
Abstract
Homelessness takes a wide variety of forms but homeless people are among the most vulnerable and excluded in society. They have much higher rates of physical and mental illness and premature death than the general population, yet are less likely to be registered with a GP. This article aims to explore the reasons behind this, the specific health needs of homeless people and the role of general practice in their care.
The GP curriculum and health needs of the homeless
The interrelationships between health and social care including the wider determinants of health within communities, e.g. housing, employment and education
The impact of poverty, genetics, ethnicity and local epidemiology on an individual and a local community's health
The impact of inequalities and discrimination on health
The inequalities in health care provision: the ‘inverse care law’
Who are the homeless?
Homelessness in the UK is a largely invisible problem, with the occasional rough sleeper representing a tiny minority of those without secure accommodation. There are many more ‘hidden homeless', such as those staying in emergency hostels, women's refuges and temporary housing, who are not ’roofless' but do not have any permanent accommodation. Others will be living in overcrowded or insecure accommodation, such as staying temporarily with friends or family, squatting or as part of a travelling community.
Risk factors for becoming homeless.
It is becoming increasingly clear that being homeless is associated with a significant increase in levels of poor health and premature death. The statistics are startling: the average age of death for homeless patients in the UK is between 40 and 44 years (Department of Health, 2010a,b). A recent study of homeless patients admitted to hospital with drug-related problems in Glasgow found that they were seven times more likely to die over the next 5 years than housed patients with the same reason for admission (Morrison, 2009). Poor health among homeless people has implications both for those individuals and for the health of the local community.
The scale of the problem
Quantifying the scale of homelessness in the UK is difficult and estimates vary. A recent Department of Health report estimated that there are 40 500 people living in hostels or supported accommodation at any one time. This underestimates the overall homeless population as it will not include those in other forms of accommodation. In 2010, 61 000 individuals in UK were officially recognised as being newly homeless. This figure excludes those deemed to have made themselves intentionally homeless and the many others who do not report themselves as homeless to the council in the first instance. There are marked geographical variations in the proportion of the population registered as homeless (Fig. 1).
While some people only experience homelessness once, more commonly people experience multiple episodes of homelessness. This often occurs when a person who is homeless is provided with a tenancy but then loses it again, known as the ‘revolving door’ of homelessness. This may occur for multiple reasons, such as repeatedly committing criminal offences resulting in a custodial sentence or defaulting on rent payments because of substance misuse and mental health problems. In 2003 Crisis, a national charity supporting homeless people estimated that each failed tenancy cost local authorities between £1400 and £4000. Tenancy support or probation schemes aiming to help people maintain their tenancies are vital; these are often provided by third sector organisations.
The role of the housing authority
Local authorities have a statutory duty to provide emergency accommodation to those who are deemed to be unintentionally homeless and ‘in priority need’. Being in priority need is defined as being more likely to suffer harm as the result of being homeless than an ordinary homeless person. Legislation exists defining specific groups this applies to: among them are pregnant women, those with dependent children and certain care leavers. Those deemed vulnerable as a result of old age, disability or mental or physical illness are also included but this is subject to an assessment of how such conditions affect the likely impact of being homeless on them.
Number of individuals in hostel accommodation per capita by PCT.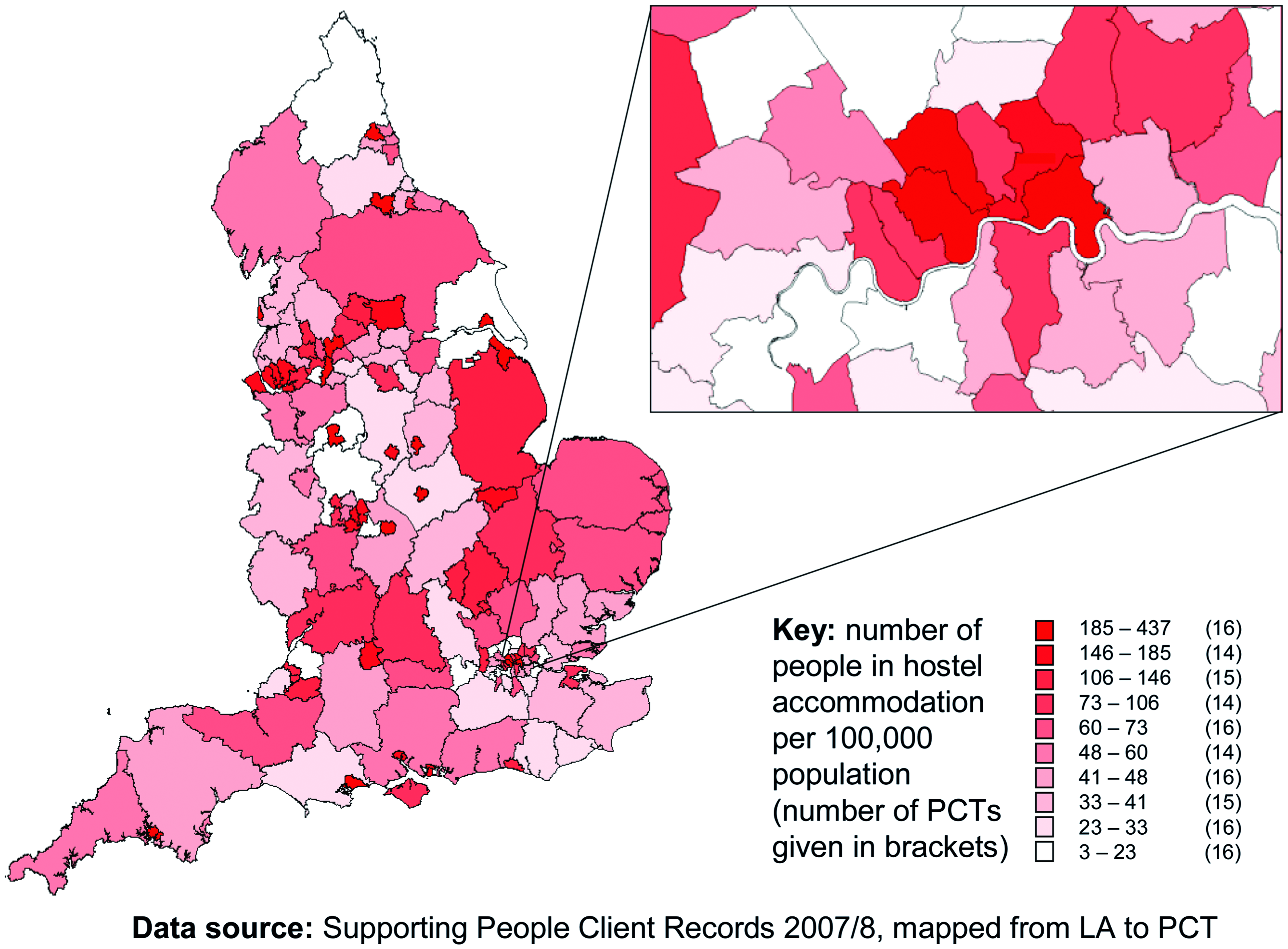
People are defined as becoming homeless ‘intentionally’ if they have to leave their home because of deliberate action or inaction on their part. This includes failing to pay the rent when they had the means to do so, antisocial behaviour that results in eviction or declining a flat that is offered to them by the council. In practice, those classed as making themselves ‘intentionally homeless’ are entitled to little support from the local housing authority.
Access to health care
Many homeless people will suffer from a triad of poor physical health, mental health and substance misuse. A chaotic lifestyle may then mean that significant health needs are exacerbated by difficulties accessing health care, particularly primary care.
A survey by the Big Issue found that only 71% of vendors were registered with a GP compared with 98% of the general population. Other earlier studies, looking specifically at rough sleepers, found lower rates of registration with a GP ranging from 35 to 66% (Pleace et al., 1999). Potential barriers include administrative requirements such as practices requiring proof of addresses or the tendency for such patients to ignore their health needs in the light of more immediate needs. A chaotic lifestyle may make it very difficult for homeless patients to make and keep appointments or comply with self-care advice. They may be registered as temporary patients and therefore not included in health promotion activity such as cervical screening.
Another major barrier cited in surveys of homeless patients is the attitude of health care staff towards them. Both GPs and hospital doctors have also been reported as being concerned that homeless people might prove to be challenging and difficult and that their presence might make visiting the doctor difficult for other patients (Pleace et al., 1999). In a study of homeless patients, 54% quoted negative attitudes of health care workers as the reason they did not go to a hospital or GP regarding a health problem (Thomson, 2003; cited in Quilgars et al., 2003).
Homeless patients' use of acute and secondary care appears to be disproportionately high, perhaps due to these difficulties. For instance, a Department of Health report found homeless people used an estimated eight times more hospital inpatient services than an average person of similar age. Comparison of data from a GP practice for homeless patients in Leicester with neighbouring practices showed a six times higher Accident and Emergency Department attendance rate, with homeless patients being four times as likely to be admitted. National hospital data looking at patients who gave their address as ‘No Fixed Abode’ demonstrated an average length of stay almost triple that of the general population of the same age. Analysis by the Office of the Chief Analyst found that these differences were largely accounted for by the difference in case mix and so were not due to discharge difficulties: the homeless patients stayed longer because they were more unwell.
Over-utilisation of acute and emergency care is costly for the health service and disadvantageous for homeless patients. Such services are not well placed to provide long-term holistic care for the health needs of such patients nor to offer continuity in the patient-practitioner relationship. There are clearly strong arguments to strive to ensure better access to primary care for homeless patients.
Extracts from the 2002 RCGP Statement on Homelessness and Primary Care.
Models of primary care for the homeless
How should effective primary care for the homeless be provided? There are a wide variety of models within the UK. A key debate is whether it is more effective to integrate homeless care into mainstream primary care or use specialist outreach teams and services. The first option reduces stigma but may make accessing the full range of services required more difficult in a group of patients who already struggle with access. However, the concentration of homeless patients outside major cities is unlikely to be sufficient to justify the additional expense of a specialist service.
An analysis in 2007 showed that two-thirds of Primary Care Trusts (PCTs) did provide some form of specialist primary care service (Fig. 2). Innovative solutions range from ‘one stop’ services where help with health care and substance misuse and housing is available in the same building, to a ‘TB Van’ in London that visits hostels and prisons and can provide counselling and a chest X-ray for those at risk of tuberculosis (TB). Projects aiming to blur traditional boundaries between primary and secondary care are also being trialed, such as a 10-bedded intermediate care facility in a large London hostel. Another project in London aims to improve hospital discharge planning by including a GP, a nurse and a person with personal experience of homelessness on hospital ward rounds (Hewett, 2010). Early results from this scheme suggest that it is providing overall savings by reducing the number of patients with prolonged durations of stay.
Health inequalities and social exclusion
People who are homeless are one of many groups within society where social exclusion and deprivation are correlated with poorer health outcomes. For example, people living in the UK in the poorest neighbourhoods will, on average, die 7 years earlier than those living in the richest neighbourhoods (Office for National Statistics, 2009; cited in Marmot, 2010). Such ‘health inequalities’ have been recognised by GPs and public health teams for years. These differences are not only to do with differences in health behaviours but also in the availability of medical care and the way people access it. This was described 40 years ago by Julian Tudor Hart as the ‘inverse care law’ – that ‘the availability of good medical care tends to vary inversely with the need for it in the population served’. More recently, there has been an increasing focus by the government and Department of Health on how to tackle health inequalities.
Provision of specialist homeless primary care services by PCT.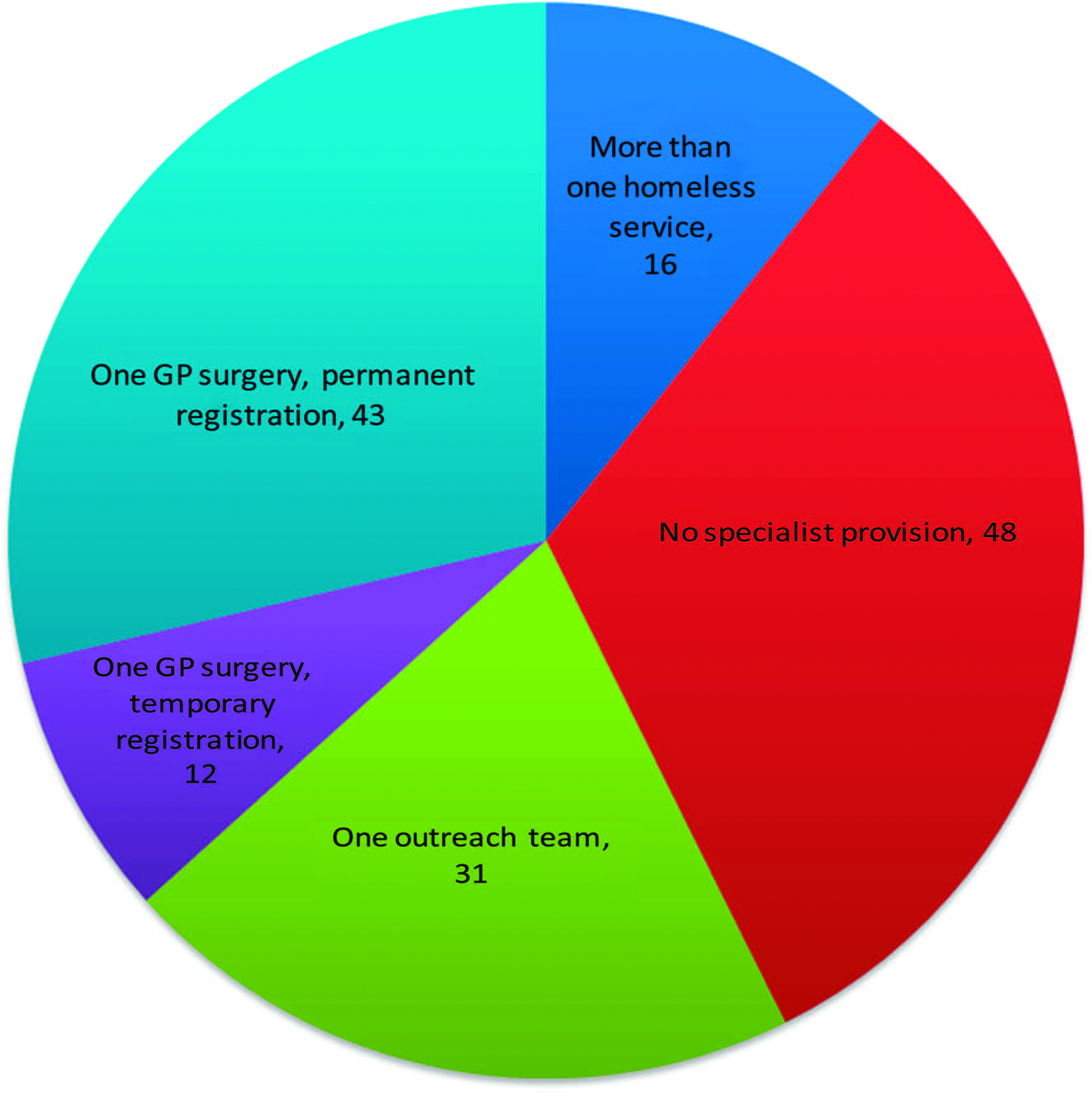
A key policy document in this debate was the Marmot Review, published in March 2010. This proposed ‘proportionate universalism’ – helping all sections of society ‘but with a scale and intensity that is proportionate to the level of disadvantage’. This raised the prospect of targeted investment in the health of deprived groups.
At around the same time as the Marmot Review, a Cabinet Office Task Force project, ‘Inclusion Health’ described the health inequalities affecting particular socially excluded groups such as travellers, sex workers, prisoners and the homeless. The project report argues that improving the health of such groups makes sense not just ethically but also economically, given the high costs of unscheduled care. This resulted in the creation of a Health Inclusion Board, chaired by Steve Field (previous chair of the RCGP), who described its role as being to ‘champion the cause of people who are vulnerable and socially excluded, such as the homeless and street sex workers’.
At the same time, a report on ‘Health Needs of Single Homeless People’ was published by the Department of Health. This went into further detail exploring the health problems commonly experienced by homeless patients and estimating the costs generated by their in-patient care.
All these are encouraging developments. However, it remains to be seen whether such documents will translate into positive decisions by commissioners to allocate the necessary creativity energy and resources towards improving primary care for the homeless.
Health problems among homeless patients
A large number of studies in both the UK and internationally have confirmed that the incidence of both physical and mental health problems is markedly higher among the homeless. Some care is needed in interpreting such results: ill-health may not only result from homelessness but may also have caused the person to become homeless in the first place. Expert opinion from the Royal College of Physicians suggests around two-thirds of serious chronic health problems among the homeless will have existed prior to them becoming homeless. Often, such problems will be exacerbated by the environmental and psychological stress of becoming homeless.
Physical health problems
Health problems commonly found among homeless people.

Mental health
Psychological disorders have been found to strongly predict homelessness and in particular rough sleeping (Maguire et al., 2009). A large number of studies have recorded high rates of depression, schizophrenia, alcohol dependence and head injury among the homeless (Spence et al., 2004). These rates are markedly higher among rough sleepers, with as many as 50–75% having Axis I disorders (anxiety disorders, depression, dementia and psychosis disorders) and 30% having schizophrenia.
However, engaging such patients with treatment may be very difficult: in one review, less than one-third of homeless people with mental illness actually received treatment (Bines, 1994). Often, a more proactive outreach approach to their care is required and in some areas, this has led to the creation of specialist Homeless Psychiatry Teams. These have the advantage of flexibility: the team in Sheffield has consulted patients in a wide range of places including hostels, squats, police stations, public houses, cathedrals, snooker halls, stairwells and railway sidings (Spence, 2009).
Studies also suggest a higher proportion of homeless people with global cognitive deficit or reduced Mini Mental State Examination scores up to 30–40% in some studies compared to 2–3% among the general adult population (Spence et al., 2004). Affected individuals are likely to find it more difficult to use services, retain accommodation and reintegrate into local communities. This needs to be recognised and taken into account when planning their care.
Substance misuse
Levels of substance misuse and alcohol dependence among homeless populations are high. Use of more than one drug, particularly heroin together with cocaine, is common. A large survey of homeless people in London found that rates increased the longer people had been homeless: 39% of those who had been homeless for 2 years or less had used heroin in the last month, whereas 49% who had been homeless for 10 years or more had used heroin in the last month. Four of five responders reported starting taking at least one new drug since becoming homeless (Fountain and Howes, 2002).
Approximately 20% of homeless people with mental health problems also have a concurrent diagnosis of substance dependence (‘dual diagnosis’). In some cases, the substance misused may be a contributory factor to the mental health problem (for instance, alcohol to depression, or cannabis to psychosis); in other cases, it may be a consequence (for instance, drinking heavily to self-medicate for anxiety).
How can a GP contribute towards homeless health?
Homeless patients are not a homogenous group. They will come with individual health needs that need to be explored and addressed in the same way as for any other patient. However, there are a few areas where knowing someone is homeless might alter a GP's approach.
Prevention of homelessness
Online resources for clinicians and patients.
Screening for mental health problems
Screening for low mood or anxiety in patients who are homeless is often revealing. Given the high levels of alcohol dependence and substance misuse, asking specifically about these is highly relevant.
Care is needed with prescribing. Given the high rates of death from overdose among homeless people, benzodiazepines, hypnotics and tricyclic antidepressants should be used with caution. People may present requesting a repeat prescription of medication issued at their previous GP practice or by another service. Avoiding dual prescribing by confirming this directly with the other agencies involved is important.
Addressing alcohol use
Screening for harmful drinking or alcohol dependence can provide an opportunity for education and brief interventions or referral to specialist alcohol services. Prescribing vitamin B and thiamine supplements to those with chronic alcohol dependence reduces the risk of alcoholic neuropathy and Wernicke's encephalopathy.
Substance misuse: harm reduction and substitute prescribing
Safe opioid medication substitute prescribing (e.g. of methadone or buprenorphine) is evidence based. In the context of an agreed treatment plan and support from a drug worker, it has been shown to reduce crime and drug use (Wright and Tompkins, 2006). For those not ready to consider substitute prescriptions, local drug services should offer harm reduction advice around safe injecting practice and risks of inadvertent overdose. Needle exchange schemes usually offer provision of syringes, water, sterile filters and spoons/cookers, thus reducing one of the main reasons for high rates of Hepatitis C among homeless drug users.
Offering appropriate vaccinations
Providing tetanus, influenza, pneumococcus, diphtheria and hepatitis A and B vaccinations for those living in hostels is recommended. An accelerated schedule of hepatitis B vaccinations at 0, 7 and 21 days, with a booster at 12 months has been shown to significantly improve the proportion of people who complete the course (Wright et al., 2002).
Sexual health screening
There is little research into the prevalence of sexually transmitted infections among homeless patients. A narrative review looking at street youth and drug users concluded that most were sexually active and that there was a high rate of partner turnover, with sex often being exchanged for drugs or money (Van Den Hoek, 1997). Asking about sexual health and contraceptive needs and offering education, screening and contraception as appropriate is important. Women with particularly chaotic lifestyles may struggle to remember to take daily contraceptive pills so remember to offer longer acting reversible methods as a more reliable alternative.
Advocacy
The GP also has a vital role in advocacy for those who are at particular risk from being homeless; for instance, those with a history of major mental illness who may be provoked into a relapse of their psychosis by being homeless. In such cases, providing a letter detailing their medical history and particular reasons that they might be deemed vulnerable may help them to be labelled ‘in priority need’ of housing by the local housing authorities.
Affirmation
Homeless patients often have poor self-esteem or a learnt distrust of authority figures. Those sleeping rough may be unkempt or smell; they may appear at the surgery either under the influence of or withdrawing from drugs and/or alcohol. Such patients provide unique challenges to our consultation skills. Sadly most are used to being ignored or treated with contempt; rough sleepers often report being beaten up or urinated on by passers by. The GP consultation provides a brief but significant opportunity to affirm their value and dignity as people. Building trust by treating them with respect and kindness within the consultation is vital if they are to engage with healthcare staff both now and in the future.
Key points
Being homeless is associated with a much increased risk of poor physical and mental health and higher rates of alcohol and substance misuse; this may be both a cause and a consequence of homelessness Homeless people may struggle to access conventional healthcare; GPs can improve homeless health by making appropriate and high quality primary health care more accessible Appropriate health care for homeless patients includes screening for mental health and substance misuse problems and providing preventative interventions such as vaccinations GPs also have a role in preventing homelessness by signposting patients whose housing is at risk to relevant agencies Ensuring access to primary care for the homeless will require change at many levels, from the individual attitudes and consultation skills of each GP to practice policies and local and national priorities