patients ‘flow’ through the system is important for ensuring effective and efficient services. Clinical systems improvement methods, particularly those relating to Lean management theory, are being used increasingly in health care in the UK, with the aim of improving service outcomes (Radnor, 2010). Lean improvement methods, initially used in the manufacturing industry, are used to highlight value-adding steps and those which introduce waste into processes and systems, from the patient perspective. Value-adding steps in a patient journey are those which contribute directly to positive health outcomes or patient experience, e.g. seeing a health professional and being given appropriate advice or treatment. Wasteful steps are the converse and include the times during which the patient is waiting for the next appointment or stage of treatment or where there is unnecessary repetition in the patient pathway. Although implementation of these methods is not without its challenges or failures in health care, it has been shown to stimulate improvement in flow through emergency departments, outpatient clinic efficiency and time between GP referral and treatment (Cooke et al., 2002; Womack and Miller, 2005; Jones et al., 2006; Radnor, 2010).
As described, the role of the public health specialist in health and health service improvement lies in providing expertise in assessing the need for health and health services, co-ordinating/commissioning appropriate interventions and services through prioritization and evaluating resultant population health outcomes. This is an area that GPs in England, as health commissioners, will be becoming increasingly familiar with. Health needs assessment is ‘a systematic method of identifying unmet health and health care needs of a population and making changes to meet these unmet needs’. Need is defined as a population's ‘capacity to benefit’ from an intervention (Wright et al., 1998). Assessment comprises three main elements. The first involves quantifying the size of a health problem or group of problems in a particular population (incidence, prevalence, distribution according to demographic profile, and projected future need as this profile changes). The second relates to understanding current service provision and associated outcomes as well as future required capacity. The final element involves a detailed review of the evidence base to determine the cost effectiveness of interventions.
The fundamental output of the assessment process is to change health improvement activities or service provision. Recommendations for change feed into commissioning prioritization processes if additional resource is required or changes to current resource use are needed. The assessment process is iterative and evaluation of changes made is paramount. The process is underpinned by the need to have access to accurate surveillance information and skilled support for data analysis and interpretation.
Prioritization of resources is central to provision of good health care but can be a difficult and emotive area as it requires making judgements about the relative worth of different interventions, which may seem at odds with the clinical professional duty to provide the best possible care for individual patients. Public health specialists play an important role in commissioning. Where working effectively, commissioning can be thought of as the process of identifying population need, determining which services will meet those needs (within financial constraints), specifying how these should be provided, and then purchasing them. Commissioning is a cyclical process; organizations should be iteratively assessing if services are meeting needs, changing policies and contracts accordingly. In Wales and Scotland, specialists are involved in planning more often than commissioning (very similar processes) as there is no commissioner/provider split.
Given a fixed financial budget to meet population health and health care needs, it is important for there to be a transparent and rational process for allocation of health funds. The concept of ‘opportunity cost’ is fundamentally important. When a new intervention is proposed, it is essential to consider what activities will need to be stopped or what alternative activities will not be possible, if the new intervention is introduced (the opportunity cost). This is an area of conflict in the individual vs. population approach to health care practice: an individual receiving funds for a treatment not routinely funded by the NHS will consume resource from elsewhere in the system, i.e. there will always be a consequent effect upon health care provision.
The ultimate aim of these two domains of public health practice is to improve population health. Geoffrey Rose, the renowned physician and epidemiologist, contributed hugely to preventative health theory through describing the ‘whole population’ approach to improving health, as an alternative or complementary approach to ‘high-risk’ strategies (Rose, 1985). The latter aim to identify those at highest risk and reduce their risk of negative health outcomes (e.g. screening programmes are often developed on this basis). The former places importance on reducing risk in the population as a whole on the basis that a small number of people at high risk cause less disease than a larger number of people at lower risk. There are situations in which one or the other approach is used, and sometimes they are used in combination. Figure 3a demonstrates the conceptual aim of the population approach, which is to shift the distribution of risk in the population as a whole towards a more favourable risk profile.
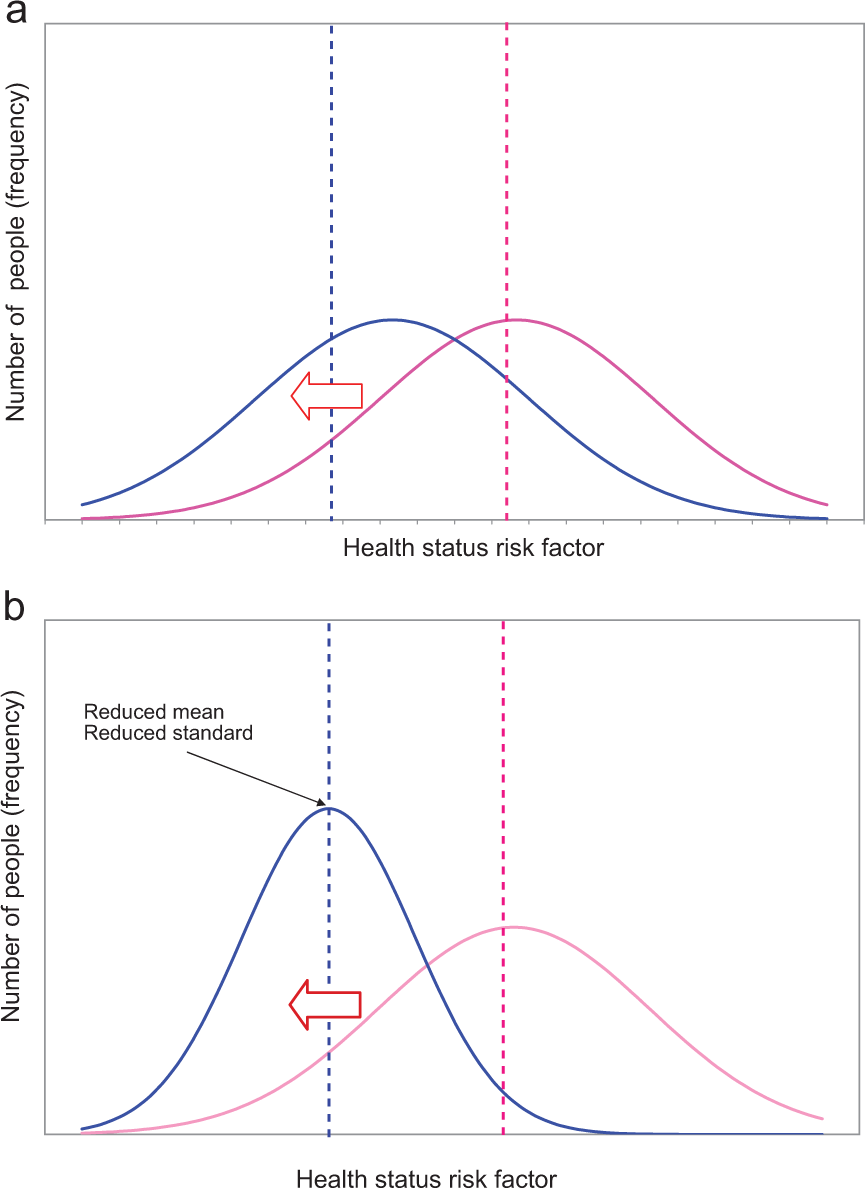
Rose's population approach and health inequalities. (a) Population approach to prevention: risk reduction at a ‘whole population’ level. (b) Population approach to prevention and reduction of health inequalities (conceptualised by article authors).
An important concept to consider here is that of health inequality, which is tightly linked to population health improvement. Julian Tudor Hart, a GP from West Glamorgan, Wales, combined clinical work with a remarkable research career. His seminal article ‘The Inverse Care Law’, asserts that ‘the availability of good medical care tends to vary inversely with the need for the population served’ (Hart, 1971). This paradox remains true. It is, thus, important to remember that differences in health outcomes, excluding constitutional and random factors, are not inevitable and warrant our efforts to effect change.
Professor Michael Marmot's recent review of health inequalities in England (Marmot, 2010), demonstrates a persisting and marked gradient in health outcomes, attributable to socio-economic status, for a number of different health measures (Fig. 4). Proposals put forward by Marmot include whole population strategies, with targeted work to ‘improve the health of the poorest fastest’. Rose's population approach can be adapted to include this concept, as conceptualized in Fig. 3b. Reducing health inequalities is, thus, inextricably linked with the health improvement responsibilities of the public health and wider health workforce.
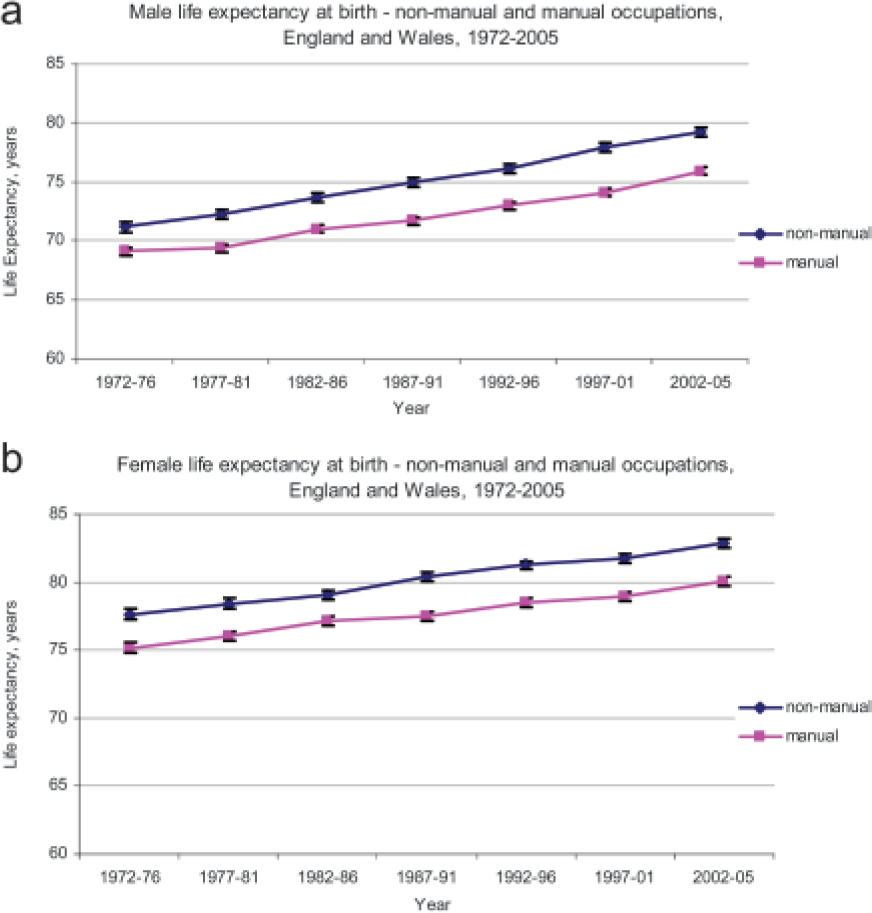
Life expectancy at birth by social class (a) males and (b) females, England and Wales, 1972–2005.
Health protection
The health protection function of public health involves the prevention and control of communicable disease transmission and protection from environmental hazards (e.g. chemicals, poisons, radiation). Health protection responsibilities include receiving notifications of statutory notifiable diseases/hazards (on the basis of clinical suspicion) from registered medical practitioners and laboratories, and taking action to prevent onward transmission or further harm. Measures taken include removal of harmful sources, giving infection/hazard control advice, contact tracing and administration of prophylaxis as appropriate.
The list of notifiable diseases has changed in England according to new health protection legislation in 2010 and now includes notification of any infection (e.g. new or emerging infections) or form of contamination (e.g. by chemicals or radiation) which may pose a risk to health (Department of Health, 2010a; Health Protection Agency, 2011;). Similar changes have occurred in Welsh and Scottish legislation (Health Protection Scotland, 2010; The National Archives, 2010). Department of Health guidance for England gives examples of other diseases or hazards for which notification is recommended because of their public health implications (Department of Health, 2010a). These include cases of carbon monoxide poisoning, chickenpox in health care workers and parvovirus B19 in contacts of pregnant women (Department of Health, 2010a). The health protection function includes planning for large-scale emergencies, such as pandemics, and other disasters which may involve mass casualties.
Health protection teams in the UK provide a reactive service, giving advice regarding single cases of disease or outbreaks. Responsibilities are also held for proactive work. Analysis of surveillance information can be used to identify future potential risk to inform long-term planning of prevention responses and monitor the impact of these measures. An example of this type of work includes developing strategies for promotion of vaccination uptake, as part of primary immunization schedules or ‘catch-up’ campaigns. A specific example of this would be the measles, mumps and rubella catch up campaign launched in 2008 in England, following large increases in confirmed measles cases linked to low vaccination uptake (Department of Health, 2008).
The much broader health protection threat posed by climate change is not one that can be ignored. Although the responsibility for action is universal, health professionals and the NHS, as one of the largest employers worldwide, have the opportunity to make a considerable impact. The NHS Sustainable Development Unit provides support for NHS organizations to reduce their carbon footprint. Projections demonstrate that many carbon-saving measures recommended for the NHS are also cost saving (NHS Sustainable Development Unit, 2010). Carbon-saving measures relevant for primary care include holding energy awareness campaigns, making small reductions in thermostat temperatures, improving heating and lighting controls, reducing drug wastage and ensuring appropriate roof and wall insulation (NHS Sustainable Development Unit, 2010).
Academic public health
Epidemiology, as the science of understanding health determinants and disease, is of fundamental importance to primary care practice, as it provides the basis for risk assessment undertaken with individuals as well as populations. Academic public health can be seen as the backbone of the evidence-based approach to population health practice. Academics may be involved in interventional research, such as trials of public health interventions, which themselves pose a different set of challenges to clinical trials (Macintyre, 2010). They may also be involved in undertaking evidence reviews of individual-level clinical or health-related technologies, using systematic review methods (such as those currently undertaken for the National Institute for Health and Clinical Excellence), to support public health and medical practice.
Some of the largest contributions to the understanding of determinants of health and their relationship with health outcomes have been made by observational studies, particularly cohort studies. Noted examples include Sir Richard Doll's British Doctors cohort study, which provided some of the best evidence regarding the link between smoking and lung cancer (Doll et al., 2004) and the Framingham Heart Study for its role in identification of cardiovascular risk factors (Framingham Heart Study, 2011).
Public health academics may also be involved in qualitative research activities, now often combined with quantitative methods. Qualitative research asks the ‘how and why’ questions and can set quantitative research findings in context. It is increasingly used as part of the evaluation of complex interventions, such as that being carried out in England for the Health Trainers project. This project involves training local community members (health trainers) to work with individuals at high risk of health problems, providing lifestyle change support (Department of Health, 2009).
Accessing specialist public health specialist advice
In the UK context, there are three main ways in which public health specialist advice may be sought by primary care professionals. These will be considered in turn, with reference to relevant sources of information.
Accessing urgent health protection advice
In England and Wales, a public health professional delegated by the ‘Proper Officer’ [usually a consultant in communicable disease control (CCDC), who fulfils a different specialist role to a consultant in general public health] is always available to take notifications of infectious disease and to give advice regarding individual cases and outbreaks. Similarly, in Scotland and Northern Ireland, notifications are taken by consultants in health protection (CHP) in local health boards or the Public Health Agency, respectively. During the day, calls to health protection teams are received by a CCDC/CHP, Specialty Registrar or Health Protection Nurse/Practitioner. Outside normal working hours, notifications can be made and advice sought through public health or health protection on-call systems. Calls will be taken by one of the above listed members of the health protection team or a Consultant/Director of Public Health.
Notifications often require immediate public health action, e.g. cases of probable meningococcal disease, E. Coli 0157 infection, carbon monoxide poisoning or outbreaks of any type. It is also worthwhile contacting health protection teams in the daytime or on-call teams after hours with queries requiring specialist advice about a particular infectious disease or environmental hazard issue. Verbal notifications need to be followed by paper notifications within 3 days to ensure complete surveillance records. Box 1 contains references to useful health protection-related resources.
Useful information sources—communicable disease control and health protection
Health Protection Agency website www.hpa.org.uk.
Public Health Wales website
Health Protection Scotland
website www.hps.scot.nhs.uk
Public Health Agency (Northern Ireland) website
The Green Book' Department of Health website
www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_079917
NHS Sustainable Development Unit website
Accessing information to improve primary care service provision
Primary care professionals are ideally placed to work closely with public health specialists and the wider public health workforce and need to consider population approaches when making decisions which affect their practice populations. A practice might have specific questions which will inform improvements in their services, such as:
How is our practice doing compared to others with regard to vaccination or screening uptake?
What is the likely true prevalence of diabetes or cardiovascular disease in our catchment population?
How do we compare with other practices with regard to referrals to secondary care for a particular problem?
We want to commission a weight management service, which models have been shown to be the most cost effective?
How can we best identify people on the practice list at high risk of a particular health problem?
How can we reduce emergency admissions to hospital?
Patients are demanding access to a new treatment they have heard/read about. Should we fund this treatment? How do we know if it is clinically and cost effective?
How can we disinvest so that funds can be made available?
The route of access to this advice would be through local Consultants in Public Health or the Director of Public Health. They will then allocate the request to a member of the public health team or signpost to available datasets and support practical interpretation of the data. Health information datasets hide complexities, which are important to understand in order to make rational and appropriate practical service decisions. Previously, such support has been crucial in enabling primary care practices to make changes to services previously commissioned from hospitals, allowing them to be provided in the community. There are a number of online resources which provide population health and health care activity data at both local and national levels (Box 2). The respective UK government websites are also useful resources.
Accessing advice and support regarding commissioning of health services
Public health specialists are ideally skilled to support primary care with commissioning and planning processes, due to their specialist expertise in needs assessment, data analysis and evidence appraisal as well as their experience in prioritization and commissioning processes, including planning and evaluating interventions and services, and supporting contract management (Solutions for Public Health, 2010). Advice and support can again be sought through Consultants/Directors of Public Health. The Director of Public Health in England will have a role in supporting GP commissioning as outlined in the White Paper for Public Health (Department of Health, 2010b). They also have important experience in working closely with local authorities, social care, and with other community services and the voluntary sector. Such a role facilitates a ‘whole system’ approach to pathways of care from primary prevention to high-quality tertiary care. Useful information resources for primary care professionals relating to prioritization, commissioning and clinical systems improvement can be found in Box 3.
‘The new world’ in England and future challenges
At the time of writing, it is believed that by April 2013, public health professionals working in health and services improvement and in health protection will be fully established in local authorities and Public Health England (a new executive agency of the Department of Health), respectively, and will no longer sit within the NHS or Health Protection Agency in England. The White Paper for Public Health and the more recent updated paper (Department of Health, 2010b, 2011) is clear that public health professionals will still be providing expertise and advice to the NHS as a skilled specialist workforce, including supporting GP commissioners. The new structure will enable the public health workforce to work with local government and primary care colleagues, through statutory Health and Wellbeing Boards, on issues affecting some of the wider environmental determinants of health.
The overall broad areas of responsibility for public health specialists will remain the same or in some ways widen, given more emphasis on wider determinant outcomes in local authorities. However, the organizational arrangements and accountabilities to new employers is likely to shape how work is prioritized and carried out. The challenges of the new world for public health are, therefore, in the process of being defined. However, working across multiple organizational boundaries and in a politically driven environment in local authorities will pose new challenges for the workforce, which needs to maintain a coherent and independent voice. Additionally, with GP-led clinical commissioning groups taking responsibility for commissioning in health care, it will be important for required support to be provided by the public health workforce, which is particularly crucial during this time of major change.
Useful sources of information—supporting service provision
Local/Practice level population data
Association of Public Health Observatories Website. ‘APHO general practice profiles’ Links to other UK observatories. www.apho.org.uk
Office for National Statistics Website (UK). ‘Neighbourhood tab’ www.statistics.gov.uk/default.asp
Comparisons of local/practice level data regarding primary and secondary activity and costs
NHS Comparators website (England) www.nhscomparators.nhs.uk
Secondary care admissions/outpatient data (broken down to hospital level/commissioning organisation level)
Hospital Episode Statistics website (England) www.hesonline.nhs.uk
Health and lifestyle information, including screening and immunization data (national and/or local levels) and primary-care population, mortality and service related (primary and secondary care) information (including Quality and Outcomes Framework (QOF) indicators)
NHS Information Centre website (England) www.ic.nhs.uk/about-us
National Centre for Health Outcomes Development (England): www.nchod.nhs.uk
Evidence-based information regarding nationally recommended care pathways (interactive)
Map of medicine website (England and Wales): www.eng.mapofmedicine.com/evidence/map/index.html
Information Services Division of NHS National Services Scotland www.isdscotland.org/isd/1.html
Scottish Public Health Observatory website www.scotpho.org.uk/home/home.asp
General Register Office for Scotland website www.gro-scotland.gov.uk/
Scottish Neighbourhood Statistics website www.sns.gov.uk
Scottish Index of Multiple Deprivation website www.scotland.gov.uk/Topics/Statistics/SIMD
NHS Health Scotland website www.healthscotland.com/index.aspx
Public Health Wales website. ‘Data and Health Intelligence’ www.wales.nhs.uk/sitesplus/888/page/46778
Public Health Wales Observatory website. www.wales.nhs.uk/sitesplus/922
Ireland and Northern Ireland's Population Health Observatory website www.inispho.org
Department of Health, Social Services and Public Safety website. ‘Statistics and Research’. www.dhsspsni.gov.uk/index/stats_research.htm
Northern Ireland Neighbourhood Information Service www.ninis.nisra.gov.uk/launch.asp
During a time of resource constriction, primary prevention activities can be sidelined in health care organizations. This is particularly so given that these activities are often criticized for their inability to deliver positive health outcomes in a timely fashion, especially those which have a positive impact on the ‘bottom line’. This is the inherent nature of health promotion work, which requires an appreciation of the long-term vision for population health. Given the distractions of the above challenges and while the economic, political and structural environment is changing, it is important for the health care community to remain focused on mitigating the threats to the health of the population and wisely use opportunities for health improvement.
Useful resources—prioritization and commissioning
NHS Institute for Innovation and Improvement website (recently launched Productive General Practice programme) www.institute.nhs.uk/
No Delays Scotland website (Scotland) www.nodelaysscotland.scot.nhs.uk
National Institute for Health and Clinical Excellence website www.nice.org.uk
NHS Quality Improvement Scotland website www.nhshealthquality.org/nhsqis/101.html#114
Right Care NHS Atlas of variation in health care (providing information at commissioning organization level) (England) www.rightcare.nhs.uk/atlas
NHS Confederation (briefing documents regarding prioritization) www.nhsconfed.org/Publications/prioritysetting/Pages/Prioritysetting.aspx
RCGP Centre for Commissioning website supporting GP skill development including development of GP commissioning competency framework www.rcgp.org.uk/centre_for_commissioning.aspx
Public Health commissioning network website (commissioning guidance and forum for discussion of difficult commissioning problems) (England) www.phcn.nhs.uk
Yorkshire and Humber Public Health Observatory website (information regarding prioritization and commissioning) www.yhpho.org.uk/default.aspx?RID=10297 www.yhpho.org.uk/default.aspx?RID=63821
Department of Health website (a number of commissioning packs have been developed for GP consortia by the Strategic Commissioning Development Unit) (England) www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/Browsable/DH_117500
Key points
There are four main areas of specialist public health practice in the UK, which overlap naturally with the work of primary care: health improvement, health protection, health services improvement and academic public health
Current public health challenges facing the UK include: increasing prevalence of lifestyle-related and long-term conditions, rising demand for health services, persisting health inequalities, budgetary constraints and the need to protect the population from emerging diseases and the impacts of climate change
Primary care professionals wishing to make statutory notifications, or needing urgent health protection advice regarding management of communicable disease or environmental hazards, can do so through health protection teams or out-of-hours public health/health protection rotas
Public health specialist advice and support with health needs assessment, including data analysis and interpretation, and evidence appraisal, can be accessed through Consultants/Directors of Public Health
Setting budgetary priorities, commissioning or planning health services/interventions, including contract management support and evaluation of resultant outcomes, are also fields of public health expertise, which can be accessed through Consultants/Directors of Public Health
Footnotes
Acknowledgements
Dr Catriona Milošević, Specialty Registrar in Public Health Medicine, NHS Lanarkshire, Scotland; Chris Littlejohn, Specialty Registrar in Public Health, NHS Grampian, Scotland; Dr Stella Botchway, Specialty Registrar in Public Health, Public Health Wales, Preswylfa, Wales; Dr Philip Veal, Specialist Registrar Public Health Medicine, Public Health Agency, Belfast, Northern Ireland; and Mrs Monica Graham, Nurse Consultant Health Protection Service, Public Health Agency, Belfast.