
Abstract
Migraine affects 15% of the UK adult population and occurs three times more frequently in women compared with men. It is a common reason for patients to consult their GP. The primary aim in the management of migraine is the control of symptoms to minimise the impact on the patient's lifestyle. Expectations of a complete cure are unrealistic. However, under-treatment is neither cost-effective nor time-effective and different options should be offered until the most beneficial treatment plan is reached. As migraine typically varies with time, patients’ needs may change and the differential diagnosis should be reviewed regularly.
The GP curriculum and migraine
Manage primary contact with patients who have a neurological problem.
Understand the principles of treatment for common neurological conditions managed largely in primary care.
Describe the indications for referral to a neurologist for chronic conditions requiring ongoing specialist management.
Describe the importance of continuity of care for patients with chronic neurological conditions.
Management steps
In adults, there are four main steps in effective migraine management [British Association for the Study of Headache (BASH, 2010)]:
Make a correct diagnosis
Provide explanation and reassurance
Identify and avoid predisposing or trigger factors
Provide intervention (both drug and non-drug)
Diagnosis is outside the scope of this article. Explanation is important as it promotes realistic patient expectations. Reassurance of the benign nature of most migraines can also be helpful; it may be all that is required in mild cases.
Predisposing and trigger factors
Predisposing factors may be distinguished from trigger factors by the fact that the former are not always avoidable but may be treatable. Trigger factors are not ‘treatable’ but can be avoided. There are several well-documented predisposing and trigger factors (see Table 1). If present, these should always be addressed prior to considering prophylactic pharmacological management, as avoiding them may reduce the incidence of migraine by up to 50%.
Predisposing and trigger factors for migraine
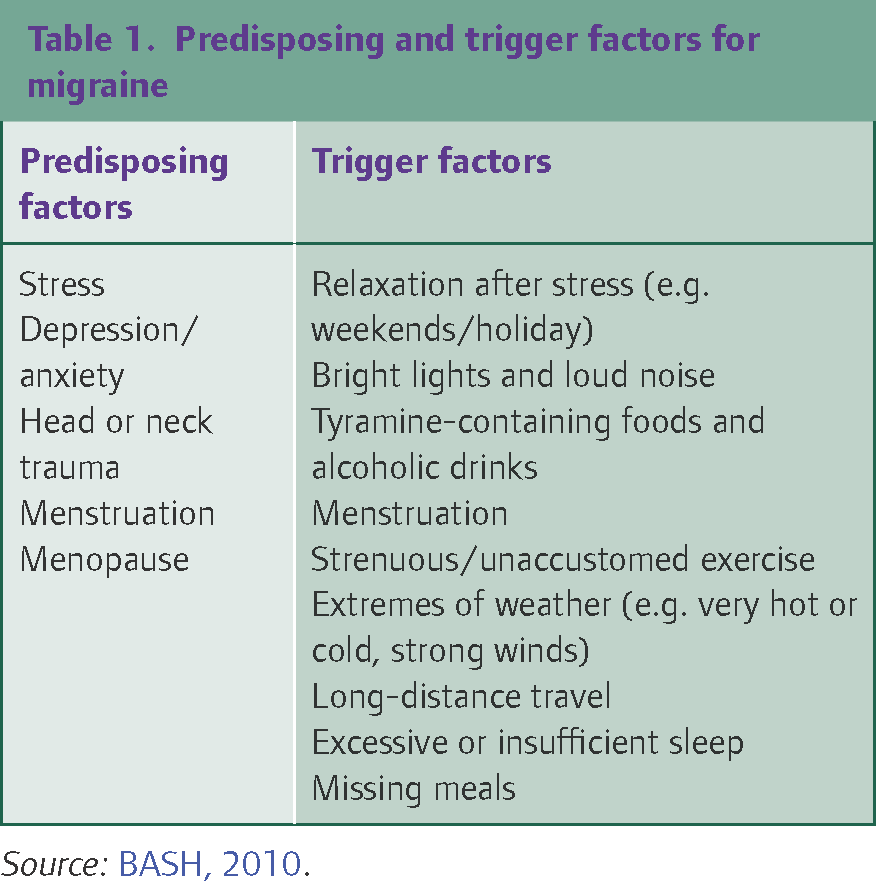
Source: BASH, 2010.
Menstruation has been listed both as a trigger and a predisposing factor, as it can be managed with measures to inhibit ovulation. Food may be considered to be a trigger when the onset of migraine is within 6 hours of consumption, the effect is reproducible and withdrawal leads to improvement. Dietary triggers are implicated in 20% of migraine sufferers (BASH, 2010). Tyramine-containing foods include yeast extracts, cheese (especially stilton, camembert, gorgonzola and brie), pickled herring and red wines.
When migraine attacks are frequent patients should be provided with a list of typical triggers and predisposing factors. They should be encouraged to keep a diary in which the presence of these factors is recorded, whether or not a migraine attack occurs (although migraines should also be recorded). The incidence of trigger factors with migraine occurrence can then be compared. The diary is best reviewed after at least five attacks. Patients can access a diary from the website of the patient support group, Migraine Trust (see further information). However, it is important not to place too much emphasis on trigger factors, since this may induce introspection.
Pharmacological management of acute migraine
Treatment of an acute attack of migraine should ideally be combined with rest in a darkened room, although remember that the main aim of treatment is to allow patients to continue with their normal activities as much as possible. When initiating acute treatment for migraine, the risks of medication overuse headache should be discussed with the patient. It is also worth bearing in mind that, in view of the gastric stasis associated with migraine, it is advisable to always use medications at their full dosage.
The treatment approach is stepwise, with patients generally being advised to move to the next step if there have been three consecutive failures of treatment (BASH, 2010). When considering the need for a step-up of treatment it is always important to review the patient's adherence with therapy and reconsider the diagnosis.
Step 1: Simple analgesic with or without an anti-emetic
Acute migraine can often be managed with some over the counter (OTC) medications, including aspirin (600–900mg every 4–6 hours as needed) or ibuprofen. Although aspirin is now less often used as an analgesic, it is known to be effective for migraine. Paracetamol is recommended for mild to moderate migraine but there is little evidence for its sole use (Scottish Intercollegiate Guidelines Network (SIGN), 2008). Codeine and dihydrocodeine are frequently found in OTC combination analgesics intended for migraine relief. However, these should be avoided due to their side effects of nausea, delayed gastric emptying and the higher risk of precipitating medication overuse headache compared NSAIDs (BASH, 2010).
Prescription medications may also be required, including the NSAIDs naproxen and diclofenac, as well as tolfenamic acid (200mg as an immediate dose, repeated after 1–2 hours if necessary), which is specifically licensed for migraine. Contraindications to NSAID use, including asthma and peptic ulceration should be remembered (BASH, 2010).
Effective, fast-acting anti-emetics include metoclopramide, domperidone and prochlorperazine. Domperidone has an advantage over metoclopramide in that it is less sedating and has a reduced risk of extrapyramidal side-effects. Prochlorperazine can be prescribed as a buccal preparation (Buccastem), which might be helpful in the context of the nausea often associated with migraine.
Convenient OTC preparations involving a combination of analgesic and anti-emetic include MigraMax [lysine acetylsalicylate 1620mg (equivalent to aspirin 900mg) plus metoclopramide 10mg per sachet] and Paramax (paracetamol 500mg plus metoclopramide 5mg per sachet). Although Migraleve is marketed to appeal to migraine sufferers, the fact it contains codeine makes it less desirable than these other preparations.
If nausea and vomiting preclude the use of oral preparations, consider diclofenac suppositories at a dose of 100mg (up to 200mg in 24 hours). These can be combined with domperidone suppositories at doses of 30–60mg (up to 120mg in 24 hours) (BASH, 2010).
Step 2: Triptans
Triptans are highly selective agonists of 5-HT1 (serotonin) receptors at the nerve terminals that supply pain-sensitive vascular and meningeal structures. They should be administered at the start of the headache phase, when it is mild, as they are ineffective if taken during the aura. Concomitant use of a prokinetic agent such as domperidone should be considered when the triptan is taken orally (BASH, 2010).
The cheapest triptan, and that with the most clinical familiarity, is sumatriptan. It should be commenced at a 50mg dose, for which a dispersible version (Radis 50mg) is also available. If the response is inadequate the 100mg tablet or 20mg nasal spray may be used. If needed the dose of sumatriptan can be repeated after 2 hours (to a maximum daily dose of 300mg orally or 40mg intranasally). Sumatriptan is the only triptan that has a subcutaneous formulation (at a 6-mg dose, to a maximum of 12mg in 24 hours), which is particularly useful if there is vomiting (BASH, 2010).
The sumatriptan nasal spray is not useful if vomiting precludes oral therapy, as its bioavailability largely depends on ingestion. Zolmitriptan is more useful in this circumstance, as up to 30% is absorbed through the nasal mucosa (BASH, 2010). High dose rizatriptan and eletriptan have demonstrated greater efficacy for initial pain relief compared with sumatriptan. Naratriptan and frovatriptan are less effective than sumatriptan but are associated with less adverse effects (BASH, 2004).
A troublesome limitation of the triptans is that they may be associated with return of symptoms within 48 hours. This relapse affects 20–50% of patients who have initially responded (BASH, 2004). In patients who relapse within a short time during a single attack the triptan dose may be repeated after a minimum of 2 hours. However, repeated dosing can give rise to recurring rebound over several days; therefore, naproxen or tolfenamic acid may be preferable for the first or second relapse. Rizatriptan, eletriptan and almotriptan are associated with more sustained pain relief than sumatriptan. Naratriptan, eletriptan and frovatriptan are considered to be associated with lower rates of consistent relapse (BASH, 2010).
To summarise, sumatriptan is recommended as the first-line triptan. If it is ineffective, the dose can be increased after reviewing the diagnosis. Failing this, the route of administration should be changed. If the response continues to be inadequate, consider a change in the type of triptan, according to the drug's individual characteristics, as several trials have observed that patients with a poor response to one triptan may benefit from another in subsequent attacks (BASH, 2010). Table 2 illustrates the cost comparison and useful characteristics of the triptans available.
Comparison of the key features of currently available triptans

Source: BASH, 2010; SIGN, 2008; BNF, 2012.
Side effects of the triptans include feelings of paraesthesia, heat, heaviness, pressure, or tightness in any part of the body (including the throat and chest). Flushing, dizziness, weakness, fatigue, nausea and vomiting have also been reported (British National Formulary (BNF), 2012).
Contraindications include ischaemic heart disease, Prinzmetal's angina and uncontrolled hypertension. Caution is advised when prescribing for the elderly or those taking vasoconstricting drugs (BNF, 2012).
Step 3: Combination therapy
Step 3 involves a combination of steps 1 and 2. There is some evidence that a combination of sumatriptan 50mg and naproxen 500mg is superior to either drug alone. (Smith and Sunshine, 2005). The National Institute for Health and Clinical Excellence (NICE) advise offering combination therapy with a triptan and NSAID, or a triptan and paracetamol (National Clinical Guideline Centre (NCGC), 2012).
It should be noted that there is a risk of medication overuse headache with NSAID or paracetamol use in more than 10 days in a month, and with triptan use in over 15 days per month. Use of analgesia on 2 or more days of the week should alert prescribers to discuss with the patient and, sometimes, review the diagnosis.
Emergency treatment
In severe attacks, intramuscular (IM) diclofenac 75mg with or without 12.5mg of IM prochlorperazine may be administered. Alternative anti-emetics include IM chlorpromazine 25–50mg and IM metoclopramide 10–20mg. Subcutaneous sumatriptan at a 6-mg dose is fast acting and can be administered together with these other medications. Consider carrying these medications for home visits. Dehydrated patients require hospital admission (Simon, O’Reilly, Proctor and Buckmaster, 2007; BASH, 2010), as do those suffering from severe, uncontrolled status migrainosus (migraine lasting for over 72 hours) (Prodigy clinical topics, 2010a).
Prophylaxis
The aim of prophylaxis is to reduce the number of migraine attacks in which appropriate acute treatment gives inadequate control. There is no definitive rule; the best judge of inadequacy of control is usually the patient. Prophylactic treatment may be recommended if the patient suffers from more than two migraines per month that result in significant disruption to daily activities, or less frequent but severe migraine attacks. It may also be considered if there has been a poor response to acute treatment or an inability to tolerate it due to side-effects or contraindications. Finally, prophylaxis may be appropriate if the frequency of the need for acute medication is suspected to contribute to medication overuse headache. Most of the medications used for migraine prophylaxis are not licensed for use during pregnancy. This should be discussed with women of childbearing age, and the need for contraception considered.
On initiation, titrate the dose of all prophylactic agents slowly to an effective or maximum dose to reduce side-effects. As prophylactic mediations may be slow to take effect, a minimum trial of 6–8 weeks should be undertaken following dose titration. Because the pattern of migraine exacerbations tends to fluctuate, it is inappropriate to continue prophylaxis indefinitely; effective drugs should be continued for 6–12 months prior to considering withdrawal. On withdrawal, the dose should be tapered over 2–3 weeks (SIGN, 2008; BASH, 2010).
First-line agents
First-line prophylaxis includes beta-blockers and amitriptyline. A non-cardio-selective beta-blocker (propranolol) is a good choice if the patient has co-existing anxiety or stress. However, it should be avoided if there are contraindications such as asthma, chronic obstructive pulmonary disease (COPD), uncontrolled heart failure and peripheral vascular disease. The usual recommended dose of propranolol is 40mg twice daily, but 10mg three times a day may be sufficient. Cardio-selective beta-blockers have an improved side-effect profile and include atenolol 25–100mg twice daily (unlicensed indication) or metoprolol 50–100mg twice daily. Bisoprolol 5–10mg (unlicensed indication) is another alternative that only requires once daily dosing, thus is associated with better compliance. Frequent side-effects include cold extremities, reduced exercise tolerance and dizziness (BASH, 2010). Overall, it may be sensible to use a cardio-selective beta-blocker in view of the more favourable side-effect profile and improved compliance.
Amitriptyline at a dose of 10–150mg taken 1–2 hours before bedtime is appropriate when migraine co-exists with tension-type headache, another chronic pain condition, disturbed sleep or depression. The dose should be titrated slowly. Frequent adverse effects include the anticholinergic symptoms of dry mouth, sedation, dizziness and nausea. They are often most apparent during the first 2 weeks and tend to settle with continued use (BASH, 2010).
Beta-blockers and amitriptyline can be used together. A synergistic effect has been suggested, although there is no formal evidence for this (SIGN, 2008).
Second-line agents
Second-line agents include sodium valproate and topiramate. These should be initiated in secondary care, so consider a referral to a neurologist if first-line medications are ineffective or contraindicated (see ‘Criteria for referral to secondary care’). They both have similar efficacy. Sodium valproate does not limit the effectiveness of the oral contraceptive pill (OCP) but topiramate does, as it is a liver enzyme inducer (thus causes faster metabolism of the OCP, so reducing its efficacy). Both drugs are contraindicated in pregnancy (BASH, 2010).
Clinical experience in migraine is currently greater with sodium valproate compared with topiramate. The recommended dose of sodium valproate is 0.3–1g twice daily. Adverse effects include nausea, asthenia, somnolence, weight gain and alopecia. About half of patients taking topiramate complain of paraesthesia that usually improves with continued use. Approximately a quarter report anorexia and weight loss, and a similar number experience some degree of cognitive dysfunction (BASH, 2010).
Third-line agents
Third-line agents also tend to be initiated in secondary care. They include gabapentin and methysergide, although the evidence for efficacy of the former is weak and gabapentin may be used as a drug of abuse. Methysergide is very effective but should be held in reserve due to difficulty weaning from the drug and its association with retroperitoneal and pleural fibrosis (BASH, 2010).
Pizotifen and clonidine have been used with limited evidence of efficacy. Pizotifen may also be problematic due to unwanted effects of weight gain and somnolence.
In 2010, the Medicines and Healthcare products Regulatory Agency (MHRA) licensed the use of botulinum toxin injections for migraine prophylaxis. However, evidence for the efficacy of this treatment has not been established and its place in migraine management is as yet unclear (Cady and Schreiber, 2008).
Management of menstrual migraine
Menstrual migraine is defined as a migraine starting at any time from 2 days before to 3 days after day 1 of menstruation, repeated over a number of cycles. It is thought to be caused by the pre-menstrual fall in oestrogen. There are two patterns of menstrual migraine:
Pure menstrual migraine is when migraine exclusively occurs around periods.
Menstrual-associated migraine is when migraine occurs both around menstruation and at other times; this is more common than pure menstrual migraine.
It is very important to ascertain whether the migraine is associated with aura, and whether certain types of oestrogen-containing contraception have been used. Oestrogen-based contraception [e.g. the combined oral contraceptive pill (COCP)] is contraindicated in patients who have migraine with aura. Moreover, if a woman develops migraine with aura at any age, or migraine without aura over the age of 35 years, following the use of oestrogen-based hormonal contraception, it should be immediately withdrawn due to the increased risk of a cerebrovascular accident [Faculty of Sexual and Reproductive Healthcare (FSRH), 2009]. However, if migraine without aura occurs around the pill- or patch-free interval (when oestrogen levels decrease), then management should involve oestrogen replacement.
Non-hormonal treatment
Non-hormonal methods of treatment can be considered if the woman does not require contraception or if hormonal contraception is contraindicated. Non-hormonal medication can be used as described in the section on acute treatment of migraine, earlier in this article. NSAIDs can be started in anticipation of the migraine, a few days before the onset, until the last day of menstruation. Mefenamic acid is a good option to treat both dysmenorrhoea and migraine. Triptans can also be used in anticipation, starting 2 days before the expected onset of migraine. The greatest evidence of efficacy is for frovatriptan (BASH, 2010).
Hormonal treatment
Hormonal medication for menstrual migraine can be used to either supplement the oestrogen levels pre-menstrually or inhibit ovulation. Oestrogen-containing preparations may be used in women under the age of 35 years who have never experienced migraine with aura. One option is the use of oestrogen supplements prescribed in the form of a transdermal oestrogen patch (100 mcg, or 50 mcg if not tolerated), from 3 days before the onset of menstruation. Alternatively, 1.5mg of oestradiol gel (two measures of Oestrogel) can be applied daily over the same time period. The gel is thought to produce higher, more stable levels of oestrogen (BASH, 2010). All oestrogen supplements should only be used in women who menstruate regularly (as these women will have innate progesterone opposition), and it is important to note that their use for migraine treatment is an unlicensed indication.
If the woman is happy to receive contraception, a variety of options can be offered. The COCP, desogestrel-containing progesterone-only pill (POP), the contraceptive implant and the contraceptive depot injection all inhibit ovulation, so can be beneficial in menstrual migraine. POPs other than the desogestrel-containing POP do not inhibit ovulation so are not recommended for the management of menstrual migraine. The progesterone-only methods (desogestrel-containing POP, depot or implant) are all suitable for women in whom oestrogens are contraindicated. As the levels of oestrogen can fluctuate with the COCP, ‘tricycling’ (continuous use for 9–12 weeks) with a monophasic pill (e.g. Microgynon) can be attempted (BASH, 2010).
Migraine associated with combined hormonal contraception
Combined contraception is contraindicated in women with a history of migraine with aura, or migraine without aura over the age of 35 years. However, if the patient does not meet these criteria, and experiences migraine during the COCP- or patch-free week (when the levels of oestrogen are reduced), the following measures could be tried:
Changing to a COCP with a different progestogen, or lower dose of the same progestogen.
Using oestrogen supplements in the form of a patch or gel (as described for menstrual migraine) during the pill- or patch-free week.
Tri-cycling three packets of a monophasic COCP.
Reducing the fluctuation of hormone levels by changing to a type of hormonal contraception that inhibits ovulation.
Migraine and hormone replacement therapy
The menopause can exacerbate migraine but symptoms may be relieved with optimised hormone replacement therapy (HRT). HRT is not contraindicated in migraine sufferers (with or without aura). However, some women on HRT experience worsened migraines, which may be managed by altering the formulation or dose (BASH, 2010). Both the oestrogen and progestogen component of HRT can exacerbate migraine. If a woman is using cyclical HRT the hormone at fault can be determined by establishing whether symptoms occur in the purely oestrogen phase, or the phase in which progestogens are added. Changing the type, reducing the dose, or altering the route of delivery of either the progestogen component or the oestrogen component may help. If a woman is on a cyclical preparation the number of days of progestogen in the cycle can be reduced but must be given for a minimum of 12 days to protect the endometrium.
If migraine is associated with oestrogen withdrawal (again, with cyclical HRT), then a continuous preparation could be considered when a year or more has passed since the woman's last period. HRT patches provide more stable oestrogen levels than tablets so these should be considered.
Migraine occurring for the first time in a middle-aged woman is unusual. If migraine occurs after starting HRT, then the HRT should be stopped and the cause investigated. If aura develops for the first time in a woman taking HRT who previously suffered from migraine without aura, then a dose reduction of the oestrogen component could be tried. If the aura continues in spite of this, the HRT should be stopped.
Management of migraine in pregnant and breastfeeding women
Most women with migraine find that their condition improves during pregnancy, although a small proportion report that it worsens. Drug treatment should be limited in pregnancy if possible and, if used, the lowest effective dose should be prescribed for the shortest time.
For pain relief, paracetamol is safe throughout pregnancy. Ibuprofen should be avoided in the third trimester, and its use earlier in pregnancy is also not ideal. Aspirin should be avoided during early pregnancy and the third trimester. Triptans are contraindicated in pregnancy. For nausea and vomiting, cyclizine is recommended as first line. Metoclopramide can be considered if this is ineffective (but should be avoided in women under 20 years of age, due to the increased risk of dystonic reactions).
Paracetamol is safe during breastfeeding and ibuprofen may be used with caution. Aspirin should be avoided completely. Nausea and vomiting can be treated as recommended in pregnancy. Triptans can be used in breastfeeding women, as long as milk is expressed and discarded for 12–24 hours after the dose.
Prophylactic treatment is not recommended in pregnant or breastfeeding women. If a patient is particularly troubled and prophylaxis is deemed necessary a neurology referral should be made (see Box 1) (Prodigy clinical topics, 2010b; BNF, 2012).
Non-drug interventions
Stress is an important trigger factor for migraine and prophylactic drug treatments may be inadequate unless this problem is addressed. It is important to acknowledge that as migraines can be so debilitating, they can be a cause of stress, low mood and reduced quality of life in their own right. Stress or anxiety management should be used as a first-line intervention if indicated, or as an adjunct to drug treatment.
Suitable non-drug interventions, that may also help to manage stress, include cognitive behavioural therapy, aerobic exercise and relaxation therapy. Physiotherapy to the neck may help if muscle tension co-exists with migraine. The BASH guidelines state that improving physical fitness might reduce migraine susceptibility, although there is insufficient evidence to recommend for or against aerobic exercise for prophylaxis (NCGC, 2012; BASH, 2010). Acupuncture may provide some benefit, but the value of hypnotherapy is unproven and homeopathy appears to be of no value (BASH, 2010).
Criteria for referral to secondary care
Referral to secondary care may sometimes be necessary either at the initial presentation of suspected migraine or later during the course of management. Early referral may be required if the diagnosis is uncertain, the migraine is particularly severe, or if it is associated with complicated features. Consider referral in cases involving evolution of unusual features, red flag features, or poor response to primary care treatment. Box 1 lists the main indications for referral to secondary care.
Indications for referral to secondary care
Indications for referral to a neurologist
The diagnosis of migraine is uncertain.
Migraine occurs in over 15 days per month (consider medication overuse headache).
Maximum treatment in primary care (for either acute attacks or prophylaxis) is insufficient.
Indications for acute admission
The migraine has complicated features, for example, persisting aura lasting for longer than an hour or migraine-triggered seizure.
The patient is suffering from severe, uncontrolled status migrainosus.
Adapted from Prodigy clinical topics, 2010c.
Key points
It is important to address trigger factors for a patient's migraine prior to considering medication.
Use medical management of acute migraine in a stepwise manner, starting with simple analgesia.
Prior to stepping up treatment assess adherence to medication and also review the diagnosis; GPs should be vigilant to the possibility of migraine being complicated by medication overuse headache.
Triptans are recommended for acute migraine attacks, only if first-line treatment is inadequate.
Menstrual migraine can be managed using hormonal and non-hormonal methods.
Footnotes
Acknowledgements
We would like to thank Dr Emma Harris for her help with the writing of this article under the InnovAiT ‘buddy’ scheme.