
Abstract
Food allergy is common among children and infants in the western world, and its incidence continues to increase. Because food allergy is dealt with predominantly in primary care, its management constitutes a significant part of the GP's workload. This article aims to provide a practical approach to the management of food allergy in primary care.
The GP curriculum and food allergy in children and young people
No single curriculum statement refers specifically to childhood food allergy, but food-induced allergic reactions are responsible for a variety of symptoms and disorders involving the skin, gastrointestinal and respiratory systems. The following curriculum statements are of particular relevance:
The scale of the problem
Food allergy is an adverse immune response to a specific protein allergen found in a foodstuff. Food allergy in children under 10 in the UK has a prevalence of 3–8%, before gradually decreasing over the next decade of life. Common trigger foods include:
cow's milk eggs fish and seafood nuts (commonly peanuts) soy and wheat some fruits
In extreme cases, anaphylaxis requiring hospitalization can result from exposure; however, most symptoms are much milder and many sufferers remain undiagnosed. The overlap of symptoms with other relatively common primary care presentations including food ‘intolerance’, coeliac disease and non-food allergies makes diagnosis a challenge for GPs. However, delayed diagnosis can result in significant morbidity for the patient and anxiety and worry for the parent or carer.
In its review of allergy services in 2006, the Department of Health concluded that there was considerable variation in the current practice for allergy care, with no agreed treatment pathways, referral criteria or service models. This meant that many people with allergies were practicing self-care or using alternative sources of support rather than the National Health Service (NHS). To address these issues, the National Institute for Health and Clinical Excellence (NICE) published guidelines to aid diagnosis of food allergy in children in primary care (NICE, 2011).
There is a lack of consensus regarding the pathophysiology and therefore classification of allergy. NICE (2011) classifies food allergy into two groups (Fig. 1):
Immunoglobulin E (IgE) mediated—acute, often rapid and onset reactions Non-immunoglobulin E (non-IgE) mediated—delayed and non-acute reactions
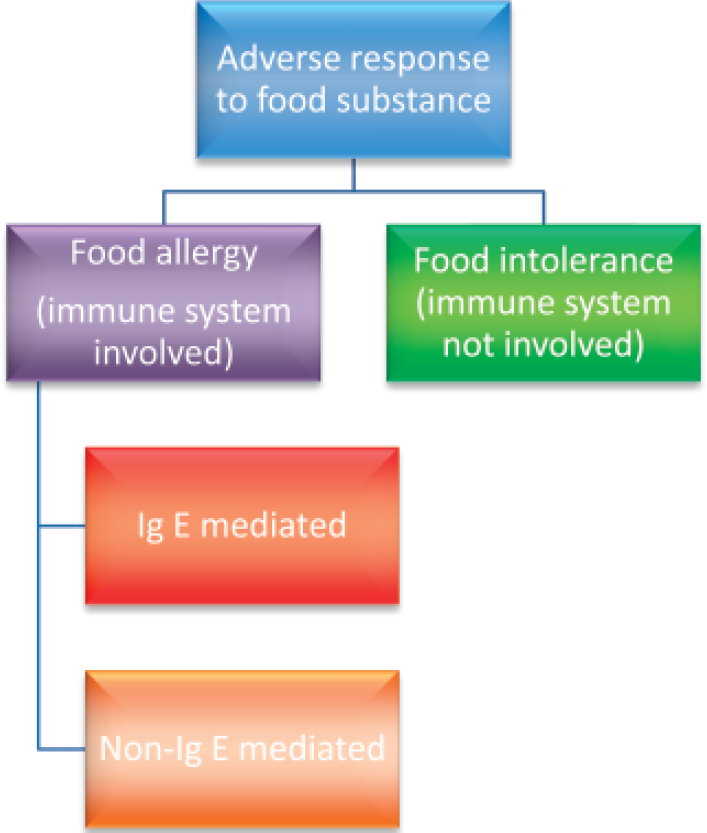
Classification of food allergy and food intolerance.
Making the distinction between these subsets is important because management and prognosis differ. However, in reality, there is often an overlap; hence, the term ‘mixed IgE and non-IgE’ mediated allergic reactions. Clinicians need to have a clear understanding of this if they are to communicate a potentially complex subject clearly to parents/carers.
Food intolerance
This article focuses on the management of food allergy, but a significant proportion of patients presenting with a reaction to a food substance will in fact be suffering from reactions to food, which do not involve the immune system. These are referred to as ‘food intolerances’. Examples are lactase deficiency, leading to lactose intolerance (a metabolic intolerance) and facial flushing in response to monosodium glutamate (a pharmacological intolerance).
Symptoms of food intolerance vary enormously, and there is some overlap with the food allergy symptom spectrum. However, as a general rule, symptoms of atopy are less prevalent, as is a family or personal history of atopy. Features of anaphylaxis and angioedema are absent. A further distinction is that a person with a food intolerance can often tolerate a low ‘dose’ of the suspected allergen, whereas those with food allergy typically cannot.
Initial recognition
Food allergy as a possible diagnosis should be considered in all children presenting with any of the symptoms listed in Fig. 2. Importantly, food allergy should also be suspected in the following groups:
Children whose atopic eczema has not responded to treatment as expected Children whose chronic gastrointestinal symptoms (such as gastro-oesophageal reflux, diarrhoea, abdominal pain, constipation, colic or food refusal) have not settled as expected and Children who are failing to thrive

Symptoms of food allergy.
A thorough history and examination covering the points listed in Boxes 1 and 2 are important as this is the basis of diagnosis in most cases. Laboratory testing is only used to confirm suspected diagnoses. Allergy testing (as offered in supermarkets, health food stores, etc.) in isolation is not helpful as false positives and negatives serve only to confuse the clinical picture.
Symptoms and signs of food allergy
Many symptoms of food allergy are common to both IgE-and non-IgE-mediated reactions, but it is important to attempt to identify children with IgE-mediated allergy due to their risk of anaphylactic reactions in the future. The typical symptoms and differences between children suffering from IgE- and non-IgE-mediated allergy are summarized in Fig. 2.
Allergy—focused clinical history
Personal history of atopic disease Family history of atopic disease or food allergy Details of any foods that are avoided and why Presenting symptoms and other symptoms that may be associated with food allergy:
Age at first onset Speed of onset Duration, severity and frequency Setting of reaction (e.g. at school or home) Reproducibility of symptoms on repeated exposure What food and how much exposure to it causes a reaction Cultural and religious factors that affect the child's diet Who suspects the food allergy What the suspected allergen is The child's feeding history, age of weaning and whether they were breastfed or formula fed Details of previous treatment and any response to this Any response to the elimination and reintroduction of foods
Allergy—focused clinical examination
Short stature Thin arms and legs Hair and skin in poor condition Wasted buttocks Oedema, wasted facial appearance and lethargy (extreme malnutrition) Anaemia
Wheeze
Abdominal distention may be a sign of non-IgE-mediated food allergy
Signs of pruritis Erythema Atopic eczema Anaemia
Anaphylaxis
IgE-mediated allergic reactions tend to have a rapid onset and present acutely. They are more common in children with a personal or family history of atopy (i.e. asthma, eczema and/or allergic rhinitis).
The most severe type of allergic reaction is anaphylaxis, which is almost always IgE mediated. A previous InnovAiT article summarizes the recognition of acute anaphylaxis and its management in primary care (Simon, 2011).
The symptoms of anaphylaxis usually start 3–60 minutes after contact with the allergen. As well as an acute onset of illness, true anaphylactic reactions always involves life threatening effects on:
the airway and/or the breathing and/or the circulatory system
Gastrointestinal symptoms such as acute colicky abdominal pain, vomiting or diarrhoea and skin and mucosal changes (flushing, urticaria and angioedema) are often present but can be subtle or absent in up to 20% of anaphylactic reactions. Skin or mucosal changes alone are not a sign of an anaphylactic reaction.
Less severe IgE-mediated reactions
Less severe IgE-mediated reactions tend to occur within 2 hours of eating triggering foods. They can also present with the following symptoms but crucially these do not compromise the airway and are not life threatening:
Pruritus (may affect the mouth) Erythema Acute urticaria (Fig. 3) Angio-oedema—most commonly affecting the lips, face and periorbital area (Fig. 4) Nausea and vomiting, colicky abdominal pain and diarrhoea Upper respiratory tract symptoms including nasal itching, sneezing, nasal congestion, rhinorrhea and sometimes conjunctivitis

Severe urticarial rash.

Acute angiodoema of lips.
Lower respiratory tract symptoms such as chest tightness, cough and shortness of breath can be associated with IgE-mediated reactions but are also common in non-IgE-mediated reactions too. It is rare for a food allergy to present with respiratory tract symptoms alone.
Non-IgE-mediated reactions
Non-IgE-mediated food allergy tends to be harder to spot as the child does not have an acute reaction to the food responsible. Some symptoms overlap with IgE-mediated allergy and these include:
Pruritus Erythema and Lower respiratory tract symptoms including cough, chest tightness and shortness of breath
Gastrointestinal symptoms are common and include:
Gastro-oesophageal reflux Loose or frequent stools that may contain blood and/or mucus Constipation Abdominal pain or infantile colic Perianal redness
Children with atopic eczema are more likely to develop non-IgE-mediated allergy and this is more common in those with severe eczema. The child may look pale and may fail to grow as expected or refuse food. It is useful to plot serial weight and height measurements on an appropriate centile chart. A sustained unintentional fall in weight by two or more centiles is indicative of malnutrition and can be compatible with non-IgE-mediated food allergy.
Allergy testing
IgE-mediated allergy
In patients where IgE-mediated allergy is suspected, NICE (2011) recommends just two forms of investigation at a primary care level:
skin prick testing (SPT) and/or serum testing of food substance specific IgE antibodies
These tests and their usage are discussed further in a previous InnovAiT article (Morris, 2009). On a practical level, the choice of test will depend on the clinical history, availability of tests locally and the preference of the patient or parent.
SPT is cheaper and less invasive than specific IgE testing; however, the accuracy of results can be affected by medications including antihistamines. SPT is contraindicated in severe allergic reactions or in settings that lack facilities to manage anaphylactic reactions (although GP surgeries that vaccinate children should all have such facilities).
In contrast, IgE specific blood tests are not affected by medications and remain the test of choice when it is considered necessary to identify a specific allergen. However, results are not immediate and rates of false positives are higher than with SPT.
Non-IgE-mediated allergy
For children with suspected non-IgE-mediated allergy, the first step in confirming diagnosis is to try eliminating the suspected allergen for an agreed period of time before reintroducing it. NICE (2011) recommends 2–6 weeks. Where more than one allergy is suspected, each food should be eliminated separately. For children with persistent gastrointestinal symptoms, anaemia or failure thrive, it is also important to consider coeliac disease as a cause for symptoms and exclude this with appropriate blood tests (NICE, 2009).
Eliminating suspect foods from a child's diet one by one can be a time consuming process and depends heavily on patient/parent/carer understanding and concordance with the elimination diet. Elimination diets can also result in nutritional deficiency themselves, particularly if the food being eliminated forms a large part of the child's diet (such as milk). In most cases, the involvement of a dietician is likely to be needed.
Alternative allergy tests
Parents may well ask about the possibility of other alternative allergy tests. NICE (2011) examined the evidence for the efficacy of Vega testing, applied kinesiology, hair analysis and serum-specific IgG testing. They conclude that none of these tests have sufficient evidence to support their use in primary care.
Management
The first aim of management in both IgE-mediated allergy and non-IgE-mediated allergy is total allergen avoidance. It is usually best to involve a dietician in this process to educate the child and parents about foods containing the food to which the child is allergic and also about food label interpretation, cross reactivity and food contamination.
Information provision
As allergen avoidance is the cornerstone of management of childhood food allergy, information provision is crucial. It is important to educate not only the child and parents/carers but also anyone else who is likely to be looking after the child, such as teachers, childminders and grandparents. Information should be tailored to the needs of the individual and will depend on the suspected diagnosis, the probability of that diagnosis, whether there is a risk of a severe reaction and the circumstances and wishes of the child and family concerned.
Wherever possible back up any verbal advice provided with written information too. Reliable resources for further information for children and their parents about food allergy can be found in Box 3.
Antihistamines
For children with mild IgE-mediated allergy who are accidentally exposed to trigger foods, antihistamines, such as chlorphenamine, may be prescribed for symptom control.
Adrenaline auto-injectors for anaphylaxis
An auto-injector device allows the child or any bystanders to deliver a rapid dose of adrenaline as first aid at the first signs of anaphylaxis. As the risk of an individual suffering recurrent anaphylactic reaction is relatively high, provide an adrenaline auto-injector device to any child who has suffered a food-induced anaphylactic reaction. Criteria for prescription to other groups are less clear. Consider prescribing an auto-injector pen to children who have had moderate (classified as mild laryngeal oedema indicated by voice change or sensation of throat tightening) or severe (classified as marked dyspnoea or cardiovascular symptoms) allergic reactions to food in the past.
Auto-injector devices consist of a fully assembled syringe and needle. Two adrenaline auto-injector devices are available in the UK at present, the Epipen and the Anapen. Both come in adult (300 mcg) and paediatric doses (150 mcg for children weighing 15–30 kg) and are available on NHS prescription.
Injection should only be given into the anterolateral aspect of the mid-thigh and can be given through clothing if needed. Children (if old enough) and others likely to be with them, such as parents, grandparents and school teacher should be taught how to use the device that is prescribed. Enough devices should be supplied so that a device is available for use in each of the locations that the child is most likely to be in (for example one at home, one in the car and one at school). Most children will require more than one device. Use of and care for adrenaline auto-injectors are covered in more depth in the InnovAiT article on anaphylaxis (Simon, 2011).
Cow's milk allergy
Cow's milk allergy (CMA) is the most common food allergy in infancy and should not be confused with lactose intolerance. It can be either IgE mediated or non-IgE mediated. Non-IgE-mediated CMA is thought to affect 1–2% of infants and up to 50% of infants with CMA have other food allergies.
As milk and milk products are found in so many foods, a dietician is always needed to advise on alternative nutritional sources, weaning, avoidance of milk-containing foods and the timing of reintroduction of milk-containing foods. Alternative milk-free nutritional choices are summarized in Table 1. Choice will depend on whether the allergy is IgE or non-IgE mediated, the age of the child and whether the mother is breastfeeding or not. It is important to note that 20% of children with non-IgE CMA have coexisting soy allergy and so soy-based formula is not recommended for this group. Most children with either IgE-mediated or non-IgE-mediated CMA will develop tolerance to cow's milk by school age.
Appropriate alternative milk substitutes for infants with CMA

Management of co-morbid conditions
For children with food allergy, it is important to optimize the management of other coexisting atopic conditions, especially asthma. It is thought that many ‘asthma’- related deaths may in fact be food allergy induced, and children with a history of asthma are more likely to experience severe (including anaphylactic) reactions to food allergens.
Useful resources for children, parents/carers and GPs
Allergy UK. Website: www.allergyuk.org—includes useful patient information links Anaphylaxis UK. Website: www.anaphylaxis.org.uk
Food Standards Agency. Website: www.food.gov.uk/safereating/allergyintol/—provides information on food labelling
Patient.co.uk. Website: www.patient.co.uk/doctor/Food-Intolerance-and-Food-Allergy.htm—excellent summary of food allergy and intolerance with further links to useful sites Royal College of Paediatrics and Child Health. Website: www.rcpch.ac.uk/sites/default/files/2011_RCPCHCarePathway-FoodAllergy_v6_(16.26).pdf.pdf—useful care pathway outlining ideal management of children with food allergy
Referral for specialist care
Although many children with food allergy can be safely and successfully managed in primary care, a significant minority will require referral to secondary care services. NICE (2011) recommends that children are referred for specialist paediatric or allergy assessment if:
they have faltering growth with accompanying gastrointestinal symptoms they have not responded to a single allergen elimination diet they have confirmed IgE-mediated food allergy and concurrent asthma they have a history of an acute systemic allergic reaction there is ongoing diagnostic uncertainty or parental concern
In addition, the UK Resuscitation Council 2008) recommends that any child who has an acute anaphylactic reaction is referred for assessment by a specialist allergy service. Urgency of referral depends on severity and frequency of symptoms.
Prognosis
Many children ‘grow out’ of their allergy to eggs, milk, wheat and soya. One-third of all adults and children lose their clinical reactivity to food allergens after 1–2 years of food elimination diets, although loss of this tolerance is common too. However, sensitivity to peanuts, seafood, fish and tree nuts is rarely lost.
Vaccinations
Parents/carers of children with food allergies are often concerned that a food allergy might have implications for future vaccination. In fact, a vaccination is only absolutely contraindicated in a patient with confirmed anaphylactic reaction to a previous dose of a vaccine containing the same antigen or another component contained in that vaccine, e.g. neomycin, streptomycin or polymyxin B. Patients with a confirmed anaphylactic reaction to egg should not receive influenza or yellow fever vaccines.
Measles, mumps and rubella (MMR) vaccine can safely be given to most children with a previous history of allergy after ingestion of egg or egg-containing food, and vaccination can take place in the GP surgery. For the small number of individuals who have a history of confirmed anaphylactic reaction after any egg-containing food, specialist advice should be sought with a view to immunization under controlled conditions usually on the hospital paediatric ward.
Where there is doubt, rather than withholding a vaccine, advice should be sought from a consultant paediatrician or other appropriate colleague. More information is available from the Department of Health's ‘Green Book’ (Department of Health, 2007).
Key points
Food allergy is common, and its prevalence is increasing An accurate thorough history and examination are essential when assessing the child with allergy Management strategies depend on whether the child is thought to have IgE- or non-IgE-mediated allergy Timely provision of appropriate information is an important element of successful management of allergy Referral to secondary care services should be considered in severe or non-responsive allergy
Footnotes
Acknowledgements
The authors would like to thank Dr Simon Bedwani, MBBS, MRCPCH; Consultant Paediatrician, Royal Cornwall Hospital, for his advice on the first draft of this article.