
Abstract
Infantile eczema is an inflammatory itchy skin condition that affects at least 10% of infants at some stage in their lives. It can continue into childhood after the age of 18 months or adolescence where it is referred to as atopic eczema. There are various treatment options for infantile eczema according to its severity. The key role of the GP is to educate parents and carers about the diagnosis and management of eczema and provide support when required.
GP curriculum and infantile eczema
Eczema is listed as a common and important condition forming part of the knowledge-based
Recognize how common eczema is among the general population Demonstrate a reasoned approach to the diagnosis of skin symptoms using history, examination, incremental investigations and referral Ensure that eczema is not dismissed as trivial or unimportant by health care professionals Appreciate the importance of the social and psychological impact of eczema on the patient's quality of life, for example, sleep deprivation as a result of itching Appreciate the importance of the social and psychological impact of skin problems on the patient's family and friends Identify the patient's, parents' or carers' health beliefs regarding skin problems and reinforce, modify or challenge these beliefs as appropriate Advise patients, parents or carers regarding lifestyle interventions Describe and implement the key national guidelines that influence health care provision for skin problems Coordinate with other primary care health care professionals, dermatologists and other appropriate specialists, leading to effective and appropriate acute and chronic disease management, including prevention and rehabilitation Make timely appropriate referrals on behalf of patients to specialist services Intervene urgently when patients present with an emergency skin problems such as eczema herpeticum
Presentation of infantile eczema
Infants under the age of 18 months commonly present with itchy, vesicular weepy eczema on the face, scalp and extensor surfaces of arms and legs (Fig. 1). In later childhood, the rash develops into a dry, scaly itchy rash commonly within the inner creases of the elbows and knees. Infantile eczema affects both sexes equally and usually starts in the first weeks or months of life.

Facial infantile eczema.
Criteria for diagnosis
Infantile eczema should be diagnosed when an infant has an itchy skin condition (or reported scratching or rubbing). Three or more of the following features should also be present:
Visible dermatitis on the cheeks, forehead and/or extensor areas History of itching around the cheeks, forehead and/or outer limbs General dry skin History of eczema or hay fever in a first-degree relative of the infant
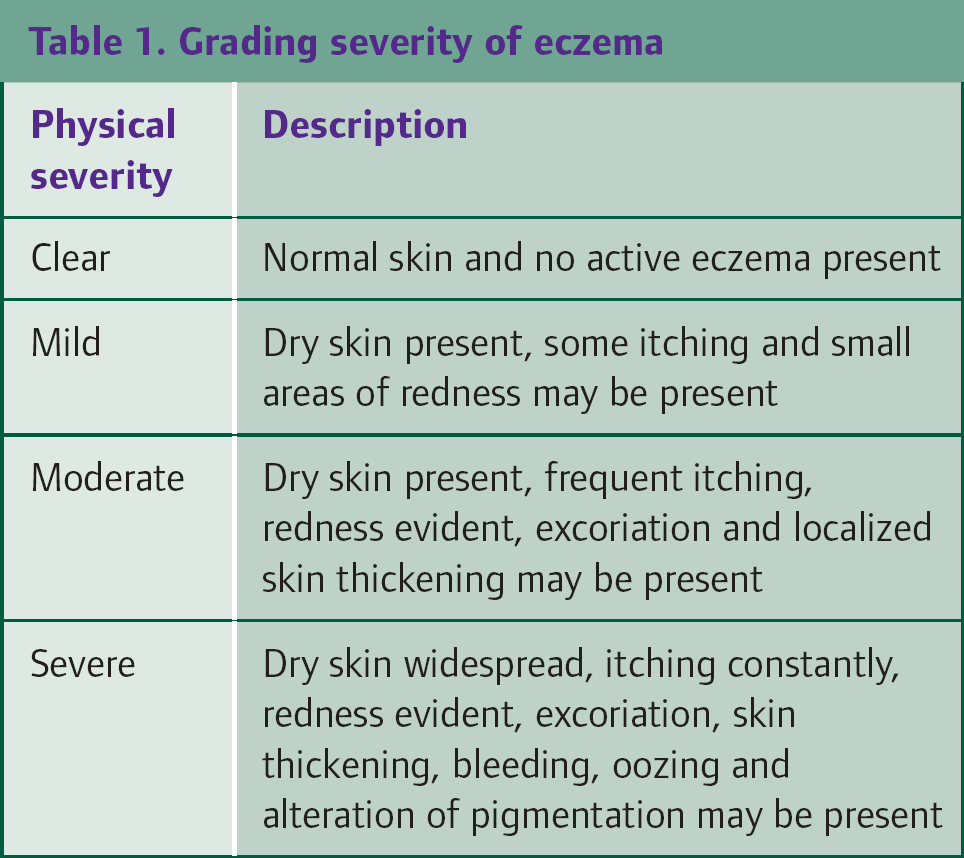
Infantile eczema can be graded according to clinical presentation. It can be classified as mild, moderate or severe (Table 1).
When assessing an infant, it is important to make a general assessment at initial presentation. Check for any comorbidities and explore the home setting of the infant. Determining if any siblings have eczema can give a greater understanding of parental and carers' anxieties. There is not always a direct correlation between severity of infantile eczema and the impact of the eczema on quality of life.
Differential diagnosis of infantile eczema
Infantile eczema may predispose or coexist with other disorders, such as scabies, herpes simplex infection, bacterial infections and superficial fungal infections. Psoriasis, contact dermatitis and seborrhoeic dermatitis may also present similarly to infantile eczema. Some rare genetic disorders feature a pattern of cutaneous inflammation like infantile eczema. Such examples include Wiskott–Aldrich syndrome, anhidrotic ectodermal dysplasia and phenylketonuria.
Investigations and management of trigger factors
There are a number of potential trigger factors linked to infantile eczema. These should be carefully explored when assessing the infant.
Irritants such as soaps and detergents
Soaps and detergents (including shampoos) can be possible trigger factors for infantile eczema. If irritants have been identified, parents and carers should be advised to use emollients, including specialist wash products to replace potential irritants.
Contact allergens
The possibility of contact allergens should be considered in infants with an exacerbation of previously controlled eczema or with reactions to topical treatments. Most infants with mild atopic eczema do not need testing for allergies. Estimation of immunoglobulin E (IgE) and specific radioallergosorbent tests (RASTs) can only confirm the atopic nature of the condition. The use of high street or internet allergy tests should similarly not be advised to parents and carers as there is no evidence of their value in management of infantile eczema.
Food allergens
The role of food allergy in infantile eczema is controversial. The National Institute for Health and Clinical Excellence (NICE) guidance on atopic eczema in children (NICE, 2007) suggests food allergy should be considered in infants with moderate or severe eczema that has not been controlled by optimum management, particularly if associated with gut dysmotility (colic or vomiting) or failure to thrive. It recommends consideration of a 6–8 week trial of anextensively hydrolysed protein formula or amino acid formula in place of cow's milk formula for bottle-fed infants under 6 months with moderate or severe atopic eczema that has not been controlled by optimal topical therapy. Specialist advice from a dietician is advised for any infant following a cow's milk-free diet for longer than 8 weeks.
Mother's diet
It is not known if altering a mother's diet, when breastfeeding, by excluding milk, eggs, wheat and a range of other foods has any impact on reducing the severity of infantile eczema. However, if a food allergy is strongly suspected, NICE recommends that an allergen-specific exclusion diet can be tried (NICE, 2007).
Endogenous factors
Factors such as stress, humidity and extremes in weather may exacerbate infantile eczema. It is not entirely clear what role such factors play in a flare-up of eczema but they should be avoided wherever possible.
Management of infantile eczema
It is important to adopt a stepped approach to the management of infantile eczema, tailored according to severity. Regardless of the severity, educate all parents and carers about the use of emollients as a basis of management. Start treatment for flares of infantile eczema as soon as signs and symptoms appear and continue for 48 hours after symptoms subside. Offer regular follow-up to parents and carers especially if they feel that their infant has not improved or if they feel that their concerns previously have been dismissed as trivial by other health professionals.
Education
Provide information regarding the infantile eczema, identification of triggering factors, the role of different therapies and their effectiveness and safe use at the point of diagnosis. Treatment options should take into account the infant's cultural practices related to skin care, such as oiling the skin and how the infant bathes. Give information in a clear manner in verbal and written forms (Box 1) and supplement it with practical demonstrations.
Information should cover the following:
How much of the treatment to use—include the correct quantities of topical treatments (Table 2) How often to apply treatments When and how to step up and down treatment How to recognize and treat flares of infantile eczema (increased dryness, itchiness, redness, swelling and general irritability) and Bacterial infection
Quantities of emollients and corticosteroids to prescribe

Emollients
Emollients have a number of different roles in infantile eczema. They
soften the skin reduce itchiness increase the efficacy of topical corticosteroids and have a steroid-sparing action
Natural surface oils tend to be deficient in infantile eczema. Emollients replace these surface oils and help in preventing irritant materials, infection and allergy-inducing substances from entering the skin and, conversely, water leaving the skin.
Infants with eczema should have ongoing treatment with emollients. A choice of emollients for every day moisturizing, washing and bathing should be provided (Table 3). A cream or lotion is best in mild dryness, whereas a thicker cream or ointment is best in cases of moderate to severe dryness. Ointments should not be used for weeping skin. Paraffinbased emollients are flammable so should be kept away from lights or flames.

Educate parents and carers about regular application of emollients to the whole body even when the eczema is under control and while using all other treatments. Advise parents and carers to use emollients including wash products instead of soaps, detergent-based wash products and shampoos. Provide leave-on emollients in large quantities (250–500 g weekly) and ensure that these are available at the nursery as well as at home.
Advise parents and carers to apply emollients liberally and at least two to four times a day. Emollients should be particularly used during and after bathing. Where different emollient products are used at the same time, different products should be applied one at a time with several minutes between applications. The emollient should be applied smoothly in the general direction of hair growth rather than rubbing it in. This helps to prevent accumulation at hair bases, which can cause folliculitis. Prescribe an alternative emollient if the infant has experienced irritation. Emphasize that emollients should be continued even after infantile eczema has cleared to help prevent flare-ups.
Information for patients about treatment of infantile eczema
Infantile eczema affects 10% of infants and usually disappears during childhood Infantile eczema cannot be cured, but there are many ways of controlling it Emollients should be applied every day to help the outer layer of your skin function as a barrier to your environment. Aim to moisturize the skin regularly—maybe as often as six times daily Wash with a bath emollient instead of soap. Hot water can make itching worse, so make sure bath water is not too hot Topical steroid creams usually settle the redness and itchiness when eczema is active Your infant may need intermittent courses of steroid cream to control eczema Emollients should be used even when the skin is free of eczema to help prevent flare-ups
National Eczema Society, Hill House, Highgate Hill, London N19 5NA www.eczema.org
Emollients can become contaminated with bacteria. Pump dispensers minimize the risk of bacterial contamination. If the emollient is in a pot, fingers should not be used but the required amount should be removed with a clean spoon or spatula. Emollients should not be shared with others.
Topical steroids
NICE recommends a stepped approach, matching the potency of topical corticosteroids with severity of eczema (NICE, 2007). For infants under 12 months, they suggest
Using a mild potency topical corticosteroid for mild atopic eczema Using a moderate potency topical corticosteroid for moderate atopic eczema Not to use potent preparations in infants without specialist dermatological advice
The potency of topical corticosteroids is dependent on particular properties such as moiety, formulation and penetration into the skin rather than simply concentration (Table 4). Check that parents and carers are not using any other creams that may contain steroids.
Examples of topical corticosteroid potencies

Topical corticosteroids should be applied to areas of active eczema or eczema that has been active in the past 48 hours. The amount applied should be sufficient to cover areas of inflamed skin even if the skin is excoriated. Prescribe topical corticosteroids for application only once or twice daily. The ‘fingertip unit’ should be used as a guide of determining the amount of topical corticosteroid to apply (Table 5).
A guide for calculating ‘fingertip units’ needed for treatment with topical corticosteroids for infants

The benefits and harms of treatment with topical corticosteroids to infants with eczema should be discussed with parents and carers. Benefits outweigh the possible harm of topical corticosteroids when applied correctly. Exclude secondary bacterial infection if infantile eczema has not been controlled within 7–14 days after application of mild or moderately potent corticosteroids. Reported local adverse effects of topical corticosteroids include skin thinning, bruising, folliculitis, pruritus, allergic contact dermatitis and spread of fungal infection. The Scottish Intercollegiate Guidelines Network (SIGN) advises that infants treated with intermittent courses of topical corticosteroids should be reviewed every 3–6 months to assess their skin and to help reduce potential reversible atrophic changes (SIGN, 2011).
Dressings and wet wrap therapy
A variety of dry wrap occlusive or medicated bandages can be used in the management of infantile eczema (Table 6). Occlusive medicated dressings and dry bandages are not recommended in the treatment of infected infantile eczema. Medicated bandages or dry bandages can be used with emollient alone or with emollients and topical corticosteroids in the short-term treatment of flares for 7–14 days.

Wet wrapping consists of two layers of open-weave tubular bandage that can be applied over topical preparations. The bottom layer is soaked in warm water, squeezed out and then placed onto the topical preparation on the skin. The top layer is dry. Wet wraps are available in bandages or garment forms. They can be worn under nightwear or ordinary clothes. Whole-body occlusive dressing (including wet therapy) or dry bandages should only be initiated by a health care professional trained in their use and is not recommended as first-line treatment.
Treatment of infection
It is important to educate all parents and carers on how to recognize the signs and symptoms of bacterial infection with Staphylococcus and/or Streptococcus. Bacterial infection with Staphylococcus and/or Streptococcus typically presents with rapid worsening of eczema with weeping, pustules, crusts and associated fever and malaise. New supplies of topical medications should be provided after treatment of infection since products in open containers can be contaminated with microorganisms and can actually be a source of infection. Routine swabs from the skin are not recommended except when there is suspicion of microorganisms other than Staphylococcus, atypical features or if antibiotic resistance is relevant.
NICE (2007) recommends flucloxacillin as the first-line treatment for bacterial infections in infantile eczema for both Staphylococcus aureus and Streptococcal infections.
Erythromycin can be used for those with penicillin allergy or in the case of flucloxacillin resistance. Clarithromycin can be used if erythromycin is not well tolerated. Topical antibiotics including those combined with topical corticosteroids can be used in patients with clinical infection in localized areas but should be used for no longer than 2 weeks.
Antiseptics such as triclosan or chlorhexidine can be used to decrease bacterial load in those infants with recurrently infected eczema. Long-term use should be avoided.
Eczema herpeticum
Eczema herpeticum is a severe primary herpes infection that can occur in individuals with eczema (Fig. 2). Consider Herpes simplex (HSV) in those infants whose infected eczema fails to respond to antibiotics and topical corticosteroid therapy. Signs of eczema herpeticum are
Areas of rapidly worsening painful eczema Clustered blisters consistent with early-stage cold cores Punched-out erosions (circular, depressed and ulcerated lesions), usually 1–3 mm in diameter and of uniform in appearance Possible fever, lethargy or distress

Eczema herpeticum.
Eczema herpeticum can affect multiple organs, including the eyes, brain, lungs and liver. It can lead to herpetic encephalitis and death. Treatment with oral acyclovir is recommended even if the infection is localized. Urgent same day assessment by a paediatrician or dermatologist is essential in all suspected cases. If eczema herpeticum involves skin around the eyes, same day ophthalmological advice should be obtained.
Antihistamines
Regular oral antihistamine therapy is not routinely advised in the management of infantile eczema. However, a 7–14 days trial of age-appropriate antihistamine therapy can be used for infants over 6 months during an acute flare-up if there is debilitating sleep disturbance. This can be repeated during episodes of acute flares if appropriate.
Complementary therapies
Homeopathy, herbal medicine, massages and food supplements have been suggested as complementary treatments in the management of infantile eczema. However, none of these treatments have been adequately assessed for efficacy or harm in clinical studies.
Educate parents and carers about caution needed when using complementary therapies, especially for those products not labelled in English or not including information regarding safe usage. Inform parents and carers that topical corticosteroids are often deliberately added to some herbal products to ensure that they work and about the link between liver toxicity and some Chinese herbal medicines used to treat infantile eczema. Parents and carers should be encouraged to inform their health care professional if they would still like to use complementary therapies. Advise them to continue using emollient therapy alongside these.
Indications for referral
Box 2 summarizes referral guidance for children with infantile eczema.
Indications for referral for specialist care
Eczema herpeticum (to paediatrics, dermatology and/or ophthalmology)
Severe eczema that has not responded to optimal topical therapy within 1 week Bacterial infection of eczema that has not responded to antibiotic treatment
The diagnosis is uncertain Optimum management has not controlled infantile eczema based on subjective assessment by parents or carers The child is failing to thrive Infantile eczema on the face has not responded to appropriate treatment The parent or carer would benefit from specialist advice on treatment application (such as bandaging techniques) Contact allergic dermatitis is suspected Infantile eczema is giving rise to significant social or psychological problems, such as disturbance of sleep Infantile eczema is associated with severe and recurrent infections, especially deep abscesses or pneumonia
Note: These are suggested timescales for referral only. Clinical judgement is needed to determine urgency of referral and this may vary according to individual circumstances.
Psychological support
Psychological support is also recommended for parents/carers and those infants with infantile eczema who have responded to optimum management but for whom the impact of infantile eczema on quality of life and psychosocial well-being has not improved. Community dermatology nurses can provide a good support network to parents and carers, especially in cases of moderate or severe infantile eczema.
Key points
Infantile eczema affects at least 10% of infants at some stage HSV, Staphylococcal and Streptococcal infection can be superimposed on infantile eczema Potential trigger factors can be linked to infantile eczema and should be explored when assessing an infant Topical corticosteroids should be used on areas of active eczema or that have been active in the past 48 hours Clear information regarding recognizing infection and the possibility of eczema herpeticum should be provided Psychological therapy may be needed when the quality of life or psychosocial well-being of parents or carers is compromised